I think these headlines, possibly purposefully, overlook the possibility that vaccine antibodies eased acquisition of infection induced antibodies to the point of being subclinical events.
That is, a vaccinated person could be exposed to a variant for which they are partially protected, not notice clinical symptoms, while the person's immune system still remembers the details of the variant.
As an iterative process, this is akin to software updates (for a running immune system).
So to say that variant A.30 isn't covered by the mRNA induced spike protein antibodies is a very different statement than to say it's able to evade an immune system primed by mRNA antibodies which then re-entered daily life and thereby was able to continuously adapt to variants.
It's also worth noting that the most people still had antibodies effective against A.30-- just not as effective. So the existing antibody response would be expected to slow infection and then the body is primed to broaden the variety and quantity of antibodies after infection.
It's only a small portion of those receiving the AZ vaccine whose serum had no significant activity against A.30-- all of those with the mRNA vaccine did and most of those receiving AZ did.
> It's only a small portion of those receiving the AZ vaccine whose serum had no significant activity against A.30-- all of those with the mRNA vaccine did and most of those receiving AZ did.
How about those that received no vaccine, but have previously recovered from Covid? Is it an insignificant number because I rarely hear it discussed.
I think it is due to politics that you don't hear this discussed; seemingly, nuance makes it more difficult to convey a message. The number of people who are known to have been infected is not insignificant, and the number who have been infected but it isn't known is much higher. (I thought estimated were that at least 4x as many people have had Covid as show up in the published results).
There is every reason to expect that natural immunity (derived from a previous infection) is better (than that conferred by a vaccine), simply because the immune system will recognize the entire virus and not just the spike cell.
"This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant."
If having pre-delta covid made it more likely that your immune system could face delta, then I think it would stand true for other variants, too.
> There is every reason to expect that natural immunity (derived from a previous infection) is better (than that conferred by a vaccine), simply because the immune system will recognize the entire virus and not just the spike cell.
No - we do not have "every reason" to expect, quite the opposite. As a starter, for many infectious diseases (incl. viral diseases) vaccine-induced immunity is better, see e.g. the commentary and examples here [1].
Regarding SARS-CoV-2, the picture is a lot more subtle. Directly from German virologist Christian Drosten:
"If you look closely at the data in the studies, the situation is much more complicated. What one should say and be aware of is vaccination, which provides a relatively constant protection, which is very well described in studies. You actually pretty much know what you have. While there is a greater spread in the case of infection. Quite simply, we get different amounts of virus in the infection. Some have a silent infection that they don't even notice, others have a symptomatic infection. And you have to be aware that in such studies, which are primarily based on PCR test results, there will always be a certain emphasis on symptomatic courses. That means saying that if I know I have survived an infection and it was confirmed by PCR testing, then that also implies that I had symptoms, otherwise I would hardly have had a PCR test at the time. So then I had a symptomatic course. I think that for this situation you can now say very well, whoever had the whole thing symptomatically, will be well protected afterwards, almost like a vaccination." [2]
The study you picked in its current pre-print form does not adequately address this obvious selection bias, nor does it address the inherent survivorship bias. I´m not a medical expert though, so we will see if it passes peer review.
In any case, please do not perpetuate the myth that natural immunity is superior per se. If you had a symptomatic infection plus a PCR test, you are likely well protected, very similar to (mRNA) vaccination. If your infection is more than 6 months old, get a booster.
Can you link to studies mentioned in your quote ? - "If you look closely at the data in the studies, [..]"
Also, you seem to be rightfully cautious that the situation is fluid, but also calling natural immunity being better a 'myth'. This may just be the word you chose, but myth to me is something that is complete BS. Are you also intending to use it that way?
I chose myth to describe the pattern of something that seems correct for seemingly obvious reasons but is actually incorrect for more complicated reasons.
In particular the black and white belief that natural immunity is superior because
a) it is 'natural' (this is a such a great example of extrapolating from a kernel of truth and can have interesting notions packed into it, like the superiority of divine creation and/or nature),
b) the vaccine only encodes the spike protein (one of the reasons the spike protein was chosen is because it is more robust w.r.t. to variation relative to other components of the virus).
I see these "arguments" often politicised with terms such as 'gold standard immunity'.
Your claim that natural immunity superiority is a myth is based on which scientific principles? Please throw all the science you can at me, I am genuinely interested.
Also, I'm curious if you read the studies you're linking to?
This is literally the conclusion from link #8
>This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.
Please re-read what I wrote: It's BS to call natural immunity superior for the reasons of being "natural" or because "vaccines only encode the spike protein".
There is no black and white argument why natural immunity should be superior - it can be worse, similar or better than vaccine-induced immunity. It all depends on the amount of viral particles you were exposed to in the first place.
Any study that compares natural immunity to vaccine-induced has to deal with a selection bias (as stated in the quote by somebody who is a professional at designing such studies).
>There is no black and white argument why natural immunity should be superior - it can be worse, similar or better than vaccine-induced immunity. It all depends on the amount of viral particles you were exposed to in the first place.
Logical arguments for a position don't equate to empirical truths. Data is preferred over argument/opinion.
>Any study that compares natural immunity to vaccine-induced has to deal with a selection bias (as stated in the quote by somebody who is a professional at designing such studies).
Do you have any evidence that the study you linked to is biased? If so, why even link to it?
In any case, I think this thread is not going anywhere, so I will just let you have the last word.
I also wonder whether the reason the "natural vs vaccine" immunity question may not have a great, direct answer is it wasn't asked until covid-19.
When I was asked about this by a 'vaccine skeptic', I said having the vaccine after an infection was clearly a huge benefit over having just the vaccine or just the infection - so do it. I've also seen a study where the super rare, problematic responses to the vaccine seemed to be the same symptoms someone would experience with an infection sans the vaccine - only the effect would be dramatically worse with an infection. (Sorry I can't offer sources at the moment - moments from sleep.)
Of course it was asked before COVID-19: there's no point in taking a vaccine for a disease you already had because the vaccine is not more virus-like than the virus itself. By definition there is no event closer to infection than infection; for the body, a vaccine is always a trial run. Hence things like chickenpox parties. There wasn't raging debate about this because it's obvious and uncontested.
It's quite sad to see people now claiming it's some kind of novel scientific question about natural immunity vs not. This is basic, high school level biology. It's not advanced stuff and the people claiming otherwise are invariably using bad science to do so. For example, claims that infection doesn't stop reinfection are often based on studies with so few cases of reinfection that it'd fall below the noise floor for almost any testing system. The belief that these events are real relies on yet more bad science (the belief that mass testing has an FP rate of zero).
The reality is that natural immunity is suddenly being questioned because "vaccine zealots" are desperate to suppress any messaging that might discourage people from taking it. They've lost all perspective, which means they're making claims that are contradicting biology considered so basic and important that it's literally taught to children in school. Then they sit around looking confused, wondering why suddenly so many "anti-vaxxers" and "skeptics" came out of the woodwork.
> By definition there is no event closer to infection than infection [...] Hence things like chickenpox parties.
Glad you mention chickenpox. Could you help me understand why the protein vaccine is much more effective than the attenuated virus vaccine? Following your argument there should be nothing better than the virus vaccine, because it is closest to infection?
It's not more effective, is it? The mRNA vaccines have proven to have zero efficacy after only a few months, at least for the goal they were judged against in the trials. They don't reduce the rate of infection at all. Even Boris Johnson has admitted that now.
Actually it is good to be vaccinated even if you have already had a disease. This confers greater immunity than the infection or just the vaccine.
Whether or not the vaccine or natural immunity is better protection isn't as clear as suggested either, generally the vaccines will give more reliable resistance.
"Natural immunity can be spotty. Some people can react vigorously and get a great antibody response. Other people don't get such a great response," says infectious diseases expert Mark Rupp, MD. "Clearly, vaccine-induced immunity is more standardized and can be longer-lasting."
No it isn't. That's extremely bad advice, please don't tell people to get vaccinated if they don't need to. The vaccines can have nasty side effects and if you've had the disease you are hardly at any risk of being reinfected, let alone actually suffering disease. The data on this is quite clear, there are many studies that look at the testing data to find this.
"Out of 149,735 individuals with a documented positive PCR test between March 2020 and January 2021, 154 had two positive PCR tests at least 100 days apart, reflecting a reinfection proportion of 1 per 1000"
So that's really incredibly low. Note that this paper, like so many others, assumes a false positive rate of zero: with such a low number of reinfections they could easily just be testing errors and thus the reinfection rate can easily be even lower still.
Remember - COVID is a mild disease for the vast majority. Having been infected reduces your chance of infection so low that it takes you from a very low chance of having serious problems to "you need scientific notation to express the probability of having problems". Vaccines can only make things worse for those people, not better.
Unfortunately our society has completely lost all rationality over vaccines. Your so-called infectious disease expert is a great example of that. Firstly, he's dead wrong that vaccine-induced immunity is longer lasting. It lasts months at most, which is why even vaccine-pushers have given up claiming it stops you getting COVID. And antibody titers are not the end goal here! The goal is to avoid getting sick. They've completely substituted the means for the end, which is the sort of contempt-worthy irrationality that makes people reject the vaccination programme.
> The vaccines can have nasty side effects and if you've had the disease you are hardly at any risk of being reinfected,
This is wrong, the vaccines are safe and effective - much moreso than getting reinfected with COVID-19. As a former medical professional who works with medical professionals today, you are completely misguided. Please don't repeat this stuff.
The vaccines were released to the public barely a year ago. There is no way to know exactly how safe or effective they are, supposing they are. We just don't have the data yet. What we have, however, is an aggressive censorship of any information or person critical of the vaccines.
This is wrong. We know how the ingredients of the vaccine interact inside the body and we know they leave the body pretty rapidly. We have a good idea of the side effects as over 6 billion doses have been administered worldwide.
Parent's comment will not cease to amaze me: We are going through a pandemic that has cost more lives in the US than the Spanish flu (absolute numbers) and there are still folks running around proclaiming that
> Remember - COVID is a mild disease for the vast majority.
If you had told me in 2019 that we will experience something like it in our lifetime I would not have believed you.
COVID is in fact mild for the vast majority. That is a simple fact, and not one that can be dismissed with strange non-population adjusted comparisons. Actually nobody really knows how many people died from the Spanish flu, so I really wonder where you heard that idea. Wikipedia says:
"Estimates of deaths range from 17 million to 50 million, and possibly as high as 100 million, making it one of the deadliest pandemics in human history."
NB: The high estimates come from epidemiological modelling so should probably be ignored as such modelling has no legitimacy. But even for the USA alone, there's no agreement on how many died, especially as many people (especially in the USA) seem to have been killed by aspirin overdoses rather than the flu itself. At the time aspirin was new and considered a miracle cure. Doctors panicked prescribed doses that we now know are far, far too high. From a paper published in 2009:
High aspirin dosing levels used to treat patients during the 1918-1919 pandemic are now known to cause, in some cases, toxicity and a dangerous build up of fluid in the lungs, which may have contributed to the incidence and severity of symptoms, bacterial infections, and mortality. Additionally, autopsy reports from 1918 are consistent with what we know today about the dangers of aspirin toxicity, as well as the expected viral causes of death.
The motivation behind the improper use of aspirin is a cautionary tale, said author Karen Starko, MD. In 1918, physicians did not fully understand either the dosing or pharmacology of aspirin, yet they were willing to recommend it. Its use was promoted by the drug industry, endorsed by doctors wanting to “do something,” and accepted by families and institutions desperate for hope. “Understanding these natural forces is important when considering choices in the future,” Dr. Starko said. “Interventions cut both ways. Medicines can save and improve our lives. Yet we must be ever mindful of the importance of dose, of balancing benefits and risks, and of the limitations of our studies.”
> Whether or not the vaccine or natural immunity is better protection isn't as clear as suggested either, generally the vaccines will give more reliable resistance.
Yah, perhaps it'd be best to talk about mean and variance.
For COVID-19, it looks like natural infection provides a somewhat better neutralizing titer of antibodies than vaccination on average. But there's a much larger variation in the response than vaccination provides. The people with the lowest responses are in the natural infection group, too.
> I said having the vaccine after an infection was clearly a huge benefit over having just the vaccine or just the infection - so do it.
Yes --- amazingly so. We don't have wonderful data for SARS-COV-2 yet, but some number of recipients of mRNA vaccines who are survivors of the original SARS apparently have strong antibody responses to all coronaviruses. https://www.nejm.org/doi/full/10.1056/NEJMoa2108453
Let's just say it was "on par" with a vaccine for the sake of argument, even if it is suggested it might be better/work more broadly. Is there a scientific reason, as opposed to political, why this would not exempt one from a mandated vaccine?
Most people in the US who have contracted COVID-19 don't have proof of it. Vaccinating everyone is cheaper and more consistent than trying to build out mass testing infrastructure. Plus if you can convince people to show up for a test, it's better to just vaccinate them. Tests can come back negative, or give false positives, in which case those people still won't have immunity, but the benefits of the vaccine are pretty well understood. AFAIK it's more of an issue of ensuring public safety and efficiency than whether your immune system produced good enough antibodies from an infection.
The Red Cross and the regional blood bank in my area both test for COVID19 antibodies. Seems extremely unrealistic that testing infrastructure would be too difficult considering how much we've done for the pandemic. "Just jab everyone and we're done!" sounds like a desire for a simple silver bullet solution, which is a very common Silicon Valley way of seeing the world.
Equating antibody presence to be the same as having been vaccinated would give health officials a much more accurate view of the pandemic and where resources need to be allocated instead of this odd ideologically driven need to demand conformity from everyone even if they already have immunity that appears to be an order of magnitude more durable than the jab. It makes clear that this is almost entirely about a pathological need to round off all the corners in the world and almost nothing at all about fighting the pandemic itself. But what a wonderful opportunity this pandemic has been for the authoritarian types. For them, this truly is the golden age and should be extended for as long as possible.
The Red Cross has ~7 million donors per year (~2% of the population). That's not really evidence that they could sample a large enough portion of the population as quickly as they could be vaccinated. And again, it doesn't increase herd immunity. It does at least have a side benefit of increasing our blood inventory, but also has the downside of potentially spreading infection among the unvaccinated while they donate.
> Most people in the US who have contracted COVID-19 don't have proof of it.
There have been over 45 million laboratory-confirmed COVID cases in the US. Basically all of these people can easily prove that they were infected and recovered by showing a copy of their positive result.
For those who believe they had a past infection that wasn't lab-confirmed, antibody testing costs around $50[1].
I'm sure some people will say "but lab results can easily be faked!", which is true. But the CDC cards for the vaccines aren't exactly forgery-proof either.
> AFAIK it's more of an issue of ensuring public safety...
To protect the vaccinated from the unvaccinated? And how? Vaccinated individuals can get breakthrough infections and spread the virus to others too. And you could make the argument that some vaccinated individuals, overconfident in the protection they have, will engage in riskier behavior (having close contact with others, not wearing masks, visiting poorly-ventilated indoor spaces, etc.).
Since initial infectious doses and peak viral loads seem to vary wildly in people who've been infected, I would speculate that it's much easier to quantify vaccine-induced immunity in a public health context relative to so-called "natural immunity", since those initial variables can be tightly controlled. This is a practical matter for making consistent and effective public health policy, as well as a scientific matter (viz. establishing the relative effectiveness of various forms of immunity for diverse and uncertain infection scenarios). Experts in public health and/or infectious diseases, epidemiology, etc. may feel free to correct me if I'm substantially incorrect.
However, for people who see the world through a lens that paints all public health policy with the brush of partisan politics, the distinction may be difficult to grasp.
> Since initial infectious doses and peak viral loads seem to vary wildly in people who've been infected, I would speculate that it's much easier to quantify vaccine-induced immunity in a public health context relative to so-called "natural immunity", since those initial variables can be tightly controlled.
I think you are missing the largest discriminator.
The US Vaccines[1], and the related vaccines, are highly limited resistance specific to a spike protein only, perhaps with boosters, to a number of spikes seen. Total = 1, perhaps 2 if it includes a delta variant spike booster also.
Natural immunity confers with it resistance to a number of different covid-19 viral proteins, not just the spike. We know Covid-19 has 29 proteins
Now, we know that researchers saw these antibodies, as they were the ones that said, "all these antibodies could be the target of future vaccines", and the idea is there. However, we don't know the exactly count of antibodies to all these viral proteins, we just know of their existence from research. [2]
But, to compare the strength of natural immunity to a vaccine is to fail at elementary math.
However, I am not saying that people at a high risk from age, comorbidities, or both, should not take the vaccine. That is their own decision. On the other hand, the vast majority of the research indicates that natural immunity actually provides superior immunity from a breadth perspective, since a legacy vaccine protection is comparatively challenged against a mutated spike.
[1] This is not true for all vaccines, merely "spike" vaccines. So, it wouldn't apply to an attenuated viral vaccine. However, attenuated vaccines do not prompt as strong an immune response.
> Natural immunity confers with it resistance to a number of different covid-19 viral proteins, not just the spike
I am personally closer to the antivax group than the provax group( at least in terms of mandates, because abrogation of bodily autonomy is straight up evil ), but I have to take issue with this statement.
While you are probably correct, we need to worry about biomechanics and effectiveness. If the S protein is the specific means of entry, that's definitely the one we should target. There's no reason to target proteins that don't actually bind to anything.
There are other issues regarding what are the limits to the memory of our circulating B cells. If my immune system has to "swap out" memory of, say, polio, in order to accommodate antibodies to eight different viral proteins, I'd rather it only remember one, if it's just as effective.
I'm not sure where you imagine I made any statement directly comparing the efficacy of vaccines to natural immunity. The substance of my comment is limited to the problem of quantifying the efficacy of natural immunity in the real world, from the perspective of public health policy.
These vaccines are leaky & non-sterilizing; these are not remotely comparable to the vaccines we have had throughout most of our normal lives that grant something like 99.99999% protection with minimal side effects. I'm saying that as someone as who has had a number of vaccines during my life - I am not an antivaxx.
You are, apparently, not even making a token effort to understand my comments.
If you want to talk about how much better natural immunity is than vaccines, there are plenty of subthreads in these comments where your contributions--while possibly controversial--would not be completely irrelevant. But this is not one of those subthreads. I have not expressed an opinion on that matter and I have no intention of doing so in this particular context.
>had a number of vaccines during my life - I am not an antivaxx
"Antivaxx" in today's context has nothing to do with whether you've ever accepted a vaccine in your life, and everything to do with whether you reject COVID vaccines. In fact, that's as much the meaning as anything: that people who were previously OK with vaccines (including the regimen of sometimes experimental vaccines required by the military) are somehow now vociferously opposed to COVID vaccines.
And, on that measure, even a cursory glance at your recent comment history reveals that you are unequivocally antivaxx.
You are using a pejorative directed at me, by calling me antivaxx, or, an antivaxxer.
That is actually an insult. Please refrain from insulting me.
I am not antivaxx. I am pro-vaccine, and as a veteran I am actually quite immunized. Heavily immunized in fact. Far more so than most of the civilian population.
However, this is a question of an unlike comparison.
Nope. You voluntarily made the claim that you were "not antivaxx". I merely clarified for you that your previous acceptance of other vaccines has nothing to do with the definition of "antivaxx" in today's COVID context.
You are clearly anti-COVID vaccines, as indicated by a number of your comments here. That makes your assertion that you are "not antivaxx" untrue in any contemporary discussion.
Relentlessly searching for ways to discredit COVID vaccines and spreading FUD are not mere "hesitance".
If you find the plain identification of your own behavior "insulting", then I would offer that you consider not engaging in that behavior.
> You are clearly anti-COVID vaccines, as indicated by a number of your comments here. That makes your assertion that you are "not antivaxx" untrue in any contemporary discussion.
> Relentlessly searching for ways to discredit COVID vaccines and spreading FUD are not mere "hesitance".
Critical skepticism is an important element of science.
Do No Harm is a key part of the Hippocratic Oath
Just like Informed Consent with Medical Ethics.
> Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a given procedure or intervention. The patient must be competent to make a voluntary decision about whether to undergo the procedure or intervention. Informed consent is both an ethical and legal obligation of medical practitioners in the US and originates from the patient's right to direct what happens to their body. Implicit in providing informed consent is an assessment of the patient's understanding, rendering an actual recommendation, and documentation of the process. The Joint Commission requires documentation of all the elements of informed consent "in a form, progress notes or elsewhere in the record." The following are the required elements for documentation of the informed consent discussion: (1) the nature of the procedure, (2) the risks and benefits and the procedure, (3) reasonable alternatives, (4) risks and benefits of alternatives, and (5) assessment of the patient's understanding of elements 1 through 4.
[1]
> It is the obligation of the provider to make it clear that the patient is participating in the decision-making process and avoid making the patient feel forced to agree to with the provider. The provider must make a recommendation and provide their reasoning for said recommendation
> Critical skepticism is an important element of science.
There's a continuum here. I guess we might say that at one end is blindly trusting whatever you're told, and at the other end is skepticism to the point of divergent irrationality, e.g. believing the Earth is hollow because you haven't personally been to the North Pole to check for a big hole leading to Inner Earth (where the meat goes on the outside of the sandwich). Of course, satellite imagery is all doctored to cover up the truth.
Interestingly, those extremes seem to curve back toward each other.
Skepticism is important, but it can be taken to harmful extremes, and it's important to examine "skeptical" impulses to make sure that's actually what they are. When you find yourself clinging to a "skeptical" position as evidence to the contrary continues to mount, squeezed into an ever-tinier corner of what-ifs and statistical improbabilities--or just cherry-picking data and presenting it out of context to rationalize your position--you have to know when to throw in the towel.
---
The above is presented as a reply to your comment about critical skepticism being important, because I think that's a line that's often used to defend irrational positions, often to the point of doing real harm when it's deployed in the public discourse. But I am not talking specifically about COVID or anything to do with it, so--again--please don't imagine that I've made any substantive statement wrt. the efficacy and/or risk profile of COVID vaccines, because I haven't.
You really could save a lot of time by just saying you're "anti-vaxx".
Maybe you're not familiar with the contemporary meaning of the phrase, but it perfectly encapsulates your behavior here and throughout HN.
Antivaxx is a syndrome. Some tell-tale symptoms are:
1) a scattershot litany of objections based on vague pseudo-scientific conclusions, cherry-picked de-contextualized data, and deployment of hypotheticals that, in total, amount to FUD;
2) Antivaxx denialism: that is, retreating to a position of nuanced skepticism when called on their clearly manic anti-vaccine FUD tactics, "hey, I'm just cautious/hesitant/skeptical".
3) an effort to characterize COVID vaccines as somehow nefarious or "illegitimate" versus previous vaccines because they seek primarily to prevent serious disease;
4) a relentless emphasis on natural immunity as superior to vaccines;
5) and the dispositive test that is perhaps the gold standard for an antivaxx diagnosis: deploying a range of pseudo-ethical arguments that seek to paint COVID vaccines or their advocacy as somehow immoral. This is usually deployed via vague rantings that, say, inexplicably invoke the Hippocratic Oath.
> The US Vaccines[1], and the related vaccines, are highly limited resistance specific to a spike protein only, perhaps with boosters, to a number of spikes seen. Total = 1, perhaps 2 if it includes a delta variant spike booster also.
This is bogus. A broad spectrum of immune response develops through mutation and maturation of B cells. This is why we see broad neutralizing activity-- even against Delta without a Delta-specific booster-- against all variants from vaccination.
> Is there a scientific reason, as opposed to political, why this would not exempt one from a mandated vaccine?
First of all, taking the vaccine is not political. What is political is the contrarian stance against vaccinating against COVID-19. This sad state of affairs was the direct result of an election campaign which was deeply invested in denying that COVID-19 was a public health concern, or even that it existed at all, and thus recognizing the vaccine's importance and effectiveness was deemed a sign of a political defeat and admission of responsibility for countless unnecessary deaths.
Secondly, natural immunity against COVID-19 is not a sure thing, with the risk of reinfection being as high as 17%, and subsequent infections are known to be more severe than the first[1]. In contrast, immunity through vaccination is believed to be not only more effective but also last longer[2].
Consequently, there is absolutely no reason at all, other than political beliefs, to refuse to get the vaccine.
> This sad state of affairs was the direct result of an election campaign which was deeply invested in denying that COVID-19 was a public health concern, or even that it existed at all, and thus recognizing the vaccine's importance and effectiveness was deemed a sign of a political defeat and admission of responsibility for countless unnecessary deaths.
You seem to be implying that the former president, whose administration helped fund the vaccine development, was responsible for all of the anti-vaxxer sentiment. Even as someone who is very happy Trump is gone, I must say this type of dishonesty has no place in a civil discourse about vaccination.
> ...and subsequent infections are known to be more severe than the first
You have conveniently misconstrued what your own citation says:
> Reinfections have been reported, and in a few instances, the second infection was more severe than the first, but serological responses suggest that patients never seroconverted after initial infection and ADE is a less likely cause of a more severe second infection
Some people don't seroconvert after vaccination either. Using outliers to make broad claims is not appropriate.
> ...immunity through vaccination is believed to be not only more effective but also last longer.
Linking to an infographic that doesn't provide citations for its statements isn't exactly convincing, especially when there is evidence that what is claimed might not be accurate. For example see, https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v...
Conclusion:
> This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.
> Many other countries do classify people who gained immunity from exposure the same as vaccinated.
Can you point out an example of any country that exempts those who were already infected with COVID from taking the vaccine? As far as I can tell, no European country does anything of the sort, neither does the US and definitely not Canada, and a quick Google search returns no search hit.
> As far as I can tell, no European country does anything of the sort
This data is pretty easy to find. One tip is to look at the requirements of vaccine certificates in use in Europe. Modern life is all about knowing which keywords to search for.
In the Swiss system, if you have a positive antibody test from a previous infection, you get a certificate for 180 days. Then you need another test. As long as you have antibodies detectable by the PCR test, you will have a certificate for the next 180 days. No vaccine needed. If you have covid, odds are you will have antibodies for the rest of your life[1].
The EU covid certificate is given along similar lines as the Swiss. You need either have a vaccine, have a PCR that detects antibodies (180 day validity), or received a negative test (72 hour validity). You can find details here:
> This data is pretty easy to find, so not sure what was stopping you from gathering it. One tip is to look at the requirements of vaccine certificates in use in Europe.
Actually, it isn't because your claim goes against pretty much all the information made available. Thus, the onus to substantiate your extraordinary claim is on you, specially because the odds that you've misunderstood or misrepresented your assertion are quite high.
> In the Swiss system, if you have a positive antibody test from a previous infection, you get a certificate for 180 days.
And here lies your mistake. Contrary to the original claim, Switzerland absolutely does not classify people who gained immunity from exposure the same as vaccinated. At all. If you take the time to read your own source, you'll notice that a) Switzerland supports both vaccine passports and certificate of prior infection, which are entirely different classifications, b) those who decide to only present a certificate of prior infection are forced to go through additional checks such as mandatory PCR tests prior to travel and after arriving, c) this only limited to international travel.
> The EU covid certificate is given along similar lines as the Swiss.
If you read up on the EU's COVID certificate you'll find out that the EU imposes high requirements for the certificate, such as not accepting PCR tests as proof of a prior COVID infection. Also, the same EU requires that those who were verifiably infected with COVID take at least a single vaccination dose to be deemed fully vaccinated.
Yes, like I pointed out, you need a PCR test every 180 days to get the certificate. But it's the same certificate as if you had a vaccine with the same access rights. That means that no, you don't need to get a vaccine as long as you got the disease (it's extremely unlike no antibodies will be detected if you were truly infected and recovered, but if you were diagnosed with a false positive, then no, a PCR test wont detect antibodies).
And expect to be required to get regular boosters on the vaccine side as well, so everyone will need to go through a process to keep the certificate, it does not last forever.
> Yes, you need a PCR test every 180 days to get the certificate, but it's the same certificate as if you had a vaccine.
You should read your own source. Even though the swiss COVID certificate applies to those who "have had a COVID-19 vaccination, have had and recovered from the disease or have tested negative", neither case is treated the same at all. You already admitted that by referring to the additional requirements for those who did not took the vaccine, such as a series of mandatory tests.
So now I am confused. How are they treated differently other than requiring the PCR test twice a year? You just keep saying "you should read your own source" with increasing hostility but no actual argument that says the individual without a vaccine but with the bi-annual PCR test is treated differently in any meaningful way.
Honestly there is a lot of bluster and emotion in your responses, and I'm having a hard time extracting signal from noise. Lots of people in the EU who had covid are doing just fine with getting biannual PCR tests and don't need to get a vaccine as they can get the covid certificate and have access to the same things as someone with a vaccine.
> So now I am confused. How are they treated differently other than requiring the PCR test twice a year?
Please read your own source, particularly the section on "I am not vaccinated or recently recovered from COVID-19. What should I bear in mind?". They are quite clear in stating the additional requirements for continuous testing, both before and after entering Switzerland.
Fully vaccinated travellers do not have to deal with nothing of the sort.
Don't you agree that imposing entirely different sets of requirements to those who are not vaccinated demonstrates that vaccinated and non-vaccinated but recovered from Covid is a clear indication that both cases are indeed not classified, and treated, the same?
the "recently recovered from covid" is the 180 day PCR test case, because it's defined as having a positive antibody test in the last 180 days ("recently"). So no I am not going to apply the section that is not relevant to those who have recovered with a positive antibody test in the last 6 months.
By reading the wrong section, you've come to the wrong conclusion as to how the recovered are treated.
No. The majority of Americans now have antibodies one way or another. In significant excess of the 60 to 70 percent Fauci and other public servants were rooting for this entire year. Some 80 to 85 percent of the population by now has antibodies.
"Had COVID? You’ll probably make antibodies for a lifetime"
On the exact terms given to us by Fauci and other public servants, there is no more reason for these covid mandates to exist. Not from a scientific point of view based on these links.
> The majority of Americans now have antibodies one way or another
Why are some hospital systems still overwhelmed? Where are all these very sick people coming from if almost everyone has been in contact with the virus?
Because hospitals operate with minimal spare capacity. Any epidemic wave will overwhelm the system. That being said, hospitals are not overwhelmed. There may be a handful of hot areas where that is marginally true, but generally speaking the vast majority of the country is doing just fine. I just threw a dart at Iowa: 69% beds occupancy, 10% covid. This is not what "overwhelmed" looks like.
Well some countries are saying proven infection is good for 7 months worth of vaccine coverage.
But the length and time period of the immune response is likely much more variable than those who received vaccination
P(Survive infection|Survive first infection) > P(Survive infection|Have been vaccinated),
in general the far more interesting inequality is
P(Survive first infection) * P(Survive infection|Survive first infection) << P(Survive having been vaccinated) * P(Survive infection|Have been vaccinated)
So it usually is still a better strategy to get vaccinated than to get infected.
I recommend that everyone get vaccinated if they can, especially if they haven't had a confirmed infection. For most patients natural immunity provides protection as good or better than vaccination.
There's convalescent plasma in the study we're all looking at.
Looks like a similar difference.
- People given AZ required 8.8x the concentration of their serum to neutralize A.30 vs. B.1
- For mRNA vaccines, this was 4.6x.
- Convalescent plasma-- those infected-- this was 4.4x.
- AZ dose 1, mRNA dose 2 was by far the smallest difference, 1.8x.
I'd caution in reading too much into these numbers. Comparing titers in general between the groups in this study is problematic because of vastly varying times since infection/administration. And the size of the populations is small.
They don't include the data in the paper, but they do have that data in the supplemental charts under "Convalescent". Looks like a similar dropoff as scene in people vaccinated with BNT162b2.
It should be noted that this convalescent plasma was taken from ICU patients, not people that were asymptomatic or had minor symptoms.
I have an open question that I've never been able to find the answer to:
What are the limits to the memory of our immune system? Surely there are limits, to the extent that our blood can only carry N number of Memory B cells, and those cells that still exist carry some degree of senescence, and we need M of them to mount an timely response to a recurrence of infection, how many protein antigens can our immune system actually remember and respond to over long periods of time?
Short answer: nobody knows. In any case, I don't believe an answer is realistically even possible because we can't easily isolate all the other factors involved. Also, you'll have to consider affinity maturation and the cutoff for B-cell specificity for an antigen to clearly define what you even mean by 'remembering a protein antigen'.
Except that data from the UK shows that’s precisely what’s not happening. Those who were immunologically naive when receiving the vaccine continue to not have N protein antibodies after subsequent infection. That is they did not gain new immunity that would have been gained in the reverse order of events.
It depends if the person who got vaccinated was exposed to the virus before the vaccination. If not, it is very likely that these variants will escape the vaccine induced immunity due to original antigenic sin, especially considering that mRNA vaccines only stimulate the production of spike ABs and not other ABs such as nucleocapsid ABs which target proteins that do not mutate as much as spike.
Antibodies is also just one part of the immune response, memory T cells are just as important.
We know the vaccines are not sterilizing so you can still catch and spread it. They do reduce the likelihood of hospitalization and that seems to be about that.
They do a lot more than that. A lot of the symptoms (coughing, sneezing, etc.) increase infectivity. The vaccines reduce not only the likelihood you'll get symptoms at all but if you do they reduce both the longevity and severity.
Saying "well you're just less likely to go to the hospital" underplays their importance and gives unnecessary credence to the completely false notion that if you don't get vaccinated the only person you're potentially hurting is yourself.
There is a slight chance, but it is not different than an unvaccinated person having an asymptomatic case (which is also common). That being said, the possibility of infecting others is much less when you don't have symptoms.
> The risk of spreading the Delta infection soon after vaccination with that jab was 42%, but increased to 58% with time.
42% (and even 58%) is still a huge improvement since the article says that the likelihood that an unvaccinated person will spread is around 67%.
The R0 value for Delta is between 6 and 7. So while an unvaccinated person might pass it on to ~6.7 people you will pass it on to only 4.2 people in the beginning (37% reduction), then to 5.8 people (13% reduction).
This calculation also assumes that your chance of getting Covid is the same as an unvaccinated person, which is not correct.
What interpretation are you expecting people to make? Because there's a huge impact from vaccination.
The chances of having a breakthrough infection and passing it to someone else are quite a lot smaller than the chances of getting infected while being unvaccinated and passing it to someone else, just because breakthrough infections aren't that high (Even if they are higher than we'd like).
COVID-19 vaccines aren't sterilizing to any meaningful extent. They provide only limited and temporary protection against infection. The real benefit is in protection against severe symptoms.
> We know the vaccines are not sterilizing so you can still catch and spread it
Unfortunately US media and government messaging at the beginning of this year touted the vaccines effectiveness as we historically understood vaccines to be, which was relatively sterilizing and a preventative. When Delta started infecting the fully vaccinated, it underscored the skepticism around these vaccines.
Ironically, right now, I know more people in my social circle that have had breakthrough cases then people who had Covid prior to vaccine’s release.
A.30 is basically dead, well outcompeted by Delta etc. The UK don't report on it now.
"VUI-21FEB-01 (A.23.1 with E484K), VOC-21FEB-02 (B.1.1.7 with E484K), VUI-21MAR-01, (B.1.324.1 with E484K), A.30, B.1.633, B.1.214.2 and B.1.1.7 with S494P have not been observed in the UK or within the international GISAID dataset within the last 12 weeks. These variants are no longer included in the data update."
The biggest pressure on variant mutation right now is vaccine-evasion - so the reason the Delta variant has out-competed it is likely because the Delta variant does an even better job of evading the vaccine.
In general, I'm disappointed that we are not rolling out updated boosters with variant protection. Flu vaccines are updated each year - and here we are almost two years from the initial outbreak, and we're still vaccinating people against the original form of the virus - which isn't even spreading anymore
That's not to say that it's not still lifesaving to get the current vaccine - but F - we can do better!
I've not seen much reported in the way of clinical trials / peer-reviewed publications for modified vaccines that target (the spike protein of) these variants of concern that are actively circulating.
Is there ongoing work here I'm missing? What progress has been made? I'm somewhat surprised that almost a year on from the initial vaccination roll-out in the UK we're now dishing out boosters which are .. identical to the vaccinations given out initially.
That is a fantastic question. We are still vaccinating & boosting against the original variant. Would "the experts" please demonstrate that vaccines against variants are effective, given that original antigenic sin is a long known and well documented phenomenon?
> Is there any reason to be afraid of getting vaccinated?
There's plenty of reasons, do you mean to also ask how likely other people on the internet believe each one to be?
For example, if you ask me, this is my personal assessment:
Reason 1 - Vaccines could also contain microchips or other device for tracking, brainwashing and remote manipulating my body and mind by whoever mastermind is in charge of what goes in them.
I think that's very unlikely, I'd give it a 0.00000001% probability. I just dont know of any possibility for such advanced technology. And I can think of many different means that you can be more cost effectively tracked, manipulated or brain washed. I can also think of other ways they could have injected you with such things.
Reason 2 - The vaccines will result in worst long terms negative effects on your health than getting Covid.
I think this is a little more likely, but given all prior vaccines have shown to be quite safe, and even if they could be responsible for some long term effects, even some we haven't linked back to them yet, seeing as life expectancy and quality of life has grown year over year since the introduction of vaccines, it seems the equation would still play in their favor.
There are also more and more literature linking prior viruses as a possible cause of long term negative effects like dimentia, various auto-immune diseases, etc. So it would seem Covid is more likely to introduce long term negative effects.
So I'd give it a 1% chance.
Reason 3 - The vaccines will result in worst short term effects on your health then getting Covid.
I think this one has been shown that most of the time, Covid is more likely to kill you or make you really sick as compared to vaccines.
I'd give this one a 0.0001% chance.
Reason 4 - Vaccines can stop your pregnancy or your period and make you stink
I have seen zero cases of this, and everyone who's had a vaccine to my nose do not smell, and still have period and can get pregnant.
I'd give this one a 0.000000000000000001% chance.
There might be more reasons, but those are the ones I've heard most often, and this is only my personal risk assessment.
Well said, and pretty reasonable numbers over all.
The one point I'd add some clarification to is your .0001% chance of the vaccine having worse short term health effects. It's not that the number is wrong, exactly, it's that it's an average. It's contingent on a host of factors, but once you learn how rare side effects are, it's tempting to rhetorically bludgeon people with concerns over the head with this, even though in some cases they don't deserve it.
To give the most obvious example [1]:
> Some advisers were concerned that young and healthy Americans who don’t need a booster might choose to get one anyway. Side effects are uncommon, but in younger Americans they may outweigh the potential benefits of booster doses, the scientists said.
> “Those that are not at high risk should really be thoughtful about getting that dose,” said Dr. Helen Talbot, an infectious disease expert at Vanderbilt University.
That's pretty strong language suggesting that if you are (1) young, (2) healthy, (3) already vaccinated, the risks might outweigh the benefits of getting vaccinated again (getting a third shot). That's extremely limited, of course, but it's important not to neglect the striking degree to which contingent facts can modulate the cost / benefit analysis.
> Reason 4 - Vaccines can stop your pregnancy or your period and make you stink
> I have seen zero cases of this, and everyone who's had a vaccine to my nose do not smell, and still have period and can get pregnant.
> I'd give this one a 0.000000000000000001% chance.
VAERS is tracking the following:
17,128 DEATHS
83,412 HOSPITALIZATIONS
92,017 URGENT CARE
127,641 DOCTOR OFFICE VISITS
7,532 ANAPHYLAXIS
10,179 BELL'S PALSY
2,631 Miscarriages
8,408 Heart Attacks
10,304 Myocarditis/Pericarditis
26,199 Permanently Disabled
3,875 Thrombocytopenia/Low Platelet
18,925 Life Threatening
31,753 Severe Allergic Reaction
9,734 Shingles
2,631 Miscarriage
15,158 Menstrual Disorders
5,401 Vaginal/Uterine Haemorrhage (All Ages)
The key question about VAERS data is, how bad is the under-reporting of side effects? The allegations of under-reporting ratios are all over the place, from as low as 1 to 3 undercount, to as bad as 1 to 100 undercount.
We really don't know how bad the situation is, or isn't. We just know there are side effects and some of them are non-trivial.
> A report to VAERS generally does not prove that the identified vaccine(s) caused the adverse event described. It only confirms that the reported event occurred sometime after vaccine was given. No proof that the event was caused by the vaccine is required in order for VAERS to accept the report. VAERS accepts all reports without judging whether the event was caused by the vaccine.
Also, where are you getting your numbers. When I search the database (after agreeing several times that I read and understood a disclaimer similar to the above), I found 8,225 reports of death
That's interesting data. How easy would it be for you to compare it against the same for say other vaccines? I still think the Covid vaccines probably over-report compared to others, since its the only vaccine I ever got where I got notified about Vaers and told to report, but it be an interesting comparison and would give us a head start. We'd probably also need the count of people who received each vaccine to normalize the comparison.
Though to be fair, and again, I'm a random person online explaining my personal assessment, but in my assessment I also take into account that I assume that smarter people then me have already ran all these numbers, and maybe I'm naive to assume that, but I also don't have the time, know how and the access to all the data I'd need to do so myself.
In that case, I have to either trust institutions and academics of multiple countries who seem to mostly agree +/- a few difference, or I have to trust volunteer effort from generally amateurs on the internet mixed in with some legitimate trolls. And since in my field of expertise, I see often that the internet is filled with more crap than accurate information, I don't really trust the internet as much, especially the information that's easy to find.
Do keep in mind that these raw counts are meaningless, and arguably scare-mongering. Some number of people will have a heart attack regardless of whether they had the vaccine... If all these numbers were zero, we should all get the vaccine simply to live in perfect health forever!
We also know that the usual mechanism for bad reactions to vaccines is allergic reaction, which is easily observed on a short timescale, and basically doesn't happen with the covid vaccines.
> Do keep in mind that these raw counts are meaningless, and arguably scare-mongering. Some number of people will have a heart attack regardless of whether they had the vaccine... If all these numbers were zero, we should all get the vaccine simply to live in perfect health forever!
The question is really fundamentally simple for a massive vaccination campaign
Expected injury rates as a % of the population
Actual / Reported injury rates as a % of the population
Even while accounting for the low likelihood of even receiving reports of things.
We already know that some of the injury reports coming in have been independently verified by other nation's health departments. After all, there is a reason for some of the vaccine pauses among the young and healthy in the nordic countries.
>We already know that some of the injury reports coming in have been independently verified by other nation's health departments. After all, there is a reason for some of the vaccine pauses among the young and healthy in the nordic countries.
Other countries with their own health systems have independently confirmed these issues.
A friend of mine that happens to be a medical professional in a European country told me of the clotting related issues starting to show up in their own numbers far in advance of it being likewise confirmed in VAERS too.
That is why we know about these issues.
Country A and Country B have problems that show up, they ask which vaccine, which vector, etc, and they draw conclusions.
I think this is a likely concern in some countries. The vaccines are challenging to transport and properly keep stable and manufacturing of them happens in many places and was put in place and scaled up very quickly, quality control could be an issue, same as proper transportation and storage.
The non-crazy, non-simple faction of vaccine resistance argues about the likelihood of ADE, which is where the vaccine primes the immune system to have a larger reaction against some types of future infection. The typical dwell time before effect is something like 12-18 months.
Argument goes along the lines that "all" previous coronovirus vaccines were found to have ADE effects. It took a long time for them to show up, but the effect was large and the trials were abandoned.
So apparently we're still all going to die. Spring/Summer 2022 (northern hemisphere time) will be the cataclysm.
I'm inadequately gnorant to evaluate the argument on merits, but I find it interesting because it fits the classic definition of "bullshit".
>The non-crazy, non-simple faction of vaccine resistance argues about the likelihood of ADE, which is where the vaccine primes the immune system to have a larger reaction against some types of future infection. The typical dwell time before effect is something like 12-18 months.
Didn't tens of thousands of trial participants get covid vaccines back during July to September last year? They're still monitored I think. If what you said is true then they should be dropping like flies which they are not.
You may find interesting that Pfizer erased the control group for the 5-11 EUA study. Probably for your study too. There is no longterm data & analysis by design. The practices of BigPharma are questionable at best.
> Pfizer intentionally wipes out the control group as soon as they can by vaccinating all of the kids who initially got the placebo. They claim that they are doing this for “ethical reasons”. But everyone knows that Pfizer’s true aim is to wipe out any comparison group so that there can be no long term safety studies. Wiping out the control group is a criminal act and yet Pfizer, Moderna, J&J, and AZ do this as standard practice with the blessing of the FDA/CDC.
What? It's an adaptive trial design, not a criminal act.
The vaccine was effective/safe enough that it would cause more harm to leave them unvaccinated. If anything it means that there's more points of safety data by doing it this way.
Not very happy about the use of 'criminal' by the original source, but you are sadly missing the point. NONE of the kids in the Pfizer FDA clinical test developed severe covid. Not the vaccinated kids, not the unvaccinated kids. There was ZERO medical reason to vaccinate the control arm of the trial. Given that the two major concerns around covid vaccine are a. effectiveness fading over time and b. lifetime OAS, makes you wonder.
> COVID-19 rates in children ages 5 to 11 are so low that there were ZERO cases of severe COVID-19 and ZERO cases of death from COVID in either the treatment (n= 1,518) or control group (n= 750).
I tried to be clear with my language -- apologies if I did not succeed.
My intention is not to spread it, but to describe it because I think it's useful to understand the narrative. You cannot disagree with something you do not understand.
There's a faction of resistance which is neither shrill, nor obviously stupid, and they have coalesced around a narrative that is constructed in a way to be very compelling and frightening.
It's either an elaborate effort, or it's the natural result of smart people not trusting evidence, and extrapolating into authoritative-sounding "maybe"s.
In short, classic "bullshit".
But it would take someone more learned than I, to argue on merits. The promulgators of this narrative have read the Wikipedia article on ADE, and insist that that narrative is flawed, for reasons I cannot contradict.
Personally, I don't believe it for a second, but my reasons are rather prosaic: IME the more elaborately-cooked the future scenario is, the less likely it is to happen, outside of fiction. Nature tends toward the non-dramatic. I expect to be proven correct over the next ~year.
That is not the question I asked. Furthermore the degree of which the current vaccines work against variants is dependent of the variant itself, please consult the OA. (Also dependent on time, but that's a separate conversation .)
I am asking specifically if there is any hard evidence of vaccine effectiveness to back statements made by biopharma corporations about variant-specific vaccines, for example:
"We have built a process that within 95 days from the day that we identify a variant as a variant of concern, we will be able to have a vaccine tailor-made against this variant," [Pfizer CEO] Bourla said.
> the degree of which the current vaccines work against variants is dependent of the variant itself
Yes, we all know that. Follow the scientific literature and you will find updated vaccine assessments soon after a concerning variant is noticed.
> "We have built a process that within 95 days from the day that we identify a variant as a variant of concern, we will be able to have a vaccine tailor-made against this variant," [Pfizer CEO] Bourla said.
That's likely closely guarded IP, so I don't think there is hard evidence for that statement. But the phase I clinical trials for Moderna's [1] and Pfizer's [2] started respectively in February and April 2020, just a few months after covid became a problem. This is IMHO reasonable evidence that 95 days is a plausible lead time.
You are misunderstanding the CEO's statement. It says that 95 days are sufficient to make the vaccine, it does not mention testing. You cannot assess the lifelong effects of almost anything in just three months.
Thanks for the correction. I find it strange to believe that 12 months are sufficient to assess the lifelong effects of an immunity system intervention.
Uncertainty is a fact of life and decision making under uncertainty an important skill to be successful.
And in case it is not clear, in this thread I am not advocating neither for or against vaccines, so we can end it here unless you have something of substance to add.
Do you mean in terms of protection, or side effects?
In terms of long term protection, I don't think we really know yet.
In terms of long term side effects - do we know of any past vaccines with notable side effects that only became known after 12+ months? Genuine question.
In term of protection. For starters, if vaccine effectiveness were holding, there would be no need for boosters.
A picture from a recent preprint of 600k veterans over 6 months shows troubling VE against infection curves. J&J VE against infection is gone. Pfizer curve is just 2 months behind, at 53% and dropping.
Fortunately VE against severe infection holds much better at 77% Pfizer for June-Sept 2021 time period. The clinical trials claimed 94%, so there is a drop there. Nobody knows what will be the VE against sever infection a year from now, and we appear to have decided to preemptively boost so we might never know.
Alas, none of this takes in account future virus variants and their interaction with OAS. OAS means that building an immune response against the virus today will prove ineffective for a virus variant 10 years down the line. The worst known scenario was encountered with dengue fever. An excerpt from a 2011 paper summarizing the dengue situation:
"Original antigenic sin has the advantage that a response can be rapidly mobilized from memory. However, the downside is that in some cases, such as dengue, the response is dominated by inferior-quality antibody. In influenza, original antigenic sin has been shown to reduce the effectiveness of vaccination (13, 34, 51). In dengue, the effect of original antigenic sin has considerable bearing on vaccine strategies. Once a response has been established, it is unlikely that repeat boosting will be able to change its scope, meaning that balanced responses against the four virus serotypes will need to be established with the first vaccine dose."
>Fortunately VE against severe infection holds much better at 77% Pfizer for June-Sept 2021 time period. The clinical trials claimed 94%, so there is a drop there.
The clinical trials were run against the original version, while the data you presented seems to be overlapping with the spread of Delta, yet you never mention Delta in your comment.
I am a concerned citizen and parent. I only have so much time to write a well source comments. I wish people were applying just as much critical carefulness with regard to CDC publications. Where is the CDC longitudinal VE study? Do they even track VE data over time? Why do I have to sift through data instead of "the experts"?
Let's look at the weekly UK vaccine surveillance report, week 36 vs. week 42, afaik both within the UK Delta wave. For VE against severe disease, let's look at 'Deaths within 28 days of first positive COVID-19 test by date of death' tables. Let's pick age group 40-49 (older parents) and compute VE = 1 - vax_ratio / unvax_ratio.
Notice something? Same for all other age groups. Same for all the intermediate VE reports. A small but constant gradual VE decline.
FWIW, none of this makes me any happy. I wish the vaccines were holding effectiveness, that we didn't need a booster within 1 year of the initial shots and that the pandemic was over. Alas, reality does not cooperate.
It's not so simple, you need to look at the total number of people in each age group or you may fall victim of Simpson's paradox [1] (as both of those reports say):
> These data should be considered in the context of vaccination status of the population groups shown in the rest of this report. The vaccination status of cases, inpatients and deaths is not the most appropriate method to assess vaccine effectiveness and there is a high risk of misinterpretation. Vaccine effectiveness has been formally estimated from a number of different sources and is described earlier in this report.
In particular, the reduction of death rates among non vaccinated over time may be caused by natural selection, i.e. the weak died already while the remaining ones have unusually strong immune system (aka survivorship bias [2]).
There may be other unaccounted confounders, too, such as a change of behaviour over time where the degree of change is dependent on the age group and/or vaccination status. For example, an apparent reduction of effectiveness for younger people may be caused by them going back to work/study, thus increasing their probability of getting infected, while older folks staying in care homes as before.
Funnily enough, both Simpson's paradox and uncorrected confounders can result in observed correlations that are opposite to the real causality effect.
And to clarify, I'm not saying your VE numbers there are wrong, just warning readers about the dangers of statistics.
I agree! Another reason why VE appears to decrease might be that the ratio of unvax population with prior infection might be growing, and it's a wash between vax and post infection natural immunity.
OTOH this is not an isolated data point. We have: the booster push (why?), the veteran study, the PHE data. Something doesn't add up. For whatever reasons, the observed epi VE, after all the confouding factors are accounted by reality, is fading for both infection and severe infection, though VE agains severe infection is fading at a slower rate. To the point of J&J VE against infection (the weakest of the bunch) being almost gone in 6 months. I don't have a time machine, but I'm really interested to see how the Jan 2022 VE numbers hold up across the board.
Given OAS concerns (please re-read the dengue study excerpt I already quoted), near zero covid risk for kids, rapidly fading VE against infection and the general lack of long term data about covid & immune system (no time machines), what exactly is the rush to vaccinate kids against the original variant?! And why do we pretend we can just tweak vaccines to any new variant, when, while technologically we can concoct any protein we like, the immune system doesn't turn on a dime?
That's interesting, though the article concludes with:
> Despite the persistent connotation of “sin” as a negative attribute, it is clear that OAS-like responses are neither inherently “good” nor “bad.” The desirability of OAS responses is instead context dependent
It doesn't really seem from that article like we have the means to predict what OAS will be most beneficial in the future, so I think everyone are just flipping a coin here. Either you get OAS from some random vaccine available at some point in time, or you get it from randomly catching some random virus at some point in time.
They said they built a process. That's a different assertion than that any such vaccine will be effective. To know that would require a time machine. That said these people made a lifetimes work of being as sure as they can that such a thing will be effective. I don't think we have better information or hard evidence from other sources.
I fully agree. To prove long term vaccine effectiveness (original, boosters, variants, sequence thereof) we indeed need a time machine. In other words, we are running a species level grand experiment with unknown outcomes. That biopharma corps are planning to routinely launch new immune stimulants without any long term effectiveness data gives me pause.
We are all taking part in a grand experiment whether we like it or not, because the SARS-CoV-2 virus definitely has a broad range of known short-term outcomes, many bad, and unknown long-term outcomes, likely also bad. All choices are a bet on the future. 77% is betting with loaded dice.
Seems to me that one doesn’t pause when being attacked by a bear, a big cat, or even a wasp. And unless you’re anaphylactic, the latter can’t fudge you up as bad as a virus. Don’t pause too long, leopards are on the prowl.
We are always running grand experiments in virology, evolution never stops. We know the outcome of evolution, that is novel viruses pop up and kill massive numbers of people.
My take of your entire thread is we let these natural processes kill millions because we fear a significantly smaller long term risk.
They ran studeies/trials on variant vaccines they deveolped and found that it wasn't better enough than the original vaccine/booster to go to the large effort of rolling out a different vaccine all over again. Atleast for Delta and the UK variant.
They haven't found original antigenic sin so far. There's a couple links with some data (although I couldn't find a pre-print or published article right now) in this comment: https://news.ycombinator.com/item?id=29005187
Thanks for the links! Note that they are making variant-specific vaccines, not proving that variant-specific vaccines are effective against the target variant, if delivered after the original vaccine.
Side note: I hope we can do better than taking at face value investor press releases by the biopharma corps producing the vaccines.
>Note that they are making variant-specific vaccines, not proving that variant-specific vaccines are effective against the target variant, if delivered after the original vaccine.
You are correct that it isn't proving vaccine efficacy, but it is showing a different set of antibodies created by the variant vaccines that are more effective at neutralizing the targeted variant than the antibody collection created by the original, WT-targeted vaccine.
>Side note: I hope we can do better than taking at face value investor press releases by the biopharma corps producing the vaccines.
I hate science by press release too. I wish I was better at bookmarking the pre-prints and journal articles I find/read, but they'd just be a mess I couldn't find anything in either :|
A South Korea paper from 2016 argues they are related "sometimes". Note that coronaviruses are RNA viruses.
Now, all the epi data we have indicates that the covid mRNA vaccines are effective against covid variants of concern. No need to panic.
"Original Antigenic Sin Response to RNA Viruses and Antiviral Immunity"
"Abstract: The human immune system has evolved to fight against foreign pathogens. It plays a central role in the body's defense mechanism. However, the immune memory geared to fight off a previously recognized pathogen, tends to remember an original form of the pathogen when a variant form subsequently invades. This has been termed 'original antigenic sin'. This adverse immunological effect can alter vaccine effectiveness and sometimes cause enhanced pathogenicity or additional inflammatory responses, according to the type of pathogen and the circumstances of infection. Here we aim to give a simplified conceptual understanding of virus infection and original antigenic sin by comparing and contrasting the two examples of recurring infections such as influenza and dengue viruses in humans."
I work at an immunology lab which is next door to most of the Oxford vaccine group.
I think the quick (and overly simplistic) answer to this question is that models (e.g. convolutional networks) that predict which chunks of viral (or human) proteins are displayed to immune cells (HLA presentation), along with other kinds of models (like those predicting crossreactivity of T cell receptors against mutated epitopes) are really primitive (mostly because of low quality training datasets, it's not really a hard problem like e.g. protein folding).
Hence, rushing a new vaccine is not easy as there is a lot of labwork to do. As a matter of fact, all COVID vaccine designs had essentially the same payload (the whole spike protein). Modern subunit vaccines would typically include only little chunks of the spike (to increase efficiency and avoid side effects). But this was not trivial to do quickly without good in silico models.
Why not just update the vaccine with the corresponding sequence from the Delta variant? Isn't the Delta variant today a better baseline than the ancestral virus?
Or do a mix - first shot ancestral, second shot Delta.
Moderna and Pfizer tested variant-specific (B1.351) boosters and found they weren't significantly more-effective than a third dose of the original vaccine.
https://www.nature.com/articles/s41591-021-01527-y
>found they weren't more-effective than a third dose of the original vaccine
This goes against the paper:
>A boost with mRNA-1273.351 appeared to be more
effective at neutralization of the B.1.351 virus than a boost with mRNA-1273, evidenced by the
higher mean GMT levels in the Part C cohort 1 participants (1400) than the GMT Part B
participants (864) against the B.1.351 virus. Additionally, the difference between the wild-type
and B.1.351 assays at day 1 dropped from 7.7-fold prior to the boost with mRNA-1273.351 to
2.6-fold at 15 days after the boost.
Thank you for posting this though -- I was looking for it earlier for my own comment and couldn't find it! Bookmarking now.
Novavax has also been working on a Beta variant booster (and I believe has moved on to a Delta booster that hasn't started NHP trials yet) -- here's some info from a presentation: https://www.novavax.com/sites/default/files/2021-05/NVAX-WVC... (It's slides 17 and 18)
Pfizer/BioNTech definitely has a Delta booster getting ready for NHP trials, but my Google Fu is lacking today, apparently.
Even if A.30 was "more contagious", like Alpha, it isn't as contagious as Delta and thus would get outcompeted.
There's a lot of variants of concern. Its important to keep an eye on new variants, but don't worry about them until they cross the 1% or 5% mark. At that point, you can better theorize that they might be outcompeting the dominant strain.
You _really_ don't know that something is outcompeting until it reaches 50%. But by then its too late. The 1% or 5% points are still a month or two in advance of the 50% crossing, in both Alpha and Delta.
So that's where I keep my attention: at the 1% and 5% points. A variant gotta get to 1% before it can reach 50% of the world ya know?
Basically one spreads faster than the other so after a few iterations almost all of new cases are the new variant.
> How would Delta prevent A.30 from thriving?
Directly by driving up immunity, indirectly by coercing people to take steps to slow the spread of delta, which also slows the spread of a.30. Things like vaccination, social distancing, mask wearing etc...
> Why won't we become infected by Delta and A.30?
Because Delta probably give you significantly more immunity than a vaccine. Specifically infection gives both more robust and stronger immunity than the vaccines.
> Specifically infection gives both more robust and stronger immunity than the vaccines.
Isn't there evidence that says the opposite? And that immunity due to infection is much more variable between individuals and infections, due to how the immune system responds to the virus.
> SARS-CoV-2 naïve vaccinees had a 5.96-fold (95% CI, 4.85 to 7.33) increased risk for breakthrough infection and a 7.13-fold (95% CI, 5.51 to 9.21) increased risk for symptomatic disease. SARS-CoV-2-naïve vaccinees were also at a greater risk for COVID-19-related-hospitalizations compared to those that were previously infected.
> Conclusions This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.
Also just in terms of baseline beliefs based on the physical world, I would assume that the vast majority of the time an infection would be more protective than a vaccine.
>Also just in terms of baseline beliefs based on the physical world, I would assume that the vast majority of the time an infection would be more protective than a vaccine.
It is also orders of magnitude more deadly. Vaccines are proven to be much safer than getting Covid.
This is one preprint study comparing natural immunity to the Pfizer vaccine. It is interesting and may hold up after peer review. However, we have to be careful drawing broad conclusions and over interpreting these results.
The danger is that we are already seeing many groups pointing to this study and trying to read this as meaning we should not be getting vaccinated, because obviously getting covid is better. We should not forget that in 2020 and into 2021, despite significant lock downs and enforced/encouraged masking, and without widely and globally available vaccinations we lost about 5 million people to Covid. Skipping vaccines in favor of "natural" immunity is a path to continued carnage.
People are not usually saying getting covid is better (not without many qualifiers anyway), they are saying that if you already had covid, getting shots might have bad risk/benefit ratio. (you get all the risk for small additional protection).
>Those who had recovered from COVID-19 months before receiving their jabs harboured antibodies capable of defanging the mutant spike, which displays much more resistance to immune attack than any known naturally occurring variant. These peoples’ antibodies even blocked other types of coronaviruses. “It’s very likely they will be effective against any future variant that SARS-CoV-2 throws against them,” says Hatziioannou.
>People are not usually saying getting covid is better (not without many qualifiers anyway), they are saying that if you already had covid, getting shots might have bad risk/benefit ratio. (you get all the risk for small additional protection).
You should really check what people are saying on random posts on Facebook.
I've seen it repeated pretty extensively on r/covid19, which I have to say comes across as a much more scientifically robust site for covid information than Hacker News. The quality of information here isn't much above Facebook.
>I've seen it repeated pretty extensively on r/covid19, which I have to say comes across as a much more scientifically robust site for covid information than Hacker News. The quality of information here isn't much above Facebook.
I 100% agree with you on the quality of information here vs. there. It is much, much more strictly moderated. But with that moderation, that subreddit does not recommend going out and getting COVID in lieu of a vaccine. Even if initial response is better for COVID.
COVID + Vaccine is by far the best, but that doesn't mean you should skip the vaccine to make sure you go the 'rona frst.
Vaccine + Vaccine (and maybe + vaccine) is, by far, the safest combination for pretty much everyone people.
The same way that Delta has decimated Flu Type B/Yamagata to the point that some are whispering that Flu Type B/Yamagata has gone extinct. (The Flu is still around, but Type B/Yamagata was very, very common before COVID19 hit. It hasn't been seen for almost 1.5 years now)
Its not like "Delta-variant" gives you immunity to Flu Type B/Yamagata. But people around the world are masking up and locking down (well, in 2020 anyway). People's behaviors change when a large-scale pandemic like this occurs, and the weaker viruses die out.
Even ignoring that, COVID19 forces an immune response. Yes, this immune response includes memory-cells (which remember COVID19's signature), but it _ALSO_ increases other immune cells (Neutrophil, killer-T cells, among others) which will hunt down any virus more effectively. This effect is temporary, but still a big enough effect to see the body fight off other diseases a bit better after getting sick from anything.
So even though COVID19 / Delta doesn't give you any immunity (ie: memory cells / antibodies) to Flu B/Yamagata, you see Delta outcompeting it and driving Flu B/Yamagata to extinction.
--------
Delta transfers memory-cell responses + antibody responses (two attributes of "memory immunity") against COVID19, and Alpha, and other variants. Sure the disease is evolving, but its not like these antibodies are totally useless against the virus within the same line.
COVID19 simply doesn't evolve as quickly as the flu does.
--------
This effect, in reverse, was seen in 2020 where recipients of the standard Flu shot had something like a 5% lower chance of getting COVID19. The temporary "immune response" that your body built up for the Flu vaccine had a minor (but measurable) effect on COVID19.
Getting sick with _ANYTHING_ makes it harder for other viruses to attack you. Your body just goes into overdrive making various white blood cells.
You asked a good question that I’ve wondered as well. Basically someone has to show that immunity to one variant confers immunity to another, which is not at all obvious since presumably they have different epitopes. I guess what people are suggesting is that the epitopes are distinct enough that a targeted vaccine might not cover both, but not so distinct that they behave like separate infections in vivo. But I would hope that an expert can chime in and shed some light here.
>I guess what people are suggesting is that the epitopes are distinct enough that a targeted vaccine might not cover both, but not so distinct that they behave like separate infections in vivo. But I would hope that an expert can chime in and shed some light here.
There are sooooo many papers that prove this -- stop pretending you are too important/lazy/etc to search for them yourself because you want to write some anti-vax BS.
Same question, especially that if someone is infected with delta he can only infect someone with delta. So delta can be outperformed at the person level only if the person is infected by both variant at the same time.
For me the only way a variant can be outperformed is that all people who get infected get also infected with the other variant OR the first variant for whatever reason stop being transmissible
>For me the only way a variant can be outperformed is that all people who get infected get also infected with the other variant OR the first variant for whatever reason stop being transmissible
Because being infected by the successful, fast-spreading one confers you a measure of immunity against the less successful variant, thereby directly suppressing it.
> Is it possible that the heavy mutations detected on the A.30 variant also make it less contagious?
That wouldn't surprise me. The spike is central to how SARS-CoV-2 is so infectious. If the virus mutates the spike too much, it might evade the vaccines, but at the cost of being less infectious.
What's surprising is this research says, in vitro, A.30 is more infectious.
Regardless, as you and others say, in real world conditions A.30 doesn't appear to out compete Delta.
>Is it possible that the heavy mutations detected on the A.30 variant also make it less contagious?
100%. This strain hasn't been seen since May. It has already died out because of Delta.
All of these discussions are academic -- we really are only talking about if a Delta variant can gain these mutations and really wreck havoc. And the answer is "probably not" (for a while, anyways)
the results in the paper suggest, the mutations facilitate viral mechanisms of entry and antibody evasion.
efficacy of Oxford, Pfizer, and hetero-innoculation with both were examined, indications were given of reduced efficacy of either vaccine alone vs CoV A.30. The combination of both vaccines[hetero-inocculation] was associated with higher efficacy vs A.30
the mutations appear in vitro; to confer inhibition of vaccine induced antibody binding; enhanced cellular entry; enhanced pulmonary[lung] trophicity[targeting]
relative efficacies of moderna; Johnson&johnson; vs Oxford; Pfizer were not examined.
genuinely asking, how do we actually know the delta variant is real, and is the dominant variant causing the current cases?
do people actually get tested for specific variants, or is it just a generic covid test?
It depends where you live. The UK was an early[0] leader in sequencing a lot of their cases. They hit 600,000 sequenced cases in July[1].
That said, if you just want to know what proportion of the population has delta, you don't need to sequence that many cases. The point of sequencing a large fraction of cases is to catch emerging variants, that wouldn't be likely to be caught otherwise. But to know whether Delta is 30%, 50%, or 70% of cases, you just need a good random sample, not a particularly large one, and I imagine you can do that at the labs where the PCR tests are being run.
(at one point, I recall that the UK had a test that matched on three distinct sites on the virus, and they found that one of those sites would turn up negative for a particular variant, so they were able to use that as a proxy for the spread of the variant. I don't remember if that was Alpha or Delta though, and obviously it's no replacement for sequencing)
NZ had until recently sequenced 100% of its cases, and used that sequencing information to map person to person infection linkages. This included all of the people in the mandatory 2-week quarantine at the border. So in NZ, yes, every case was tested for specific variants. Delta does seem to be real.
Some small subset of COVID tests are sent to larger labs to perform a more detailed genetic test to determine specific variants. The prevalence of different variants within that set is extrapolated to the population of the region from which it originated.
If the lab finds that 87% of the samples from Adam's College are of the Omega Mu strain, then it's assumed 87% of total cases at Adam's College to be Omega Mu variant.
In Washington state, a percent of positive tests are sent to the dept of health for variant sequencing. You can see the published results by week. Delta has outcompeted every other variant for several months. All covid is essentially delta.
This is a speed-up that pre-dates the mRNA trick Moderna had been working on, a virus from chimps (so humans aren't immune to it because it wouldn't infect humans normally, yet chimps are similar enough that the virus can get into a human cell) but hollowed out to make whatever you want instead of more copies of itself. You put any payload inside it and it'll re-program the patient's cells to make that for a brief period until the immune system cleans up the mess. This vaccine uses the spike protein as payload to train your immune system.
Is it also the case that the human getting vaccinated build up immunity to the carrier virus and thus booster shots might become less effective? Would that be a reason to get a booster shot from something other than AstraZeneca?
Exciting that they're using it as a platform to develop other vaccines.
But I still maintain the official names are ridiculous. “Vaxzevria” is the trademark used by AstraZeneca in the EU. (As you say, not ChAdOx1.) And yes, the general population end up seeing Vaxzevria, on their vaccine information forms, and online at https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria-...
Someone on Twitter says: "Galaxy brain take: Pfizer intentionally picked a terrible & unpronounceable brand name because it wants people to keep calling it "the Pfizer vaccine"". (I personally will just pronounce it as "Moriarty", that being the closest recognizable name.)
For other drugs, an amazing amount of effort is devoted to finding something that a) sounds "promising" but b) without making legally-untenable promises.
The name `Viagra`, famously, is supposed to evoke ideas of vigor and Niagra (Falls). Pfizer had some trouble with Champix (varenicline), which some regulators thought was too close to "champion", and so was called Chantix in some markets instead.
No, I don't think Comirnaty is any better! I am however relatively partial to Spikevax, aka Moderna: at least Spikevax is easily pronounceable.
I suppose you mean the vaccine names are mainly useful for regulatory purposes, because the general population will continue to name the vaccines after the manufacturer or researchers?
As a native French speaker, I would say Comirnaty is actually easier to pronounce than Spikevax, and I suspect it might be similar in other Romance languages.
Yes, and it was only when the AZ vaccine (Jansen?) showed a trombosis risk that all manufacturers started to fokus on branding their vaccines to potentially distance themselves, or was this a timely coincidence?
Why couldn't they just be called Moderna/Pfizer/... Covid Vaccine?
IIUC, when COVID first gained notoriety, there was a large public effort to solve its molecular structure [0].
Articles like this seem to imply that they've solved the structure of numerous variants, making me think we (collectively) can do it much more quickly now.
If that's really true, what's changed? Does knowing the structure of other COVID variants give us a massive head start? Or has there been a massive investment in computing power for solving COVID-variant stuctures?
Famously, once the novel coronavirus was sequenced, Moderna had their mRNA sequence ready just a few days later. This was well-covered in the press.
All the time from then to general availability of their vaccine was spent on testing and scaling.
This is not exactly what you asked. But if the question is whether we have a speed advantage on vaccines because of greater understanding of viruses now, the answer is yes. It’s one reason the COVID-19 vaccine was the fastest in history.
Should it become necessary to separately vaccinate against coronavirus variants, the same advantage would confer. And vaccine makers have said they are monitoring variants and ready to go, if necessary.
The question is, will it be necessary? And how much testing will variant vaccines need to undergo?
No, there are not solved structures for these variants (in general). They're using computer modeling.
Even if there were, changes of a single amino acid that don't induce significant conformational (shape) change are the sort of thing that you'd need a very good structure to discern, since they're mostly on the surface of the spike, and probably spin around a lot.
The most relevant thing to know is what a mutation / mutations looks like in the context of antibody binding, but that's even harder to get a good structure. It's not something that can be done quickly.
when the focus is on individual molecules it is about a statistical measure of bond angle, distance, resonanceforms, charge distribution, and rotational freedom.
this ends up looking like the quantum physics conundrum where there is a central tendency rather than certainty, until you pin it down in some way.
this is why we have a vaccine to begin with, the realization that there are conformational frequencies to the S protien, and a particular locus in the sequence is associated with the conformational change that sequesters the binding domain of S protien. thus the 2proline version of S was used in subsequent vaccines, allowing the ACE2 binding domain to remain exposed to the PAMP recognition machinery.
it takes months or weeks depending on how well the supervising scientist receives a request, it used to take years and decades in many cases.
> this ends up looking like the quantum physics conundrum where there is a central tendency rather than certainty, until you pin it down in some way.
Yes, this is always true. Entropy is real, and loss of entropy affects free energy of binding. Even "structures" aren't really structures, but instantaneous pictures of a system in constant motion.
Computational docking (figuring out what drug molecules bind strongly to) is still not solved. In order to find drugs that 1. work well and 2. aren't toxic we need robust docking estimators that work well over a wide variety of proteins. My understanding of the space (which comes from undergrad comp bio, so please someone feel free to correct me) is that just having a molecule that binds well to your target doesn't mean it's going to work well as a drug, because there are delivery and toxicity concerns.
at least for identifying variants, you don’t necessarily need to know the full (highly complex) structure of each variant, just the relevant diffs from the original variant, and computer modeling to tease out whether the diffs are significant enough to warrant a ‘variant’ label (along with epidemiological data, of course). once identified and labeled, pcr can give you enough information (via the differing prevalences of short sequences of dna/rna that act like unique fingerprints) to tell the variants apart without needing to know anything about the structure.
yes to all. the early days of biochemistry were heavily dependent on x-ray crystallography, meaning the subject structure was in crystalline form, meaning there was a bias toward understanding of structures that facilitated crystalization. sequencing and structural studies[folding] were slow tedious wetlab efforts until mid 90s when computing power was of caliber, and shared across the internet, we now have such computation cheaper smaller, and locally.
like any jigsaw puzzle, the more pieces correctly placed the easier it becomes to progress.
I didn't see any information about this variant's ability to infect those with immunity from previous infection. Did I miss it, or was this rather important question completely out of the scope of this study?
Yes it is outside the scope of this study. It looked at behavior of the variant in a test tube. The results suggest that the question you raise is a natural next line of inquiry. But it won't likely be performed by this group, they are test tube researchers, that question is answered by number crunchers.
I remember getting downvoted a while back, but my suggestion has been to have people get vaccinated and then give them a small dose of coronavirus thereafter. At the time it may have seemed wild, but now it has been proven to be the most effective immunity.
> At the time it may have seemed wild, but now it has been proven to be the most effective immunity.
It's wild because immunity is useful for preventing infection (also, reducing the severity of infection). There's little point catching the thing you don't want to catch in order to prevent you catching it, because you still. suffer. the. harm. of having been infected.
There are way better options, like third doses of vaccines. Or revising the vaccines for Delta. Besides, if you want something 'like' a small dose of coronavirus, it would be far safer to attenuate the coronavirus first. Then you just have a classic vaccine.
The study shows natural immunity with a single dose is the most effective. I have little faith in a vaccine that can't be trusted to mitigate a controlled infection. What would be the point of the vaccine if it only "might" help prevent infection? Otherwise, if it is only effective %5 of the time but has nasty side effects 1% of the time, then you're taking a much bigger risk don't you think?
Wow, you really do want to condition people to ignore or disregard anything someone says as long as you say antivax. It is like the word Nazi. Doesn't matter what actually happens, you'd want to be able to call someone a Nazi and have someone mindlessly punch them in the face.
A vaccine preventing the seriousness of infection is a precondition. If I get a vaccine and it does nothing it is pointless. While most vaccinated act like political drones, if you told them than the vaccine actually does nothing to prevent the spread and vaccinated people are still frequently dying from COVID then I'm sure a lot of them would not be getting it.
Has it? I thought there was promising result with catching COVID and then being vaccinated (though you've already caught COVID, so you've failed the whole "don't catch COVID" objective), I wasn't aware there was good research for the opposite.
Like most things with COVID they didn't test the other way, but it is thought to be as effective and more so in order to prevent an initial serious infection, especially if timed adequately with the body has produced maximum resistance.
Will the body actually generate antibodies to other covid proteins in that case or will the existing antibodies against the spike protein destroy covid before new ones have a chance to be developed?
Great question. Isn't the reason the delta variant is so effective at infecting (mildly) already vaccinated people due to the fact that the immune system (unexpectedly) doesn't produce antibodies for the broad structures in the spike protein? My understanding based on a few papers I've read is that the immune system was more efficient than anticipated, and tended to produce antibodies based on specific structures that are part of the spike protein. Apparently, evolving an entirely new spike protein would be implausible, but mutations on the existing spike protein are more frequent, and this narrower than expected antibody is slower to bind to these.
The silver lining with Delta is it's such a transmissible variant that it out-competes the more slowly spreading but more vaccine evasive variants. I hope we never see a more transmissible one than Delta
We're also about to discover what happens when people don't exercise their immune systems for 2 years. There's a "super cold" of some sort going around in the UK [1] which, while not COVID (and therefore is probably not vaccine-sensitive wrt vaccines designed for COVID), has similar symptoms and is a lot more severe than a normal cold.
Normally you'd get colds 2-3 times a year (there are over a billion cases per year in the US alone), sometimes without noticing. These would "boost" your immune system from time to time and afford some limited protection against severe disease. That did not happen over the past 18 months for a lot of people, especially in countries like UK/NZ/Australia which went way overboard on lockdowns, to the point where there was no "flu season" last year.
I bet US will fare better just because enforcement is relatively lax, and 190M people already had COVID [2] (probably due to not really observing any lockdowns or whatever).
Heterologous ChAdOx1 nCoV-19/BNT162b2 vaccination, which was previously shown to augment neutralizing antibody responses against VOCs compared to corresponding homologous vaccinations [7, 10], might offer robust protection against the A.30 variant.
It's important to point out that many scientists were called conspiracy theorists by mainstream media after predicting (long before the vaccine rollouts) that mass vaccinations would cause the virus to mutate faster and that we'd all be worse off (as is clearly the case)...
Mainstream media and big pharma are corrupt. The people responsible are criminals and should be brought to justice.
COVID19 is not lethal for the majority of people. We will all die of something eventually but if some people are particularly fixated on COVID19, they are welcome to spend more time at home (instead of going out to meet people) and they can try to find remote work or some job which doesn't require so much contact with other people.
Anyone could easily bring their risk of catching COVID19 to nearly 0% by limiting social contact, proper distancing, hand-washing, mask-wearing, choosing the right kind of job (or retiring), getting plenty of sunlight, vitamin D supplements, living outside of urban centers, not travelling too much, etc...
All of these things are going to be way more effective at protecting individuals from COVID19 than any vaccine and these things don't require ruining other people's lives.
Also, if you don't want to risk dying of COVID19, you can just go live in a remote village/town; nobody is forcing you to live in a densely populated city.
Big cities are reservoirs for the COVID19 virus. Other people can kill you; this is a fact of life which we have to accept.
If you choose to constantly surround yourself with many people, then you're taking the risk, nobody else owes you protection from whatever viruses they may harbor inside their bodies without their knowledge.
The hospital system will be fine. If hospitals become too crowded with COVID19 patients; they can just start turning them away! People will come up with solutions; temporary/makeshift COVID19 hospitals, home-delivered ventilators, etc... Maybe governments can fund this if it comes to that?
Except the live in the remote town, your other points have been refuted and are easily disproven with some basic research skills.
My home country with silly low vaccination rates just introduced 8pm curfew last week, a neighboring country is sending additional ventilators, routine healthcare and surgeries have been stopped, government is making plans of sending patients abroad if the infection and hospitalization rates don’t change and they’re now talking about targeted mobilization to help healthcare staff, who are crunching insane hours to save people lives.
But hey ho, “Honey, come look! I’ve found some information all the world’s scientists and doctors have missed.”, said an HN commenter.
Just makes me sad.
If you think you’re the smartest person in the world, you need to look in the mirror twice.
There are clearly people in positions of power at pharmaceutical companies that need to be brought to justice. The Opioid epidemic, Johnson and Johnson's issue with talc/baby-powder... It's disgusting. And yes, individuals can take a certain amount of responsibility to limit their risk.
> The hospital system will be fine. If hospitals become too crowded with COVID19 patients; they can just start turning them away! People will come up with solutions; temporary/makeshift COVID19 hospitals, home-delivered ventilators, etc... Maybe governments can fund this if it comes to that?
If someone has a 'needs to go to a hospital' case of covid, if the disease is affecting their lungs and body poorly enough, then they will need attention from people who have medical degrees. If they are all busy working in overcrowded hospitals which are in triage / ration-care mode, who will staff the alternative care solutions you've outlined? Especially if hospital demand outstrips hospital supply?
There is so much wrong with this. Let's start with the apparent numbers you are accepting. Millions of Americans will die directly from infections, millions will need life support, and an additional ten million will die as a direct consequence of an overwhelmed health care system.
With those numbers it's hard to imagine a family not hit with these enormous consequences, where you seem to gloss over.
Secondary, the virus has no will of it's own, it will just randomly mutate, and if a stronger variant appears it will do so, if there are vaccins or not.
However, you are advocating to roll the dice millions time more, just because there was already a very small chance this gets worse, and you think that is a good idea?
At least 329 million Americans will die over the next 100 years no matter what we do; that's 3.29 million per year on average. So far less than 800K people died from COVID19 in almost 2 years... That's 400K per year; ~12% of all deaths... OK, this is a very rough/approximate calculation but is it worth ruining people's lives and taking away people's freedoms over a slight increase in death rate? This isn't the black plague. Personally, I wouldn't accept any significant change in my lifestyle for anything less than 100% (2x) increase in my chance of death... So I won't even bat an eyelash over a 12% increase (and I'm in a not-at-risk group so it's probably way less for me); and especially if I have some control over the risk... Some smokers take on much bigger risks by continuing to smoke; the risk is worth it to them - Who are we to judge?
This pandemic has been blown out of proportion. The media emotional 'contagion' has had a bigger negative impact on people's lives than the actual virus. Did everyone suddenly forget the emotional 'contagion' study which Facebook did some years ago? https://journals.sagepub.com/doi/full/10.1177/17470161155795...
The result of that study was that people's emotions could be manipulated without their knowledge... How do we know that what we're dealing with now isn't just Facebook and the media putting the results of that study into practice? It sure looks that way. I can definitely feel myself being manipulated by the media and I suspect that others who are more suggestible than me are even more so and less likely to notice it...
Using your math, there have been 738k deaths in ~1.7 years, or roughly 434k deaths per year yielding 15%, or 1 out of 6 deaths.
I just want to point out that death is not the only bad outcome of Covid. Medical researchers are finding evidence of memory loss and brain fog, long term disability, and long recovery times. https://www.foxnews.com/health/covid-side-effects-could-incl...
Also, 2x chance of death is a pretty high threshold! (I don't mean any criticism, just surprise.)
But this all focuses on the role of an individual and not the on role of a community. Smokers don't just harm themselves; second-hand smoke harms other people. Indoor smoking bans are for communal health, they aren't primarily meant to impact the individual smokers, who just go outside. Similarly, Covid-19 harms others if they get infected, and it also harms people who have put off non-emergency surgeries when hospitals are overcrowded.
..
Re: Emotional Contagion. If I remember correctly, the effects that were reported in the Facebook study were small, on the order of a change from 5.1 to 5.3 positive emotion words. (But it has been a while, so take that with a grain of salt.)
> How do we know that what we're dealing with now isn't just Facebook and the media putting the results of that study into practice?
This is an interesting question. Consider that lumping 'the media' together with Facebook means that most media outlets in every country (hundreds of thousands of people with their own agendas, political slants, biases, motivations, and who don't speak the same language) are now cooperating with one of the few companies widely credited with decimating newsroom web-traffic and by extension newsroom profits.
How well does this variant evade natural immunity-induced antibodies, which includes not only antibodies vs. the spike protein but vs. the body of the virus as well?
The question is are outcomes in vaccinated people comparable to flu - if yes - we can freely ignore it. Or people that have natural immunity. Or unvaccinated.
I have a bad feeling that with focus just on antibodies we're ignoring the important metrics. Which is outcomes.
The outcomes are pretty clear already, 10 times more official deaths globally compared to a bad flu. And we know the official death counts is under-counted by a 4x-10x factor.
> And we know the official death counts is under-counted by a 4x-10x factor.
Or it could be overcounted by a sizable chunk too. Nobody really knows the actual count and we probably won't until the dust settles and cooler heads prevail. The only thing we can do at this point is take the numbers we have at face value.
It would be very surprising if death counts were overcounted by a lot, because excess mortality rates have spiked massively since COVID-19 hit the scene, and in general are higher than the COVID-19 reported death rates.
So, for it to be overcounted, you would need to have an explanation for the reason that not just the recent excess deaths not attributed to COVID-19 have jumped so much, but that the 'real' causes of death have overshot and bit into the COVID numbers.
> And we know the official death counts is under-counted by a 4x-10x factor.
Not even California undercounted that much and they are among the worst under counters in the western world, if we compare Covid deaths to excess mortality. Death undercounts are closer to 30% at worst.
If I remember correctly, that number is true of the US. Globally speaking, The Economist has it pegged at 3.9x. A far cry from 10x, but also a far cry from an undercount of 30%.
> Taken together, the researchers found that excess deaths were estimated to be in the range of 3.4 million to 4.7 million - about 10 times higher than India's official Covid-19 death toll.
But that question is far harder to answer than testing the viral proteins in a lab. You seem to be dismissing this research whilst suggesting they concentrate on something that is probably impossible, thankfully, due to the fact that this variant hasn't spread much.
Sure, it's hard to test things in real world conditions, but that doesn't mean we should over extrapolate from in vitro findings. In particular, infecting cells easier in a lab doesn't mean the virus spreads from person to person easier.
Besides, the fact this variant hasn't spread much is telling in and of itself! Maybe we got 'lucky'. But maybe it just isn't that contagious, compared to Delta.
Is there any significantly contagious and deadly disease where natural antibodies have proven more protective than large-scale vaccination? Measles? Polio? Diptheria? Flu? Mumps? Rubella? Hepatitis? ...
Dengue. The initial vaccine did not target all subtypes of dengue, causing "severe dengue" in infections after a naive individual was vaccinated. The same could happen if someone moved from one region to another, since the subtypes inhabit different regions. Your body will respond to one subtype's antigens primarily with it's initial conditioning. If you weren't conditioned with that subtype, you get original antigenic sin / severe dengue
The worst-case scenario for a vaccine is not "no immunity", it is negative immunity. If your adaptive immune response outcompetes your innate immune response in binding to antigens, but does not neutralize them, then your immune system will struggle to fight off an infection
I worded it poorly (and it wasn't really anything worth saying in the context of COVID), but:
A population with 5% naturally-induced/80% vaccine-induced immunity might see more spread of a new variant than a population with 25%/60%, however the total outcomes would still be better in the first population; so "less protected" was definitely the wrong thing to say.
Naturally-induced immunity for COVID is stronger because it targets more than just the spike protein, and it presumably[0] grants better mucosal immunity than our current vaccines induce, but of course the risk/cost of natural infection is very high.
The great imbecility pandemic of 2020-2021. People who have experienced severe symptoms, hospitalization and deaths of relatives came out smarter than those who didn't.
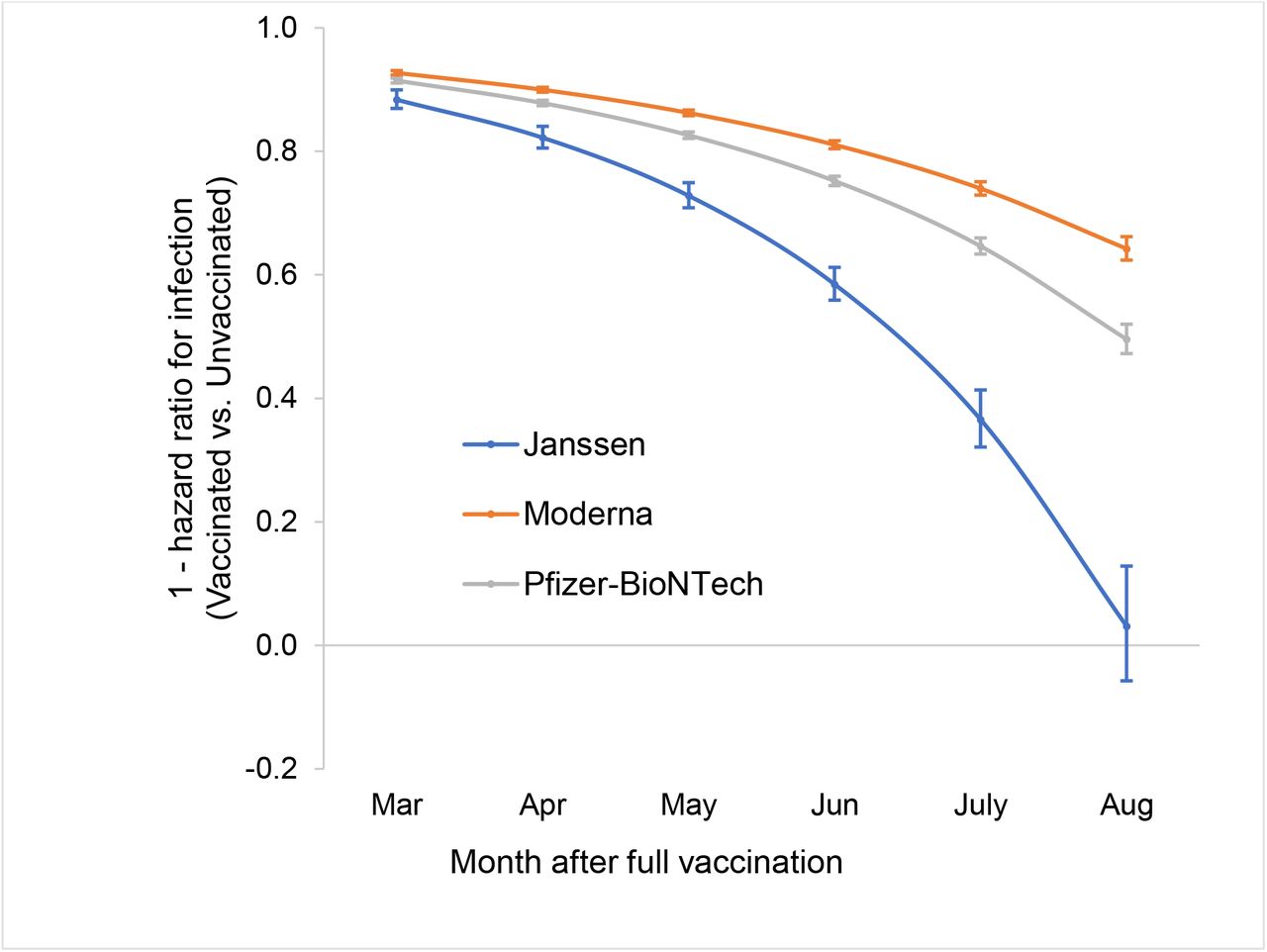{kind=link}
That is, a vaccinated person could be exposed to a variant for which they are partially protected, not notice clinical symptoms, while the person's immune system still remembers the details of the variant.
As an iterative process, this is akin to software updates (for a running immune system).
So to say that variant A.30 isn't covered by the mRNA induced spike protein antibodies is a very different statement than to say it's able to evade an immune system primed by mRNA antibodies which then re-entered daily life and thereby was able to continuously adapt to variants.