You are misunderstanding the CEO's statement. It says that 95 days are sufficient to make the vaccine, it does not mention testing. You cannot assess the lifelong effects of almost anything in just three months.
Thanks for the correction. I find it strange to believe that 12 months are sufficient to assess the lifelong effects of an immunity system intervention.
Uncertainty is a fact of life and decision making under uncertainty an important skill to be successful.
And in case it is not clear, in this thread I am not advocating neither for or against vaccines, so we can end it here unless you have something of substance to add.
Do you mean in terms of protection, or side effects?
In terms of long term protection, I don't think we really know yet.
In terms of long term side effects - do we know of any past vaccines with notable side effects that only became known after 12+ months? Genuine question.
In term of protection. For starters, if vaccine effectiveness were holding, there would be no need for boosters.
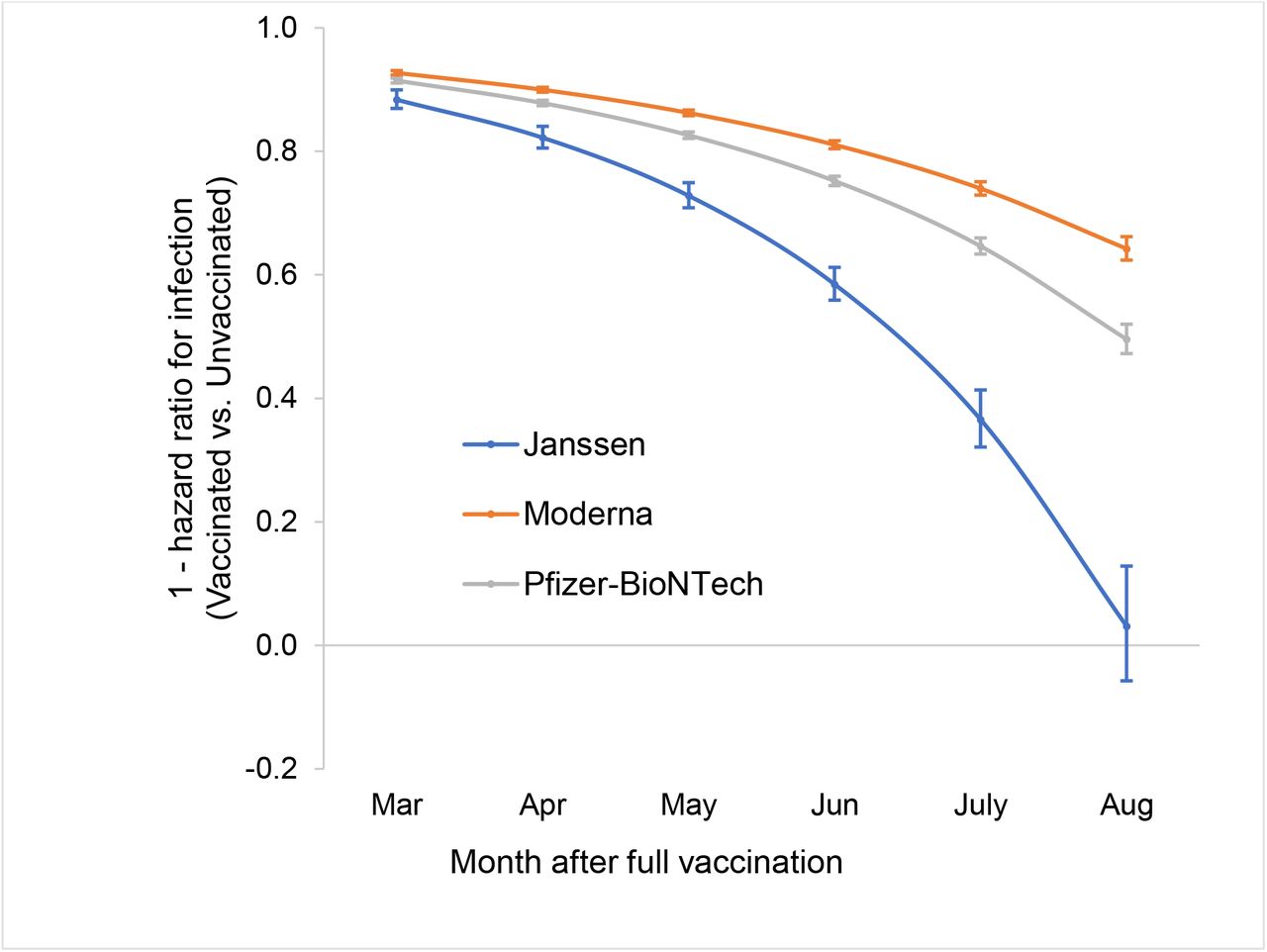
A picture from a recent preprint of 600k veterans over 6 months shows troubling VE against infection curves. J&J VE against infection is gone. Pfizer curve is just 2 months behind, at 53% and dropping.
Fortunately VE against severe infection holds much better at 77% Pfizer for June-Sept 2021 time period. The clinical trials claimed 94%, so there is a drop there. Nobody knows what will be the VE against sever infection a year from now, and we appear to have decided to preemptively boost so we might never know.
Alas, none of this takes in account future virus variants and their interaction with OAS. OAS means that building an immune response against the virus today will prove ineffective for a virus variant 10 years down the line. The worst known scenario was encountered with dengue fever. An excerpt from a 2011 paper summarizing the dengue situation:
"Original antigenic sin has the advantage that a response can be rapidly mobilized from memory. However, the downside is that in some cases, such as dengue, the response is dominated by inferior-quality antibody. In influenza, original antigenic sin has been shown to reduce the effectiveness of vaccination (13, 34, 51). In dengue, the effect of original antigenic sin has considerable bearing on vaccine strategies. Once a response has been established, it is unlikely that repeat boosting will be able to change its scope, meaning that balanced responses against the four virus serotypes will need to be established with the first vaccine dose."
>Fortunately VE against severe infection holds much better at 77% Pfizer for June-Sept 2021 time period. The clinical trials claimed 94%, so there is a drop there.
The clinical trials were run against the original version, while the data you presented seems to be overlapping with the spread of Delta, yet you never mention Delta in your comment.
I am a concerned citizen and parent. I only have so much time to write a well source comments. I wish people were applying just as much critical carefulness with regard to CDC publications. Where is the CDC longitudinal VE study? Do they even track VE data over time? Why do I have to sift through data instead of "the experts"?
Let's look at the weekly UK vaccine surveillance report, week 36 vs. week 42, afaik both within the UK Delta wave. For VE against severe disease, let's look at 'Deaths within 28 days of first positive COVID-19 test by date of death' tables. Let's pick age group 40-49 (older parents) and compute VE = 1 - vax_ratio / unvax_ratio.
Notice something? Same for all other age groups. Same for all the intermediate VE reports. A small but constant gradual VE decline.
FWIW, none of this makes me any happy. I wish the vaccines were holding effectiveness, that we didn't need a booster within 1 year of the initial shots and that the pandemic was over. Alas, reality does not cooperate.
It's not so simple, you need to look at the total number of people in each age group or you may fall victim of Simpson's paradox [1] (as both of those reports say):
> These data should be considered in the context of vaccination status of the population groups shown in the rest of this report. The vaccination status of cases, inpatients and deaths is not the most appropriate method to assess vaccine effectiveness and there is a high risk of misinterpretation. Vaccine effectiveness has been formally estimated from a number of different sources and is described earlier in this report.
In particular, the reduction of death rates among non vaccinated over time may be caused by natural selection, i.e. the weak died already while the remaining ones have unusually strong immune system (aka survivorship bias [2]).
There may be other unaccounted confounders, too, such as a change of behaviour over time where the degree of change is dependent on the age group and/or vaccination status. For example, an apparent reduction of effectiveness for younger people may be caused by them going back to work/study, thus increasing their probability of getting infected, while older folks staying in care homes as before.
Funnily enough, both Simpson's paradox and uncorrected confounders can result in observed correlations that are opposite to the real causality effect.
And to clarify, I'm not saying your VE numbers there are wrong, just warning readers about the dangers of statistics.
I agree! Another reason why VE appears to decrease might be that the ratio of unvax population with prior infection might be growing, and it's a wash between vax and post infection natural immunity.
OTOH this is not an isolated data point. We have: the booster push (why?), the veteran study, the PHE data. Something doesn't add up. For whatever reasons, the observed epi VE, after all the confouding factors are accounted by reality, is fading for both infection and severe infection, though VE agains severe infection is fading at a slower rate. To the point of J&J VE against infection (the weakest of the bunch) being almost gone in 6 months. I don't have a time machine, but I'm really interested to see how the Jan 2022 VE numbers hold up across the board.
Given OAS concerns (please re-read the dengue study excerpt I already quoted), near zero covid risk for kids, rapidly fading VE against infection and the general lack of long term data about covid & immune system (no time machines), what exactly is the rush to vaccinate kids against the original variant?! And why do we pretend we can just tweak vaccines to any new variant, when, while technologically we can concoct any protein we like, the immune system doesn't turn on a dime?
{kind=link}