Plus, to preemptively address any assumptions that Dr Jetelina may have an optimistic bias, compare her "There is good news" article from 5th January, which is based on what we now know, with her article from 26th November when Omicron (initially called "Nu") was first detected: "New Concerning Variant: B.1.1.529" https://yourlocalepidemiologist.substack.com/p/new-concernin...
At the time, little was known about this new variant except that it was extremely different from all that we had seen before, which would very likely result in escape from prior immunity, and may even lead to more severe disease (or not?). The only definitive silver lining that she found at the time was that 1) the variant could be quickly detected with PCR thanks to its S-gene deletion, 2) it was detected early thanks to South Africa, and 3) vaccines could be quickly adapted if necessary, thanks to mRNA vaccine technology. However, in all other regards, the variant was still very concerning.
In other words, do take her cautious optimism seriously. She's not a wishful thinker. Rather, she is a specialist in the field who works with the data as it becomes available and knows how to interpret it
" We can easily see that in many graphs, but my favorite is below from New York City, showing a clear distinction in hospitalizations among vaccinated compared to unvaccinated people"
I don't see this as much here in Ontario. Among the vaccinated as of today there is a 10.10/100k hospitalization status vs 16/100k for the unvaccinated (and 11.9 for one-dose). The hospitalization rate among the vaccinated is climbing quickly. Yes, there's still a gap, but yikes.
ICU is better, though, with a 0.76/100k rate for the vaccinated vs 4.74/100k for the unvaccinated.
This may have to do with different hospitalization and testing criterion, I don't know. But hospitalization here is in full exponential growth and not just among the unvaccinated.
Obviously being vaccinated is still far preferable. I have had 3 doses (1 AstraZeneca and 2 Pfizer) FWIW.
Simpson's Paradox applies here: once you slice by age, the data tells a different story. Even when vaccines are highly effective, the confounding factor that gets lost when you aggregate across ages is that the most vulnerable (the elderly) are also the most vaccinated.
I highly recommend anybody concerned about hospitalization among the vaccinated read this post. It's about Delta hospitalizations in Israel 2021, but we should expect the same effect from Omicron and across countries: https://www.covid-datascience.com/post/israeli-data-how-can-...
That's not the metric you should look for (at least you don't need to). You should look at the average age of unvaccinated people. That way you can estimate the prior probability of infection.
From that, you can figure out that there are more people unvaccinated under 12 years old, than in the entire rest of the population, by a large margins - out of 7.6 million people without full vaccination, 2.9 million are between 5 and 11 years old, and 1.9 million people are under 5 years old.
So out of the 7.6 million people who aren't fully vaccinated, 4.8 million are under 12 years old!
And from 2.8 million remaining, 430k of those are under 18, and 1.0 million are under 30.
From this, we can figure out that the pre-vaccine hospitalization risk for the unvaccinated population is much, much lower than for the normal population.
This is without taking into account health status, of course!
Its good to see that its mostly young people who are at lower risk that are of the unvaxed, however the majority of ICU cases in Canada are still of the unvaxed, so that's why I am curious what is the average age of the unvaxed in the ICU. If 92-99% of people over 60 are vaxed, but its the 60+ demographic of unvaxed taking up ICU spaces, what more can be demanded by the government? Forcing younger people who are unvaxed might not reduce ICU cases very much.
This still shows a greater than 10x difference in outcomes. Additionally, the "unvacccinated" population includes people naturally vaccinated by virtue of having a previous case.
It could very well evolve into a form that is mild enough and different enough from the vaccine spike that brings the unvaccinated and vaccinated hospitalization rates to convergence. Respiratory illnesses in general harm the elderly and immunocompromised disproportionately. But if that becomes the end game where COVID is still circulating, vaccines are no longer as effective at preventing serious illness, because the general severity has gone down, that is also a good outcome as it is what we have always lived with.
Colds and flus have always killed 10s of thousands a year. COVID killed many more because it was particularly severe. Just as the flu of 1918 is still with us today in a less harmful form (H1N1) This virus has a global reservoir and will never run its course entirely before mutating again most likely. Just like colds and flus before it.
> "COVID killed many more because it was particularly severe."
no. covid is novel, not appreciably more severe, and that's where mortality rates are coming from. it's following the dynamics of the many cold and flu viruses that came before it. we just happen to be at the beginning of the dynamics rather than at relative steady-state (e.g., 'endemic'), which is where most other viruses are at.
this inability to reason cogently about steady-state vs. dynamic aspects of systems is absolutely rampant across media, politics, and casual conversation, and must be a named fallacy at this point, though i don't know that name offhand.
It is? Care to source some data on these 'dynamics'?
You are engaging on wishful thinking I'm afraid - wishful thinking that is even now still killing hundreds of thousands. Perhaps there is a name for that too.
The best available evidence indicates that another coronavirus HCoV-OC43 probably caused a worldwide pandemic and killed a lot of people starting in 1889. The same virus is still endemic today and the only reason it doesn't take a huge death toll is that most of us get infected when we're young and the resulting natural immunity protects us as we age. But it and other endemic coronaviruses can still be quite deadly to frail and immunocompromised patients.
"Additionally, the "unvacccinated" population includes people naturally vaccinated by virtue of having a previous case."
Only if it's recent. How recent isn't clear yet. Somewhere in the > 90 days, < 1 year range, it seems.[1] As of last summer, about 1% of COVID cases were known re-infections.[1] Most repeat cases seem to involve two different variants.[2] Whether people who had previous variants are showing up infected with the omicron variant doesn't appear to be published yet.
This virus has a global reservoir and will never run its course entirely before mutating again most likely. Just like colds and flus before it.
Maybe not. A much broader vaccine is coming along well.[1] That's from the US Army's Walter Reed Medical Center, and it just passed phase I (safety) clinical testing. That one is supposed to protect against all COVID & SARS variants.
There are 93 more COVID vaccines in development at the moment. Some are pills. Some are nasal sprays. Something is going to work. What we have now is the minimum viable product, and even that is pretty good. Early on, there was concern that a 50% effective vaccine was all that would result. Which is about where the original Sputnik vaccine, and the original SinoVac, are. Instead, we got 95% effective vaccines in round 1.
The Ontario science table dashboard has the hospitalization ratio for unvaccinated to vaccinated still at 5:1. Where are you getting that these rates have become nearly equal?
> Ontario science table dashboard has the hospitalization ratio for vaccinated to unvaccinated still at 5:1. Where are you getting that these rates have become nearly equal?
If the rates are the same, and 5/6 people are vaccinated, we would expect 5/6 people admitted to the hospital to be vaccinated. In fact, 5/6 people are vaccinated in the 12-40 age cohort, with older (and more vulnerable) populations having at least 9/10 people vaccinated and quickly going to 19+/20. Therefore, vaccines prevent hospitalizations, as the average of all adults is greater than 5/6.
You're misunderstanding. The dashboard is per Capita (so you don't need to account for the stuff you're describing), and shows 5x lower rate of vaccinated people hospitalized (and 10x lower ventilated). A far cry from the ~1.5x rate mentioned by ggp
Corrections: My above post was written in response to the unedited version of the GP post, which stated the 5:1 ratio was vaccinated:unvaccinated (and implied it was based on total numbers). Apparently, since I posted it was edited (and corrected) to say it was 5:1 ratio of unvaccinated to vaccinated (and based on per capita.) This makes far more sense and also makes my reply look insane.
I take GP at their word that there were just errors in writing their post. But it does leave a weird artifact out there that I cannot fix.
ontario still conflates anyone hospitalized for anything testing positive for covid, with anyone hospitalized from covid; this alone could explain the discrepancy between a hospital bed and icu. lies damned lies and statistics...
It’s not that simple: yes, if someone gets in a car crash it’s probably not COVID but there are many cases where someone had a manageable condition that was disrupted by COVID — not 100% fault but not 0%, and a big problem for hospital capacity.
My guess is because it was not a counter-point to what the previous poster wrote. Although what they wrote does not exactly address the comment being replied to either.
Comparing the rates only makes sense if one believes the risk is distributed equally among the two populations. However, the most vulnerable are the most likely to be vaccinated, and the least vulnerable are the most likely to be unvaccinated, so the vaccine could still be very effective even if the rates of hospitalization are equal, or even worse for the vaccinated population.
My guess is that this speaks more to the cheapness of hospitals in Canada and the greater likelihood to go to a hospital with a lesser case of COVID. For instance, you quote a 7.6% rate of the vaccinated moving from the hospital to the ICU and a 29.6% rate of the unvaccinated moving from the hospital to the ICU. Meanwhile, the US blended average seems to be around 30% (eyeballing the data.) That could be because the unvaccinated are an overwhelming percentage of the admitted (it's the same rate), or it could be because there is a higher bar to go to the hospital at all for either class.
Thanks for this, just in those two blog posts she answered many lingering questions I had about how omicron has been changing things. the SEOd google results are always a flood of incomplete or speculative information when I try to find answers to covid questions so this is a dream come true.
If anyone has any other sources like this that can find and interpret good data for covid I'd love to hear about them.
> I think thought-leaders and experts could use a whole lot less deification right now
I'm not sure that's possible - the experts are more or less screaming into the wind at this point. The WHO and the CDC have been reduced to punchlines by liberals and conservatives alike. IMHO this scorn is well-deserved.
I'm not a big fan of this new trend of some random Twitter personality suddenly becoming the go-to source of information on COVID.
Granted, it seems true that she's actually an epidemiologist, though not unusually notable as an assistant professor at a mainstream state school. As far as I know she doesn't have unusual access to information, or a hands on role, she's drawing from public sources and doing analysis.
Which, is fine. But what makes me nervous about this trend is that she's now like almost a household name. She's built a personal brand around this image as being the up to the minute source of information, and the audience she's developed has a certain profile. They're basically looking for someone to tell them how bad everything is and how scary everything looks, backing it up with details so her audience can feel smart when they relay all this info to their friends.
The minute that COVID isn't actually something to worry about her audience is gone and she goes back to being a random obscure civilian.
Which is an incentive structure that makes me pretty sure I know what she'll be posting tomorrow, and a week from now, and so on.
I realize the mainstream news media isn't any better. But still, it's an odd new development that people are mostly seeking out the level of fear/concern they want in their news rather than the other way around.
> though not unusually notable as an assistant professor at a mainstream state school.
We really, really need to get away from this academic obsession with prestige. If she does solid analysis and communicates it effectively, with a record that looks increasingly good as time passes, she's already ahead of the curve. Meanwhile many other highly-credentialed, prestigious experts have been wrong over and over and over again in this pandemic.
Academic/scientific institutions are polluted by the credentialisim/prestige focus. It's the ugliest aspect of the whole space.
If it matters almost the same thing has been happening in my country (Romania), only that around these parts of the world we have FB as a replacement for Twitter.
I personally regard it as a coping mechanism for the people that follow these newly created Covid personalities, the bad thing is that in most of the cases the mainstream media copy-pastes those posts/messages and presents them as the truth, even though there are many devils hidden in the statistical details most of the time.
> In certain jurisdictions, though, we’ve met or exceeded last winter’s hospitalization peak. We can see this in many states in the Northeast, including New York.
When presented with a new source, I tend to judge people based on their perspectives on things I know about. This one is a case study in being misleading, while not technically lying. New York state has only "met" last winter's hospitalization peak if you look at trend lines. If you look at hospitalizations per day, we clearly haven't. Also, of course, "last winter's peak" was not really any sort of stress for the hospital system at all (compare to the spring 2020 wave, which was), and it happened at a time when things were much more restricted than they are now:
...but it's still misleading, because again, this is a fraction of previous waves in NYC, but also, a lot of these hospitalizations are going to ERs for testing. Government officials are pleading people to stop going to the hospital for trivial things:
I don't know if she is intentionally trying to mislead, or just doesn't have a good handle on the data, but this is the sort of thing that makes me skeptical of a person's other claims.
> But it's still misleading, because a lot of these hospitalizations are going to ERs for testing.
I don't think this is correct. Going to the ER is not the same as being admitted to the hospital. From everything I've read, ER visits are not counted as hospitalizations anywhere.
> Hospitalization counts reflect the total number of people with COVID-19 ever admitted to a hospital, not the number of people currently admitted.
If you go to the ER and make it to a treatment area, you're admitted. These are bright-line distinctions. Nobody is making judgment calls on the data ("did this person really get admitted, or is it just someone in the ER for an hour? Let me look at the chart!") at this level of analysis.
Really? Is this a NYC thing? Any hospital I’ve ever been in has considered the ER an outpatient service, and you are only admitted to the hospital if they transfer you from the ER to inpatient care. Do they consider other outpatient services, like, say, yearly physicals, an admission as well?
I can't speak to outpatient services, but hospitals report this data, and make the call. The government doesn't do it -- which is what you'd expect. It's hard and slow to make case-by-case judgment calls when you're far from the source data. Hospitals, in turn, don't spend any more time than is absolutely required making these kinds of classifications, unless someone makes them do it.
It would not surprise me at all to find that other cities/states have the same thing happening.
Just a thought after reading the good news - ok this is great for the US and the west where there is decent vaccination.
What the hell is going to happen with the omicron spread in countries with hardly any vaccination? I mean if it really is like measles, this could be terrible.
Not an expert but comparing countries is hard, especially now that there are other factors such as how many people are vaccinated, boosted etc. I don’t think it’s obvious from one country how another will fare.
It's been getting to the point or already is that you can't get treatment. Plenty of urgent care centers are simply closing down for now. Hospitals won't even treat covid.
Surely this is the end of the pandemic? With an estimated 300k+ cases per day here in the UK, that is 10 million this month on top of everyone who has already had it. It’s as though nobody is ready to acknowledge the elephant in the room that Covid is nearly finished.
You're missing the fact you can catch it over and over. My wife is currently battling Omicron after we both had covid at the start of last year. Fully vaccinated and boosted three weeks ago, caught it anyway. With an infected population this massive mutations happen fast enough to cause a new wave before the old one burns out.
I have omicron right now (4-5 months after 2nd jab, so pretty much no effect from that) and it's just like a common cold (certainly wouldn't call it "battling omicron"). I have zero problems with getting this each year.
Both my wife and I (double vaxxed for 5 months, not boosted yet although were just about to do so) caught Omicron-flavoured Covid in the lead-up to Christmas and it wiped us out each for 2-3 days each, with a combination of fatigue, aches, fever, and violent coughing. Certainly worse than any cold or flu we've had up until that point.
I still have a pretty nasty cough and a throat inflammation.
Congratulations. You haven't had a bad cold or flu before. It's not uncommon for the flu to knock someone out for a good week. Or for a cold to leave a lingering cough for weeks.
> It's not uncommon for the flu to knock someone out for a good week.
This is why it has a vaccine. That prevents it, prevent seriousness of symptoms, and deaths. (yet a large percent of the population doesn't get it, and so 50k us citizens die each year)
I have gotten a flu vaccine every year since I was 18. The worst flu I ever had was in January 2020. (I was tested and positive for influenza)
Fever for 4 days, horrible coughing, vomiting, barely able to get out of bed. Flu vaccines certainly provide some cross-immunity when the vax isn't matched to the strain, but not too much. That's what my doctor told me when I complained to her (when she told me I had tested positive for flu) that I'd gotten the annual flu vaccine the preceding October. Depending on the strain vs the vaccine for that year and how big of a mismatch it is, it can really whip your ass despite the vaccine. That being said, the flu shot is a good idea for anyone, and crucial for seniors.
We've been under threat of lockdown, under lockdown, or under restrictions for ~2 years now.
It's understandable that some are very concerned after or about getting sick but many of us, for our own sanity and psychological health, need to move on.
> We've been under threat of lockdown, under lockdown, or under restrictions for ~2 years now.
> It's understandable that some are very concerned after or about getting sick but many of us, for our own sanity and psychological health, need to move on.
WWII lasted longer, and IIRC the US was under a restrictive civilian rationing regime that whole time.
I understand that people can get annoyed with various measures required for the public good, but that's not good reason to "move on" from whatever challenge that motivates them.
Caught a bad flu in late 2018. Lingered for two months. Cough so bad, I dislocated a rib. Had X-rays taken, and everything. Took about a year for the the rib to stop slipping whenever I exerted myself. In the end, it was a period of discomfort that set me back a spell, but which I ultimately got over. Probably wouldn't try to shut down society over it, or use it as proof that people should fear the flu. Just that sometimes you get sicker than usual.
i had a similarly bad flu bout winter 2017-18. the worst of it literally had me at the edge of death one night. would have stopped breathing had i not willfully forced myself to, through all the congestion and soreness (also had a rib issue like you). the flu is no joke, and yet i also wouldn’t try to shut down the world, let alone my city, for the flu.
People forget that it knocks so many people down at once in a short time, and with quarantine rules in force. It is more contagious than flu/cold. Imagine what would happen every year in winter if this becomes the new normal.
Imagine what would happen if we go in lock down every year. And keep making kids learn remote. And keep letting governments gain more authority without the reasonable discussion
It’s terrible to feel terrible, but getting over the worst part of Covid in 3 days is an enormous improvement from how unvaccinated people fared in the initial waves. Even for people not hospitalized, they dealt with pneumonia and shortness of breath for weeks. I think we can celebrate the progress we are making in reducing the average severity of this disease and there are more tools coming soon with Pfizer’s new pill and newer multivalent vaccines.
According to the CDC, 30% to 40% of symptomatic people get shortness of breath, which is a significant share. That is a signal that the infection has reached the lower respiratory system.
Had I reported to the CDC (I didn't), I would have reported that I woke up in the middle of the night unable to take a deep breath, went nearly immediately back to sleep, and was free of all symptoms the next day. This would have counted toward the total (had I reported), and such counting needs a wider perspective before such things as say, creating lockdown policies based on these figures.
According to https://www.bbc.co.uk/news/health-59895598, over 500,000 people in the UK are still suffering health issues a year after catching Covid, and nearly 900,000 are still suffering after 12 weeks. The UK population is around 70 million, so that's around 1% of the entire population. If you take into the fact that many people in the UK have managed to not catch it at all yet, or exclude children who suffer far less (if at all), then the percentage would be higher.
The problem with a statistic like that is that it is pretty much devoid of almost all data that would make it truly meaningful and valuable. That stat tells us nothing of their health pre-Covid, and I’d bet a very large portion of that number were already dealing with health issues (which we already know significantly increases severe Covid). The meaningful number is how many formerly healthy people are battling Covid caused health issues a year later. My guess is that it is a pretty small number, likely small enough that it would be considered even by you to be a “small minority”.
Previous health condition status is part of the dataset, so you don't need to guess. If you want to take that into account, then use the data to make your point.
Thanks for the tip! I’ll let the dataset speak for itself:
“7. Health/disability status is self-reported by study participants rather than clinically diagnosed. From February 2021 study participants were asked to exclude any symptoms related to COVID-19 when reporting their health/disability status. However, in practice it may be difficult for some participants to separate long COVID symptoms from unrelated exacerbation of pre-existing conditions, so these results should be treated with caution. “
Yeah absolutely, I count ourselves reasonably lucky that we only caught the disease after vaccinations.
I have absolutely non-zero desire to go through this every year, unlike my parent commenter though.
Would I be of a similar opinion as parent if I had a similarly asymptomatic-to-mild case? I don't know for sure, but I would hope not, because I wouldn't want to draw conclusions or base policy from just my anecdotal experience.
Other replies to me appear needlessly partisan jibes: I neither said nor implied anything about continued lockdowns and any such inference is pure projection.
Your parent commenter wasn't saying that they have a desire to get this every year, just that if the worst case outcome is getting what they had every year, they would find that an acceptable trade-off for getting society back to normal.
> I have absolutely non-zero desire to go through this every year, unlike my parent commenter though.
Many people get sick every year or every other year. Their illness is like you described: 2-3 days of being "knocked out" and about a week to fully recover.
It's not that I "desire" to go through that every year or two, it's just life. I expect that's why people responded incredulously to your post: for them, getting sick occasionally is normal.
to add on — before i had kids i rarely got sick. at one point i went maybe seven or eight years. now, every couple months. and at least one a year that puts me down a few days or more. And those aren’t even the flu, typically. There are many kinds of colds that can knock you out.
Each is likely an endemic version of something that was far more serious and deadly historically. Now it’s a minor or major annoyanace that is part of normal life. i bet eradicating covid would fall into the same bucket S eradicating any of the others. Something to aspire towards, but until then something to simply accept as normal and move on with our lives.
By saying “I don’t want to experience this every year” without any caveats, there is an implication we should do something to prevent it. Especially given the broader context of the pandemic thus far. Surely you can see how many readers might feel that implication.
That sounds like a fairly typical cold, maybe edging to "bad" in my experience. I'm double vaxxed plus a booster about 1 month ago, and currently have Omicron. I have roughly the same experience as you, although less on the coughing, which is odd because I usually get a lot more coughing with colds.
I regularly feel "wiped out" from a typical cold, often for 4+ days in a row.
This whole thread is full of anecdotes from people implicitly claiming that their experience applies to everyone, when in reality everyone's going to have different experiences with everything from colds to covid. Unfortunately, the latter has a much higher prevalence of seriously-worse side-effects (long-haul, ageusia, anosmia, death, etc) compared to the former.
My 15 yo son got Covid about three weeks ago, symptoms matched what the parent poster described, including feeling "wiped out". Oh wait, no he didn't. Testing all came back negative. Diagnosis from his pediatrician: common cold.
Ah, yeah, you're right. It was probably just the cold that myself, my son, and my wife got after being exposed to someone that had symptomatic, PCR tested Covid. I'm sure it was just a coincidence that we then all three tested positive for covid.
technothrasher wasn't doubting that you had COVID, but rather making the point that the common cold and COVID now have the same symptoms and severity, and that getting a test is now the only way to tell which one you have.
Joint pain and being mentally "out" (not being able to hold complex structures in my mind = unable to code) are two hallmarks of common colds for me and why I always take ~2 days off work when I have one - I'd just get frustrated trying. Sore throat is another one.
Omicron now is no different. Ended up taking 3 days off work and am now back to normal capacity.
FWIW: To me, it sounded like an atypical cold or a typical flu. I've been "wiped out" by colds before, though rarely, and I'm always "wiped out" by flus, though I catch them a lot less often than once a year.
This is one of the most privileged takes I've ever read. OH GOOD HEAVENS. You were sick for a whole 2-3 days. Best lockdown the country to avoid what most people experience 1+ times per year.
Omicron didn’t kill 800 000 people. There’s also vastly more immunity (whether through vaccines or previous infections). Let’s wait and see but there’s hope it’s a different, milder disease.
(You are right of course. With the data we have now, we are quite certain that Omicron is much milder. Hopefully no lockdown is needed.)
But, personally, I would like to avoid getting Omicron, as long term effects are still unclear: does "long Omicron" exist, does it affect vaccinated, and if yes how common and severe is it. There are some recent news about long Covid: it could be micro-clots.
Unless you live as a hermit you are unlikely to avoid getting Omicron. A more rational approach would be to take steps that will maximize your odds of survival when you do get it.
Yes, like taking a vaccine. And also social distancing and avoiding others so that the peak of cases doesn't coincide with an overflow of Medical facilities resulting in your inability to get proper medical attention if needed.
so the answer is to stay locked down and screw over small businesses and tons of workers every winter because a subset of people have harsher symptoms?
Every policy has tradeoffs. We could save around 20,000 lives per year (in the US) with a simple policy change: just cap all speed limits at 45 mph.
I think it's a fair critique that some lockdown measures go too far (particularly those with low efficacy, or "safety theater"), but it's more helpful to take about specifics, rather than "lockdowns good" or "lockdowns bad".
At some point (and maybe it's now?), we'll need to shift our thinking from "pandemic" to "endemic". COVID is going to be with us from now on, and will start to look more like flu season (viruses tend to evolve to be less deadly over time). And I don't say that to trivialize it; COVID has given me much greater awareness of the impact of the seasonal flu on the elderly and the immuno-compromised.
I agree, that is my point is exactly. At a certain point, we need to learn to live with it. Majority of us on HN are in an extremely privileged position where we can WFH and infact for a lot of us, pandemic led to more savings. But that is not the case for an average person out there. There are families out there have been ruined financially for life because their business had to shut down. Kids very much might have life long repercussions from the school shut down. At a certain we have to take all this into account before just initiating a province wide lockdown every winter (which is what is happening in the country I live in, Canada).
My brother had mild symptoms after being unvaccinated. So did my kids. So did my neighbors whose kids play at my house all the time.
So did the vast majority of South Africans who aren't vaccinated.
I push the vaccine onto all my high-risk family members. I recommend it to anybody as a tool to introduce your immune system to the virus.
But let's be honest about this:
The vaccines in circulation were created to stop the Alpha variant. The immune system response is too targeted to antigens on the spike protein that are no longer present in the newly evolved, vaccine escaping variants. The vaccine is a useful tool for mitigating severe disease, but it's an outdated vaccine for a variant that no longer exists. Just like the a flu shot for the wrong strain tends to have some positive benefit when you catch a mismatched strain via some cross immunity, that's what we get from this vaccine. And guess what? We get it from infection induced immunity as well.
Plenty of unvaccinated (the vast majority, in fact) also experience mild symptoms. It's almost like you've got an unfalsifiable way to always say "it worked!"
> Plenty of unvaccinated (the vast majority, in fact) also experience mild symptoms.
This is true of essentially all diseases except some very very rare exceptions that also tend to burn out very quickly. That's just how disease spread works, mild cases help the virus propagate. It's not like the virus is a mustache twirling villain that wants to murder you, it takes a fairly specific balance to obtain long term survival.
> It's almost like you've got an unfalsifiable way to always say "it worked!"
There's plenty of evidence to support the idea that "it works", and actually quite a lot of evidence to contradict the idea that "it doesn't work". Severe outcomes are blatantly more common, per capita, in people who are not vaccinated. The only way you get to any other conclusion is if you just plain don't trust any evidence presented, in which case there is literally nothing that is falsifiable for you and you may as well believe covid-19 is evil unicorns or something.
I mean, it's pretty early to be drawing conclusions about this with omicron. Especially since it hit right as people in most of the vaccinated world were hitting 5-6mo since their second shots. That doesn't mean it's "unfalsifiable" it just means it hasn't been yet.
That said, I don't think the null hypothesis is suddenly "vaccines do nothing" for some reason. It's clear enough it spreads more easily but that doesn't suddenly invalidate all prior assumptions about the vaccines' effectiveness against severe outcomes.
Edit: I'm very happy to be proven wrong about this but I feel like people should direct some of these replies more to the person I was replying to? I'm not the one who thinks vaccines do nothing here. :P
It's only too early if, like our public health authorities, you are too bigoted and self-important to trust South African medical scientists because they aren't from a mostly white country. That's my take on why the CDC ignored their scientists, as did the media.
From the very beginning, the South African medical authorities were screaming that this variant was producing far fewer hospitalizations OVERALL (despite higher case numbers) than the delta/alpha did.
But because they are a third world country, and the news media in the West is biased towards bad news, they chose to treat this positive data as suspect. It the SA scientists had talked about how horrible it was, they would have taken it as gospel.
Those of us who were looking at the data knew otherwise.
I thought the issues were more about the younger population than in Europe and the US. And the unknown number of folks that had already been exposed to previous waves. Not the racial makeup of the people living there.
I was amused at the sudden acknowledgement of natural immunity from previous infection in the very publications that have constantly claimed it doesn't exist, the minute it supported their need to keep fear mongering. Same with the younger population point, considering these very organizations have gone out of their way to obfuscate the vast risk stratification by age for most of the pandemic. The terrified 20-somethings wearing respirators in TikTok videos are a result of this.
> I was amused at the sudden acknowledgement of natural immunity from previous infection in the very publications that have constantly claimed it doesn't exist
> I mean, it's pretty early to be drawing conclusions about this with omicron.
No it's not. Late November was too early. In mid-December we could start drawing conclusions. At this point things are becoming quite clear - we see similar trends everywhere, not just South Africa.
"The data suggests that three doses of vaccine provided an estimated 68% drop in the risk of being hospitalized with Omicron compared with people who were unvaccinated."
When you look at individuals, you'll never be able to truly say any treatment "worked" with certainty for virtually anything. It's same with nearly all medical treatments. Humans, very often, get better on their own with time, and time can't ever be rewinded to test the alternative.
The way we know a medical treatment works is by looking at large scale data, controlling for variables, understanding mechanisms of action, and by approaching this science in good faith and not cherry picking data to fit one's own conclusions. There's a concept known as "Number Needed to Treat" that is probably relevant to your concerns here.
Vaccinations have historically been extremely effective for many diseases, and COVID is no exception. It's accurate to say (most) "COVID vaccines are highly effective at preventing severe disease caused by the SARS-CoV-2 viruses". Omicron is so new that it's hard to be certain of anything regarding it right now, but we'll have a better picture in a few weeks. I do know that we're seeing many hospitals get overwhelmed across the US currently, and many medical workers are out sick with a COVID infection.
I have some skeptical family members who like to talk about 3rd party anecdotes. "A nurse told me she saw blah blah blah happen". As you say, stories like this are not a way to know a thing, but I can't get them to understand.
It's like we rolled a die once, and it came up 6, and now we're all forming our own special opinions on whether or not the die is fair. We just can't know. Of course, if someone rolled the dice 30,000 times and reported what they found, that would be great (wink wink).
Instead of using Calc 1 as a filter course, we should use Statistics instead.
Yet it is predominantly the unvaccinated who are overwhelming hospitals with more severe cases. In NYC it is something like 15x difference -- 30 per 100000 unvaccinated versus 2 per 100000 vaccinated people wind up requiring hospital care. Those may be small numbers, but with omicron clearly being both more contagious and evading prior immunity it rapidly becomes problematic.
On a personal level it's gonna be either 100% or 0%. You either got severe disease, or you didn't.
You can't extrapolate a population-level percentage from a single data point. Luckily, we've got information on hundreds of thousands of deaths, millions of hospitalizations, and billions of shots.
You can't get 15% of a case of severe COVID. At a personal level, the vaccine either worked at preventing it, or it didn't. We can compute a population-level probability of those two scenarios for you, but you can't really say "15% effective, after 2 jabs, for me personally".
Getting Covid or not is binary, yes, but the severity of the disease is on a spectrum. I can surely get a 15% less severe disease thanks to a 4-5 month old vaccination. Just like the severity of the disease depends on the viral load you're exposed to.
Of course there's no way of knowing what the exact percentage is for me personally, so in that sense you're right - it's just an average. But it's surely indicative, which is why you should be getting boosters after a specific amount of time, if you're in a risk group.
"Plenty of unvaccinated (the vast majority, in fact) also experience mild symptoms. It's almost like you've got an unfalsifiable way to always say "it worked!""
Yes, it's called 'Science'.
The vaccine absolutely helps to reduce symptoms, hospitalizations and death, even 5 months in.
There are millions of Omicron cases around the world measure up against various vaccinated and unvaccinated populations.
I have 5 people in the house, 1 vaccinated, 4 not.. the ones that were not had a 2 day fever... the one vaccinated (me) had no fever but just a cough for 3-4 days. All in all just like a mild flu
Anecdotal stories don't paint an accurate picture. I live in NYC and had Covid xmas week. It was ROUGH. (I'm double jabbed.) I also know unvaxxed people (0 shots) that just had a little sniffle and bounced back in 2 days. I also know of a seemingly healthy young lady that tested positive and died 3 days later.
> Anecdotal stories don't paint an accurate picture
You would have thought that after 800,000+ deaths in the US people would have learned the importance of understanding statistics when dealing with these issues, especially on a place like HN, but pandemic has melted people's brains and now people are arguing anecdotes about what constitutes a "bad cold" and a "mild flu".
The funny part is that it doesn't really matter because it's not like we get to collectively vote whether the pandemic will end or not. It's pretty clear that, even given how extremely contagious omicron is, people don't care as much as the used to about a seasonal flu.
Even supposing covid sticks around and becomes "only" as bad as the flu, 10 years ago if your said it was fine to double the annual cases of flu and flu death people would have said that was insane.
Sadly if people haven't learned to reason about these problems correctly now, it means they very likely never will.
> vaccine mandates were still in effect at that point, they'd say that was insane too.
No, that one is particularly weird right now. Vaccines are essentially mandated for many parts of life, and have been for my entire life. At multiple points throughout my development I've had to get required vaccines to do things. I had never even heard of antivaxxers until my late 20s. They used to be laughed at as an insane fringe group on HN.
Nobody in 2011 would have thought it was weird that vaccines would be mandated. I suspect if I predicted on HN that there would be strong resistance to a vaccine in the event of a global pandemic people would have laughed at me as ridiculous.
People don't like vaccines because they don't like the reality we're in and they strangely think resisting wearing masks and resisting vaccines somehow makes it less real. Unfortunately it has made things much worse.
> Vaccines are essentially mandated for many parts of life
Not ones requiring multiple jabs per year, seemingly forever (unless something like Omicron comes along).
Also not experimental ones rushed out with an EUA. Would you accept a mandate of the Chinese or Cuban vaccine, twice per year, for your whole family, for the whole foreseeable future?
> Nobody in 2011 would have thought it was weird that vaccines would be mandated.
You'd be very wrong. I remember very well that people were highly vocal against the H1N1 vaccine a decade ago and would've (rightfully so) lost their minds with mandates. Turned out the vaccine caused narcolepsy in kids[0], among other things. I never had that vaccine. My pregnant partner did (which turned out to be a lucky gamble).
> resisting wearing masks
Barring N95/FPP2+ masks it's mainly theater. It will be interesting to read all about this in a year or three once the heated political agendas have subsided.
Mandated vaccines for adults in the United States actually is weird and unprecedented in the modern era.
It's so unprecedented and unpopular an idea that everyone - including Biden - were falling all over themselves assuring us they would under no circumstances mandate the Covid vaccine.
tl;dr Vaccine effectiveness around 15% for me at this point. So it was the natural immune response (gasp!), combined hospitalization rates across the world reflects this.
Comparing death rates in Australia, which actually did pretty major lockdowns, to South Africa[1], I don't know that this is a great argument against them. South Africa definitely paid for that infection-based immunity in human lives.
Of course heavy and complete lockdowns are effective (at delaying the spread of the virus) - if no one is in contact with anyone else there's no way for the virus to spread. A more apt comparison would be made between countries/states with slight or "normal/average" lockdown to ones without, but that's very difficult to do in practice. And then measure the financial and societal impacts (which is also difficult/impossible).
We already have a great deal of pre-existing immunity. The big question we're answering right now is whether vaccine-based immunity (which we have more of in AU, UK, and the US) is as robust as immunity from infection (main source of immunity in SA). It's still too early to say with certainty, but it's looking like the vaccines are working if you're not immunocompromised.
That also covers only previous, more virulent variants. Omicron does not seem to infect areas outside of upper respiratory so it is a tad overzealous to spread such fear over a preprint of a different variant. It would be like comparing a mild flu strain to H1N1 original.
One might want to pay attention if the boat had a leak...
I do apologize if you took that as fear mongering, I have a nephew in a similar situation as you and we are keeping an eye on him just in case anything does come up, not that we expect anything will.
Lots of things to be aware of when boating. The best is of course to use a structurally sound vessel. Then your main concern will simply be to keep a lookout as to not hit other boaters. With a leaky old brittle boat you need to make sure to have various backups plans and means of repairs for when things go wrong. The better shape your boat though, the less you have to worry outside of basic precautions. But if your boat is old and frail it would be of prudence to get the Pfizer Hull-Restoration kit and apply it thoroughly before heading out. And remember to apply twice per year!
There was some initial fear that anosmia might be related to brain damage (since basically ruled out I believe).
One of the common long covid symptoms is "brain fog" though. Which I _think_ is probably metabolic or circulatory or something, but definitely affects the brain whatever the actual cause is.
It's not a high percentage of cases. But there are significant number of people reporting long-term issues with brain fog post-covid. Whether that's actually caused by a brain issue I don't know. But it certainly seems to be able to effect your ability to think.
Eventually it’s going to do what all other viruses have done. Mutate into another flu or common cold. We already have l seasonal coronavirus outbreaks. We call it cold and flu season; except it’s numerous coronaviruses and influenza viruses and one or two “win” that year.
Some part mutation, some part immunization so that future infections are milder. In the absence of perfect vaccination this involves killing millions of people. Let’s not forget about this.
I hope your wife is ok. Unfortunately, infection with Omicron is inevitable and not preventable, without living in a bubble. It's too infectious, and the vaccine, unlike with previous variants, does basically nothing to stop transmission. Combine that with an R0 equivalent to measles, and avoiding infection was never possible. She probably took every precaution she could reasonably take, and still got infected. That was my experience as well.
Statistically, people who are healthy and vaxxed developing severe symptoms from Omicron are outliers. That is no comfort to you, and I can assure you I know how you feel on that front when people like me tell you the stats. My mother-in-law suffered a very rare (statistically) adverse event from her second Pfizer shot in May, which killed her. She was in her early 60s, and healthy, but suffered cardiac arrest 3 hours after her second shot, in the midst of a fever. It was an exceedingly rare event, but it was no comfort to us to be told that.
I'm sorry about your wife, hope she gets through it fine.
It's mainly that you provided a personal anecdote in one direction and I found it prudent to provide one in the other direction - one that echoes everything we've seen so far, cases skyrocketing, hospitalization rates barely nudging.
Motivated anecdotes aren't prudent or useful. We know from the 2ish years of this we've had so far that the dynamics are tricky to pick apart. For example when young low-risk people are out at bars (very high exposure) and older or higher risk people stay home what happens is the hospitalizations lag because it takes some time for the first group to get sick, infect the second, and then some of those people to go on to the hospital. On the other hand older people are much more vaccinated so the relative risk between the groups will likely be different from previous waves.
That aside, hospitalizations are going up faster than they have at any point prior so not sure where your "barely nudging" comes from.
But this means, that we can reopen everything, let young people "live", and target the efforts towards old people (and other risk groups).
Atleast here in slovenia, most of the mandates affect mostly the young and healthy... yes, theoretically neither 20yo bobby nor his grandpa can enter nightclubs, due to them being closed, but with such data, we could reopen nightclubs, let bobby party and do all the stupid stuff we were free to do at 20yo, and focus the effort at grandpa, so he gets vaccinated, gets the masks, has somone bring him food, so he doesnt have to go to the stores, subsidize a plan for a smartphone to encourage more videoconferencing instead of live visits, give out free tests at home, to detect the infection early, etc.
You're describing a sanity of focused protection which should've been in place since day one, but for some reason policymakers instead lost their minds. :| At least now with Omicron they will slowly realize that lockdowns make no sense. Right? Right? (looking at Finland and crying, my home country recently having gone into full lockdown mode for no good reason other than case numbers)
Whew, I'm similar and it tanked me for about a week. I could feel every joint in my body and breathing was a conscientious decision for a few days due to the pain/discomfort. It has subsided a bit (and my family wasn't hit as hard) but I have 0 interest in experiencing it again. Currently hoping it doesn't impact me long term since I like to stay active.
You know what, I was unintentionally fear mongering. I'm glad you and others pointed that out. I did not make the connection between you having Omicron and the lack of Omicron in the paper (my nephew caught Delta...so that's where my concern lied). I hope you are still ok. :)
I encourage everyone eligible to protect themselves by getting vaccinated, but the current thinking is that new variants are most likely to evolve in immunocompromised patients who experience prolonged infections. The vaccines aren't very effective for them.
You realize that in the United States, the so called “freedumb idiots” are not the bulk of the unvaccinated right? And you also must realize that Omicron did not start among a population of “freedumb idiots” right?
Leave the straw man out of this, disease is not a reflection of character.
You say "over and over" but Omicron is the first variant that actually evades immunity (both natural and vaccine-induced) in a meaningful way. What we don't know is the level of immunity that an Omicron infection will provide. It could actually confer immunity to both itself and previous variants, which would effectively end the pandemic.
Actually prior infection by previous variants appear to still provide a significant level of cellular immunity against Omicron. There will always be some rare outliers who have a rough time but most reinfection cases will experience milder symptoms because their immune systems are already primed to respond.
If something's a one a million event, happening billions of times per day, it'll happen pretty much constantly.
This one, omicron, seems to mostly infect nasal passages and upper respiratory tract. The next, maybe after spending 2 years spreading across all the weasels of upper winchester county, may affect the lungs again.
Yeah, sure. Who knows what viruses could be spreading and mutating amongst those weasels. It's not like SARS-CoV-2 is the first, and it won't be the last. But when you say
> This is a lottery that's less fun to play
How exactly do you propose not playing? Lockdowns, social distancing, masking, etc. for life? We're eventually going to have to start treating Covid the same as we've always treated "the flu" and it definitely appears that once Omicron has run through the population, we'll have reached the time to do that.
> Lockdowns, social distancing, masking, etc. for life?
Very few places did lockdowns at any point so I wouldn’t expect that to start now, butthe ones which did were successful in breaking spread. It doesn’t need to be continuous, but it’s clearly effective for preventing huge spikes.
Similarly, we’d save lives and billions of dollars if we established the same social norms which some Asian countries have about wearing masks when you’re symptomatic. It doesn’t need anything like 100% compliance or time to be useful – we appear to have lost an entire strain of influenza this way.
The best thing to happen is people staying home when symptomatic. Wearing a mask while knowingly symptomatic is unhelpful to others, so I disagree with your belief of the alleged benefit of alleged Asian culture.
There are a number of things going on in the world that fall into the "really bad" category of both thing and trend of thing.
There's space in between bland acceptance and incapacitating terror. At the very least have an honest, clear eyed view of where the risk bars are going, and it isn't in a good direction.
> Lockdowns, social distancing, masking, etc. for life?
If you can't handle these things as a part of your life you're really not going to like what climate change brings to the relatively near future.
But you don't have to worry about arguing in forums, you've already won. Nobody respects lockdown, and never really did, even at the highest rate of infections I see people wearing masks beneath their noses, crammed next to people in airports. After omicron I can't imagine anyone caring at all even if we double our current death count.
Covid is here, it will stick around forever, it will probably be notably worse than the flu for years to come. But in a few more years that will seem like a quaint thing to worry about.
I think everyone in this thread is applying a binary model of immunity - either you are immune or you aren't, either a variant escapes or it doesn't.
But immunity is analogue. A strong, specific, antibody response can prevent infection. A T-cell response can stop infection turning into severe illness and death. Variants can evade antibodies somewhat easily, but find it much harder to evade T-cells. Antibody levels wane in weeks or months (although memory B-cells remain), T-cells remain active for years or decades.
If you had COVID last winter, then there would be a good chance of you getting it again this winter, even if it was the exact same strain. But you'd be much less likely to die of it.
So when does the pandemic "end"? What is a "pandemic"? If tens of percent of the population are catching every winter, but few are dying, is that still a pandemic?
In general, vaccines do lower transmission, by decreasing the viral load and duration of infection. Of course when you are dealing with a mutation that the vaccine has low effectiveness against, that is all out the window.
The vaccine also reduces the symptoms of the virus and so a carrier of the virus may seem well but actually transfer the virus to someone else as they are less likely to quarantine if they are not tested or showing symptoms.
The vaccine also gives one a sense of protection from infection and so they are more likely to attend mass gatherings. where the virus can be transferred.
Lowered symptoms on droplets would be better, but a lot of in-person workplaces have a "do you have a fever?" check before they issue you any sick leave.
Not having a fever and looking like a mild cold in winter would cause at least my cousin's employer to ask her to come in and wear a mask at work (manufacturing, so she wears a P100 respirator anyway).
Obviously it's way too early to have hard data on this matter.
But the WHO has been warning about this for months.
> We cannot say this clearly enough: even if you are vaccinated, continue to take precautions to prevent becoming infected yourself, and to infecting someone else who could die.
> In many countries and communities, we are concerned about a false sense of security that vaccines have ended the pandemic, and that people who are vaccinated do not need to take any other precautions.
Exactly, and that comment is why mask usage in public is still important. The two-pronged approach of masking and vaccination was always going to be our best way out of this, and nothing about Omicron fundamentally changes that.
Try not to get sick. If you do get sick, don't spread it. If you do spread it, try to spread less of it. Defense in depth.
Are the unvaccinated catching it over and over again? That seems to me a vanishingly rare occurrence, admittedly within a rapidly shrinking set of people. It would be interesting to get some figures for this, hopefully without being lynched for asking the question.
There were many stats, showing most of people with omicron being vaccinated (above the vaccination rate). I never found the methodology behind it, because if they only tested travellers to eg. africa for omicron, then sure, probably all of them were vaccinated, if they did randomized testings, they you'd expect at worst (vaccines don't work) the same percentage un/vaccinated as in the general population, or at best, vastly more unvaccinated infected.
> hopefully without being lynched for asking the question
Somehow this is a sad reality of social media and the current 'situation'... asking anything is seen as "provocative", and there are many things happening that would require more rigid questioning and better answers.
Another small sample size for you:
I know one family that's not vaccinated - both children are too young either way. Both parents and older child have caught it twice, about a year apart. Youngest is still nursing, and has not caught it. Dad and son are fine, but the Mom has an "annoying lingering cough" as she put it. But both times it wasn't worse than the flu for any of them, so in their case they see it as "we got lucky" but no one has any underlying conditions that would have caused complications.
> This is the first evidence to show us that the rate of reinfection with Omicron is high—3 times higher than Delta. In other words, infection-induced immunity is not doing a great job at stopping Omicron.
Can you give us some indication of how severe your symptoms are? Mostly we're hearing that if you've been vaccinated and/or you've had covid in the past that omicron is relatively mild.
Muscle aches, chest pain, headache, and severe coughing fits that won't let her sleep and scare me when I hear them from the other room. After being awake for two days and one of them dropping her blood oxygen to 87 I made her go to the emergency room where they gave her prescription cough medicine that finally let her sleep.
Omicron is less dangerous than Delta. It's still dangerous.
Sorry to hear about your troubles. Everyone is shouting in the media (including here) Omicron is upper tract instead of lower so I had hoped you wouldn't get oxygen drops that low or lung related chest pains. Maybe I misunderstood what these things mean although some renowned newspapers here explained it like that.
Wait 87 SpO2?! I'm pretty sure that's the point at which you would be on a ventilator? Not sure what sleep has to do with SpO2 and it seems criminally negligent for the emergency room to just send your wife off with just a cough medicine..
> You're missing the fact you can catch it over and over. My wife is currently battling Omicron after we both had covid at the start of last year. Fully vaccinated and boosted three weeks ago, caught it anyway. With an infected population this massive mutations happen fast enough to cause a new wave before the old one burns out.
I think at this point, the likely endgame is endemic virus with tolerable consequences. Humanity probably isn't capable of the level of cooperation required to drive this virus to extinction (I'm guessing that would take a massive, coordinated, well-complied with vaccination campaign undertaken over just a couple months).
As far as I know previous immunity still protects against serious disease, even with the variants, so hopefully we'll see less deaths and hospital admissions.
Correct. I know several people who are vaccinated yet caught Covid twice. The principle thing to keep in mind,
- vaccination is a risk reducer on severity of infection. Nobody said immunity; nobody said prevention.
- and on that point not getting into the hospital is important. From a management standpoint, we've got to insure demand for hospital resources does not dwarf those same resources. That's the key management function here.
> "I would say 50% would have to get vaccinated before you start to see an impact," Fauci said. "But I would say 75 to 85% would have to get vaccinated if you want to have that blanket of herd immunity."
Talking about herd immunity is definitely saying immunity, and doesn't make sense unless the vaccine prevented transmission.
Then, May 2021:
> Masks off? Fauci confirms ‘extremely low’ risk of transmission, infection for vaccinated
Almost all Covid related predictions have been incorrect, and the ones that seem correct, are only so at the surface level and require mental gymnastics. The pathology of the disease simply isn't well understood at this point, and the new mutations make it a moving target. I don't personally like Fauci, but he is a victim of being conscripted as the Chief Covid Prognosticator by the media. It's a fundamental misunderstanding of science to believe a person can give guarantees on an emerging pathogen like that.
It's amazing how we can rewrite history so fast. The number of times I see on Twitter people from different countries saying the same things, first it was "nobody ever said this vaccine will be 90% efficient against getting covid", then "nobody ever said the vaccine reduce transmission", and now it's "the vaccines have always be only to reduce ICU stays".
It's more like people are realizing what the original claims from Nov 2020 were instead of blindly trusting politicians. Pfizer and Moderna only checked for symptomatic covid in those trials and never made claims about infection/transmission. That was all assumptions people were making over 2021.
back in early 2021 I remember the media, especially the "MSM," warning that the vaccines weren't guaranteed to prevent transmission, and commentators arguing that the media were scaremongering and we should be secure in feeling the vaccines do prevent all infection and transmission. E.g.
https://www.nytimes.com/2021/02/23/opinion/covid-vaccines-tr... "Many scientists are reluctant to say with certainty that the vaccines prevent transmission of the virus from one person to another. [. . .] There should be more data within the next couple of months. Until then, precautionary measures like masking and distancing in the presence of unvaccinated people will remain important."
FWIW, it seems like those commentators who were actually right until Delta emerged. Looking at graph of Covid cases in the USA for example we were on track to low case levels until July, then the Delta variant began to break through in vaccinated individuals and the epidemic grew in size again.
> Looking at graph of Covid cases in the USA for example we were on track to low case levels until July
Gotta compare 2021 to the the curves from 2020 though: It's the same shape with different magnitude. Looks more like that drop in the spring and early summer was because it's seasonal than anything else, which we misattributed to the vaccines.
To be fair, nowhere in the US (that I'm aware of) is close to the % population vaccinated numbers necessary for a semblance herd immunity. According to the CDC, only 62% of the US is fully vaccinated, with only 35% of those also having had a booster.
Different variants mean different efficacy for vaccines, particularly regarding infection. The existing vaccines could very well have led to "signs of herd immunity" had the variants not taken hold.
It also should be said that just because you are symptomatic or tested positive, don’t go to the damned hospital unless you really need to go. You are just wasting medical resources.
Here's a thought experiment. Compare the reddit "the button" with Covid staying with us. Even with only 1 person at a time trying to hit the button it stayed alive for 3 months. And that's with people trying to keep it alive, 24x7 - just enough people to keep it going. Enough people being interested in getting a low time and staying with it.
With covid, it's just automatic, but you just need 1 foolish move between 2 people, and there's no server making sure only one person gets it at a time, it's totally a distributed network. And the timeout, instead of being 60 seconds, it's 2 maybe 3 weeks (perhaps a lot longer - we don't REALLY know).
The thought experiment here is that if we TRY to keep something alive that's actually kinda hard to and it lasts 3 months, how is covid EVER going to end?
The epidemic ends when the unusually high threat of serious illness or death ends, though, right?
If we get to the point where people aren't dying of covid at a significantly higher rate as any of the other "usual suspects", does that not mean it's over? It looks like between the vaccinated and just about everybody else that is about to or already has gotten covid, we're must may arrive at the point where covid is a just another thing on the list of seasons ailments.
Do you know what was the test that distinguished omicron from delta? Asking because my local county health department seems lacking in that technology.
I will say beforehand that I'm heavily pro-vaccination and reducing risks regarding covid.
Do we know at this point what are the hospitalization rates of omicron compared to the flu?
p.s. I hope your wife gets better soon.
Numbers are still changing but the current stat is one percent hospitalization rate for Omicron. This year's flu has a hospitalization rate almost twice as high as last year's, at 1.4 in 100,000 or 0.0014%.
> For the week ending Dec. 18, 1,265 lab-confirmed flu patients were hospitalized, up from the week prior. The cumulative hospitalization rate was 1.4 per 100,000 population as of Dec. 18, nearly double the overall cumulative hospitalization rate reported during the 2020-21 season. 3
I think you're comparing hospitalization rate per population vs. hospitalization per infected persons. If we look at the recent data and do some estimation, that's about 50k new hospitalzed for 3M new omicron cases, which is 0.016 or 10 times the flu; this sounds more reasonable.
Covid has a death rate hundreds of times higher than a cold. Colds don't make healthy women in their twenties stay up all night coughing so hard their oxygen dips into the 80s. Colds don't cause lung, heart, and cognitive damage that is potentially cumulative.
If covid brain fog compounds over time there will be some serious damn consequences.
Actually my wife had a bad cold this summer and she coughed so hard during the night that we had to take her to the ER and she was lacking oxygen (not sure by how much). She is otherwise healthy in her early 30s, though she was pregnant, which might have made it worse. It surprised me, I always thought that colds were harmless.
Yeah, they're really not. I was a paramedic about 10 years ago. Every winter I'd see colds or influenza kill people. (Or at least, initiate convalescence and subsequent rapid death from related issues within a few weeks.) Always though, those were people who were either very old or had COPD (a lung disease). It's a common way that people go out actually. A cold leads to weakness/stress leads to pneuomonia/UTI's/sepsis and then death.
An unvaccinated man with underlying health conditions died in Texas mid December after testing positive for the COVID-19 omicron variant, officials in Houston said, marking what is believed to be the first death linked to the strain in the U.S.
Your article perfectly illustrates my point. It says Omicron is 3/4 of the cases and that this one person MIGHT have died from it, but it's unclear and may be due to his other health conditions.
Let's just assume it was Omicron that killed this guy. All signs point to Omicron being less deadly than the common cold.
We can't know that because it hasn't been around long enough. But as far as taking a bayesian prior, I'd start by assuming yes except in rare cases and correct your model as evidence comes in.
I'd guess that because, for the most part, that's how the previous variants behaved. Relatively robust immunity, with subsequent infections generally being rare and more mild. Since Omicron has a lot of mutations on the spike protein which is the primary antibody target, it has greater immune escape potential because the antibodies don't fit as well.
> ... preliminary evidence WHO based their recommendation on earlier this week: People who have previously had COVID-19 could become reinfected more easily with Omicron.
But even after mutations, the next time you catch it, symptoms will likely be a lot less severe than the first. At that point, we can stop tracking it and write it off as a variant of the common cold.
I have Omicron. Already caught the virus in February 2021, good old OG Alpha Covid, which resulted in mild symptoms and loss of sense of smell for 7 months.
My only symptom is a mild runny nose, nothing else. I WISH I had colds this mild. We have a new virus that is endemic in humanity. We can choose to accept it, protect the vulnerable like we do with flu, and get on with our lives. Or we can continue to allow the news media to enervate us with non-stop panic, and choose existing over living, while fucking over kids to protect older adults.
My father is a rabid viewer of MSNBC, lacks mathematical or critical thinking skills, and doesn't read much. The result is he has been in a constant panic since the virus hit, and has isolated himself from family in a manner that has been detrimental to his health. This despite being vaxxed, boosted, and recovered from a mild post vax delta breakthrough infection. He still thinks the virus can kill him, and cancelled Christmas Eve plans for 5 of us to go to his house. The media has polluted his brain with irrational fear. His shitty physician (where I grew up is a dirt poor rural county, and the MDs there are the dumbest i've ever met) told him that "there is no natural immunity to COVID, it doesn't exist." Utter nonsense. As if my immune system (I wasn't eligible for the vaccine in Feb 21) fought, then cleared the virus from my body with some mysterious, unidentifiable mechanism that is completely unrelated to how it clears other viruses.... just unbelievable.
The virus was deadly because it was novel. It ceases to be novel when your immune system acquires memory T-cells, even if you no longer have active antibodies present. If you are old enough, or have a deteriorated immune system, the lag of producing new antibodies can be very problematic with the other strains of COVID, which is why boosters are so crucial for high-risk groups.
The data is now this:
People in their 70s who are VACCINATED have a lower death rate from Omicron than they do from flu. (If they aren't vaxxed, this is obviously not the case.)
See the New York Times, which is a very hawkish paper on COVID, for that specific stat:
FWIW, David Leonhart is one of the only journalists at the NYT who seems to be remotely literate in data and statistics writing about COVID. That newsroom is essentially filled with people who haven't studied math since high school, despite their degrees from Columbia/Yale/Harvard journalism schools. And boy does it show.
Yes, welcome to the endemic. Covid is here to stay, it doesn't matter if 100% of the world were vaccinated tommrow, covid would not go away. It doesn't matter if you get the vaccination or not, in your life time you WILL get covid (just like the flu, no one escapes it, you typically get the flu about every decade or so regardless of shots).
We need to just accept this and move back to "old normal".
I think that may be a completely rational perspective from within the United States... however, from the perspective of countries with effective containment strategies, that sounds prematurely defeatist, and also ignores the vast good that comes from containing spread for mutagenic purposes.
What effective containment strategies? Pretty much every country's strategies have completely collapsed due to Omicron.
Australia currently has a wildly exponential growth of cases and twice the number of daily cases/capita compared to Sweden, to take two countries at each end of the "containment" spectrum. And that's despite Australia being in the middle of summer, despite Australia being isolated in the middle of the Pacific Ocean, and despite Australia having more restrictions than Sweden right now.
It's all hubris. We have way less control over the spread than we like to think.
I think NZ and especially China are the only ones left. I think NZ has relaxed its restrictions about 2-3 months ago and to be honest I'm a little surprised they haven't yet followed Australia's path with the exponential number of Omicron cases, but imo the very big question remains China, I have no idea how they plan to handle this going forward.
I don't trust a single number or report coming out of China. The official numbers show a couple of thousand dead. No way.
Dictatorships usually make examples of individuals/groups/regions to make everyone else fall in line. The virus however doesn't give a shit about the wishes of authoritarian regimes, which is why making an example of a region or a city and forcing millions of people to stay indoors, doesn't stop the spread elsewhere. It's a virus, not a rebellion.
I'm assuming China has always had a low level spread that could be hidden, because their demographics make it a non-issue. However, I'm guessing Omicron is creating such massive spread that regional officials can't deny reality any longer, and the lockdowns are some kind of desperate last-ditch attempt to save face.
There have been independent studies showing their numbers are, while not perfectly accurate, within the margin of error for extrapolated excess mortality[0].
As I've said in other threads on this issue, it is very difficult to hide deaths on even a small scale. Bodies do not simply disappear, and even small numbers of deaths are easily discoverable by measuring economic output (and even air quality!) of the region.
China is being at least reletively honest in their reporting, and I think thats difficult for us westerners to believe because their numbers are so shockingly low. An effective containment strategy _is_ possible, and the west has utterly failed in that respect.
I'm not suggesting China has been hiding bodies, but with a demographic where diabetes and obesity is almost non-existant, the mortality of covid-19 is very low. You shouldn't see any excess mortality, which means you can hide the true number of cases by lying about cause of death instead.
Your argument is incredibly dishonest and myopic, because you're suggesting that every single one of those deaths were avoidable, and that any containment strategy wouldn't cause any deaths or carry any costs either.
Suicides among kids and teenagers are up 20%, I'm sure those kids would disagree with you.
Deaths of despair, i.e. alcohol and drug-related deaths are up considerably. Do their deaths count?
Deaths among dementia patients and similar are up, because of the isolation. It's very important grandma doesn't die of covid, but apparently no-one cares if grandma dies of loneliness.
Cancer screenings, heart screenings, stroke care, all of that is on the backburner, which will cost hundreds of thousands of lives in the future.
School disruptions affect all kids, but lower-income kids are overwhelmingly affected by it, and them lagging behind translates directly into shorter lifespans for that group.
We understand that every policy needs a cost-benefit analysis, but somehow, for corona, we completely abandoned that line of thought and went on some hysterical bandwagon where absolutely no strategy is deemed to costly.
Every single comprehensive QALY analysis of lockdown policies show that their cost is horrendous compared to the benefits. We're happily, gleefully, sacrificing our young for the benefit of our elders, and yet if you point this out, you're somehow the callous, unfeeling, murderer. It's insane.
China has obviously succeeded in defeating COVID, and done so with none of these secondary deaths you're describing (look at excess mortality). All of these "secondary" deaths did not occur in countries that implemented effective containment strategies, why do you think that is?
The western strategy has resulted in these "secondary" deaths you're describing, as a result of people like yourself being unwilling to accept the effective containment is possible and worth the cost.
Yeah, NZ is going to get Omicron at some point and then we'll catch up with the rest of the world. We had <20 cases the other day, but there are hundreds in quarantine who've arrived from other countries that will bring in Omicron. 2020 and 2021 was mostly totally covid free, so having normal life back again was a real blessing. But it's just a matter of time before we catch up to the rest of the world
> Australia having more restrictions than Sweden right now.
Do you have a source for that? Most Australian states have little to no restrictions at the moment bar mask mandates indoors.
If I googled correctly, Sweden only allows seated customers in bars, restaurants and events as well as limits to events?
Most Australian states still have mandatory qr-code checkins for everything, police are still chasing people fleeing the "voluntary" quarantine at Howard Springs, and still fining people not wearing face masks. And some still have restrictions that are stricter than what Sweden currently has:
> the vast good that comes from containing spread for mutagenic purposes.
We're never getting a T-cell escape mutant that dramatically increases the risk of hospitalization/death in the vaccinated/recovered.
There's really very little to worry about variants if your vaxxed and boosted.
Experts still don't have any idea how intrinsically virulent Omicron is, and it may be every bit as intrinsically virulent as Delta was (there's lots of issues with the TMPRSS2 studies in mice, while the dominant effect is that Omicron is an escape mutant and is reinfecting and infecting the vaccinated).
The lower hospitalization rate of the Omicron wave can be explained entirely by human immunity. The properties of the virus are likely much less important than the headlines indicate, which suggests the the slow process of the human race building up immunity is going to grind on and future waves will be less and less effectively virulent (although it seems like human emotions are really attracted to the idea that the virus is changing to become less virulent and that seems to be driving emotional acceptance that the pandemic is winding down).
> wave can be explained entirely by human immunity.
It's also the fact that, to put it bluntly, many of the people who were the most susceptible to be sent into ICU or to die because of Covid have already had that happen to them. Not sure if that scenario is included in the definition of "herd immunity", to be honest, just wanted to point that (cynical) truth out.
Yeah and at some point the remaining people who haven't formed any kind of natural immunity many just be "hard to infect". Their ACE2 receptors might be different, or their innate+intrinsic defenses shred the virus very effectively before infection really gets going. They just aren't accommodating hosts for the virus due to some trick of their own biology/genetics. Selection effects work both ways.
It will be very interesting to see how containment countries adapt to the future, where global eradication simply isn't possible. Perhaps there will be a sterilizing vaccine that makes it worth it in the end.
My heart goes out to those impacted by containment strategies. I was talking with someone from NZ or AU (I forget), who hasn't been able to go home an see his wife in two Christmases.
I, too, think that Omicron is the beginning of the transition back to "normal" with Covid becoming endemic. Everyone is going to be exposed to Omicron if they haven't already.
I expect that for the next year or two, boosters will be recommended as a yearly "flu shot" to give you a decent chance of being minimally affected if exposed. Omicron will continue to be the dominate strain, finding hosts in both the vaccinated and unvaccinated. The difference will be that we will have a myriad tools at our disposal to prevent serious illness and treat it when it does happen.
Most of those viruses are actually very deadly, and most of those vaccines actually make you not-get-it-at-all.
The only comparable virus is the flu, and the vaccine is equally shitty [0] as the covid vaccines are.
Death rates for young and (currently healthy) people are very very low (lower than traffic deaths in my country, much lower than suicides), and they are the most affected by the lockdowns. By reopening and focusing on risk groups we could finally start living normally again.
Yes, but that’s because you’ve only started listening to people talk about the number of dead folks recently. 800k isn't nothing but it’s not exactly earth shattering.
Not ones that mutate this efficiently. Flu is the only example and we typically only manage to get high percentages of the vulnerable with it. This is what we want with these types of virus otherwise you risk Mariks scenario. (See the poultry industry issues)
Our daughter had a fever for four days over the holidays. We literally could not even get into see a pediatrician or an urgent care. There was nothing available.
If a minor cold is enough to cripple our healthcare system, you have to wonder if maybe there is some other reason our hospitals aren't able(or willing) to go back to normal.
I spend thousands of dollars on health INSURANCE every year. If I go to the ER it still costs me over $2k. The last time I went to the ER, I didn't even see a doctor ONCE.
It's crippling our healthcare system because it's not a minor cold. People are filling our ICUs rooms needing ventilators and intravenous fluids just to not die. The common cold does not do that. They could not see your daughter about a fever because all hands were too busy keeping people from the literal brink of death.
This is why anti-vaxxers and covid-deniers are such a big problem. They think that even if they are wrong, it only affects them, but it doesn't. If I get in a car accident tomorrow, there is a very real possibility that my own treatment will be delayed because the nearest hospital is overwhelmed with dying COVID patients.
We have had over two years to prepare for this. I don’t buy it for one second.
The last time I went to the ER was prior to the pandemic… and it still cost over two thousand dollars after insurance. Insurance that I spent probably over 10k a year for.
Maybe Covid isn’t the issue. Maybe our infrastructure is.
If you think they aren’t laughing their arses to the bank over this then I dunno bud.
You really think that we can’t afford the equipment and staff to handle this? How much do you spend on health insurance every year? Your brother? Sister? Literally everyone around you? Why aren’t we pointing fingers at the hundreds of wasteful medical contractors hemorrhaging taxpayer dollars in this time of crisis? How much money do you think director level types and administrator level types deserve in times of catastrophe such as these, especially if my daughter can’t even see a doctor when she is sick?
Omicron is not the problem. We should be able to handle this.
Can't say that 'it is the end' yet - but given that pandemics end when there is no more 'room' for the virus to move through naive hosts (places to infect). The fact that Omicron is SO contagious means it will effectively find any pockets of 'fuel' in the adult human population in the coming weeks and months. Everyone will be exposed.
It is probably more accurate to say it is the likely start of the transition between 'pandemic' and 'endemic' phase. We say endemic as it LOOKS like the gap between coronavirus immunity length to viral instability (number of changes) is longer than for influenza. (T-cell response still very strong, original SARS patients almost 2 decades later have cross immunity to SARS-Cov-2, Omicron immunity effective against delta, etc) That said - it is VERY unlikely to be eradicable at this point due to its ability to infect so many different species and circulate and breed in the wild (more so than even influenza).
So new variants down the line in the coming years/decades is more likely (not different than swine flu, bird flu, etc pandemic risks in the recent past). But, if longer term immunity holds up - none of these will have anywhere near the impact given the absence of billions of naive hosts to burn through.
So if we call the transition from pandemic to endemic the end (likely, yes) - then probably.
It's been over ever since the vaccines became widely available. After vaccination many of us went back to normal and haven't looked back. Huge bureaucracies just take a long time to change course and some simply refuse to recognize that it's endemic for whatever reasons.
> A pandemic is an epidemic of an infectious disease that has spread across a large region, for instance multiple continents or worldwide, affecting a substantial number of individuals.
> An epidemic is the rapid spread of disease to a large number of people in a given population within a short period of time
In no way has "rapid spread of infection disease across multiple continents" ended. The past few weeks should make that a bit more clear. Being vaccinated reduces the negative effects of infection, and may also reduce infectiousness and spread, but it didn't end the pandemic.
But does it matter? If omicron becomes the "new flu" (or "the new cold") for the young and healthy, and with vaccines even for old and weak, do we have to call it a "pandemic" anymore?
I mean... did we have a "cold pandemic" or a "flu pandemic" before 2020? I'm pretty sure most of the planet had a cold every winter, and we just lived with it. Same with the flu... risk-groups died, and noone bothered the young with it, we just called it "normal life".
> In epidemiology, an infection is said to be endemic in a population when that infection is constantly maintained at a baseline level in a geographic area without external inputs.
> A widespread endemic disease with a stable number of infected individuals is not a pandemic.
The cold and flu are "stable" albeit seasonal. While we might expect that outcome for variations of the SARS-CoV-2 virus, we're not there yet. A rapidly exploding number of infections is not a stable number of infected individuals.
At any rate, some people getting vaccinated and choosing to live as if the infections do not exist does not "end the pandemic."
it’s nice to believe, but a lot of our ability to return to normal requires these bureaucracies to be on board. it doesn’t matter that you individually are comfortable sending your kid to school, that school’s not going to be open if the consensus and bureaucracies are against you.
somehow we failed to coordinate the back-to-normal in my region when the vaccines arrived. this seems like the next best opportunity to admit that we’re ready to lift restrictions, so here’s hoping we can keep the majority on board this time.
Keep in mind, that between the "like the flu" and "mild" designator, folks are dismissing the severity of Omicron. But we must keep in mind that "mild" is in reference to "severe" which entails death and ground glass lungs.
The pandemic has taught me how little people care about words;
"Asymptomatic" now means "just a low grade fever", or "a cough that didn't take me to the hospital"
"Allergies" now means "I can barely breathe no matter what environment and I'm tired like I'm taking Claritin, just ignore the color of my sputum or my cough."
"It's just the cold or flu" now means "I'm just sick for a week, and I should definitely socialize like normal"
Medical community Covid "mild" is a far cry from common cold "mild".
I had a "mild" Covid Original Flavour. I "only" had a 103 fever for 3 weeks, swellings in places I didn't know could swell, and had my stamina shot to shit. It's been just over a year and I'm just now beginning to feel like I can start bringing myself back to pre-Covid healthiness levels.
And all that is "mild". I didn't lose my sense of smell. I didn't lose oxygenation. I never had to go to the emergency room.
There's no reason to believe that we'll achieve herd immunity to anything beyond Omicron. There's a reason Flu vaccines are a thing you get every year, even if you've had the flu.
There will be no real herd immunity effect to protect those who lack immunity. Instead virtually everyone is just going to get infected, and most survivors will retain cellular immunity which gives them significant protection against severe symptoms during later reinfections.
Herd immunity has been predicted since about May 2020 (in Sweden) and there is always far too optimism about it. We now know that a recovered infection does not produce permanent immunity.
And Omicron is an order of magnitude less virulent on hospitalization/deaths per infection basis.
The pandemic is never going to be "over" on a case basis, and the virus is never going away, spread will never be zero, variants will always keep happening for decades.
Omicron is telling you that its going to be time soon to start thinking about this virus more like a normal cold/flu virus based on its impact.
It's hard to imagine a more transmissible covid variant for a layman such as myself. I wonder if microbiologists are able to model the maximum theoretical transmission Sars covid is capable of.
I don't think we can model it accurately, but we can look to other viruses as examples. The SARS-CoV-2 Omicron variant is still only about half as contagious as measles.
Omicron is infecting fully vaccinated people and those with previous infection. In the early cases detected in SA, many had already had COVID and/or Delta.
It would be amazing if an Omicron infection produced antibodies that fought off COVID & Delta, as that could rapidly bring relief to the pandemic, but I haven’t seen that suggested anywhere yet.
If it’s largely immune to the vaccine and doesn’t produce antibodies against COVID/Delta, we might as well label it a new disease instead of a variant.
Luckily it seems to be incredibly mild. I wonder if we had such robust data on the common cold of it would look similar to Omicron.
> It would be amazing if an Omicron infection produced antibodies that fought off COVID & Delta, as that could rapidly bring relief to the pandemic, but I haven’t seen that suggested anywhere yet.
There has been a study that suggests Omicron infection provides protection against previous variants. This correlates with data from the UK that suggests Omicron is displacing Delta.
You're thinking about it all wrong. Omicron and Delta are the same virus, and there's not particularly any good data that Omicron is less intrinsically virulent than Delta.
Omicron infects those who are unboosted, and likely reinfects a lot of the population that is >6 months recovered from prior single infection.
It is all about the fact that Omicron infects people who already have T-cells and aren't immunologically naive. The way out of the pandemic is our memory B-cells and T-cells.
> It is all about the fact that Omicron infects people who already have T-cells and aren't immunologically naive. The way out of the pandemic is our memory B-cells and T-cells.
What does immunologically naive mean? And how do B-cells and T-cells help us get out of the pandemic?
immunologically naive means that your body has no prior exposure to a virus (or its variants). basically it means it has NFC how to deal with it. so it basically has to brute force its way to a defense against the strain.
This is why you saw people with early covid cases having their immune system go haywire and a lot of the treatments for covid focused on dampening the immune system to prevent it from killing the patient.
once you've seen a virus and its variants a few times your body has 'remembers' strategies on how to fight the virus. and launches those strategies against it. sometimes depending on the mutations those strategies are less effective (omicron) and your body has to create new strategies.
B-cells and T-cells are how the body store and deploy these strategies.
Your body has intrinsic, innate and humoral defense mechanisms, along with circulating neutralizing antibodies.
Intrinsic and innate defenses are early and quick and children and young people have strong defenses there and they can shred viruses quickly (and sometimes so fast that people don't form any humoral memory to the infection). If you ever get a '24 hour flu' where you feel like you have a degree of fever and then it passes that may have been an aborted infection that was destroyed by your innate and/or intrinsic systems.
Neutralizing antibodies are what most people think of as "immunity" which is immunity against infection. Small amounts of neutralizing antibodies will bind to foreign particles that are circulating and hinder them from being able to bind to cellular receptors and cause infection to begin with. This is true sterilizing immunity, and if its good enough it is a perfect shield. The neutralizing antibodies though bind to specific sites on the proteins of the virus (about 20 for the spike protein of SARS-CoV-2) and mutations at those sites can cause escape mutation variants (like Omicron). Neutralizing antibodies also tend to wane (probably because of autoimmune diseases that they could otherwise cause).
Once an infection has taken hold then you have intracellular virus and proteins. Those are chopped up by proteases inside the cell (in general proteins are often chopped up by the cell this goes on continuously) and those short protein segments are bound to a receptor called MHC-II which is then transported up to the cell surface and displayed on the surface of the cell. This is how cells signal what kinds of proteins they are "seeing" inside of them. There's a complicated system to distinguish between self-protein segments and foreign segments which I won't go into. Once the segments of the viral protein are displayed on the surface of the cell on MHC receptors that is a signal to other immune cells that there's something going wrong and the cell is either lysed and destroyed or dragged off to lymph nodes (by dendritic cells, which have nothing to do with nerve dendrites, but they looked kind of similar so got named that a long time ago).
Once in the lymph nodes the learning process happens and undifferentiated B-cell and T-cells are trained on the peptide and that leads to T-cells that can recognize the proteins. The fact that it is small slices of the protein and not the whole thing mean that there's actually many more segments that T-cells get trained on. There's a couple thousand T-cell epitopes in the virus, and they're overlapping and in many cases they're overlapping in conserved regions of the proteins where the virus likely cannot ever mutate without ceasing to be a virus. So T-cell antigenic escape will be impossible.
This process takes a lot of time though, and doesn't happen right away. There's also the process of hypermutation and affinity maturation which means that the whole humoral system looks a lot more like a bayesian spamfilter than a lock-and-key model. This is why giving a booster 6+ months after an initial shot(s) is effective at producing immune responses against variants that have mutations in the protein that the immune system is being trained on. You give the immune system "Viagra" as a string and it learns to identify "V14gr4" as well more or less.
Now the next time you get hit with the actual virus, even if its a variant, it may not be affected by neutralizing antibodies due to antigenic escape or waning immunity, but if you've got T-cells then they'll see those peptides being displayed by infected cells. Many or most of the peptides will be recognized as being exactly the same as the prior infection. Those T-cells will then either send out cries for help (CD4+ helper cells) and rally the troops, or else they'll directly lyse and destroy the infected cells (CD8+ cytotoxic lympocytes).
Because you've seen the virus before those T-cells have a huge headstart now and even though you don't have "immunity" in the sense that you've been infected, the severity is lower, because your body can identify the infected cells and immediately deal with them.
And one example of how we know that T-cells don't really wane and have considerable cross reactivity in the face of mutated proteins is the 2009 H1N1 pandemic. People that were born before 1957 were exposed to the H1 protein of the H1N1 strains that were circulating in humans from 1918 to 1957. That virus spent ~50 years mutating in pigs before hopping back into the human race, but the H1 protein in the 2009 H1N1 pandemic still was recognized by cross reactive T-cells in old people born before 1957 and that took the whole edge off of that pandemic. Everyone born before 1957 was effectively vaccinated (and probably boosted many many times against the 2009 pandemic). The H1 protein would have extremely mutated after 50 years of serial passage through probably billions of pigs, but conserved regions in the protein meant that the "spamfilter" was still trained on enough of it to give it a high score.
And that's the quick overview, there's a lot more.
The gov and media are never going to straight up tell us the pandemic is over. We have to take our way of life back and let big bro silently move on to something else.
As far as I can tell, there ends up being no practical difference between "the pandemic is over" and "this virus will be in circulation forever". People use one phrase or the other to emphasize different concerns.
I think people don't think of "the pandemic" as a state of having virus around us, but as a bigger political picture of lockdowns, mandates, vaccine passports, travel limits, mandatory testing, masks and all that.
If omicron means we'll all get it in the next few months, and (for the 99.x% survivors) that means that covid is "just another cold/flu", we can stop with the "pandemic" (political), and live as we did before 2020. Old people will need vaccines and boosters and all that (as they did for the flu before 2020), and young people can finally live a normal life again.
People have been talking about how hospitalization numbers are lagged since before Thanksgiving. It's been almost two months. It's time to stop hoping for doom and gloom and accept that it's over.
> People have been talking about how hospitalization numbers are lagged since before Thanksgiving
People have been saying that since 2020, but if you're talking about the current variant, omicron wasn't even given the omicron designation until the day after Thanksgiving.
> Everybody can make their own decisions, as long as hospitals are good.
Wait. "Everyone can make their own decisions"? And those decisions are completely rational, not affected at all by what the media is saying? I would argue the complete opposite.
Why are you trying to bend the argument into hospital capacity? Is your argument that if hospital capacity is under threat then it's ok for the media and government to lie and instill baseless fear into people, solely as a means of a) scaring them into staying at home (to minimize the spread of the virus) and b) to demonize unvaccinated people?
One would think that transparency and honesty would work better than bullshitting people.
Yeah and nobody mentions that our hospitals were already stretched to their limit before Covid because they are for-profit corporations. They should have had capacity for a pandemic because everyone knew there would be one. It’s poor planning, not Covid. They will add capacity and then what will your argument be?
you can't add capacity to a system that requires highly trained specialists on a dime. hospital capacity is very much limited by how much it is used on a day to day basis, regardless of pandemic status.
what you suggest simply will never be an effective strategy.
It's a combination of doctors and nurses. In some places, it's nursing staff that's keeping all beds from being open. This is absolutely a workforce that can be flexed on a shorter term notice.
Doctors can also be incentivized to do rotations in the ER. My primary care physician many years ago used to do ER rotations as a sort of overtime. Inventivize with the right pay, more will do it. Granted this isn't a large labor supply, but it certainly could help.
Instead, what you see is a shrinking of the nurse labor supply by a few percentage points due to vaccination requirements. Pretty ridiculous to complain about lack of capacity when you force some of that because you refuse to officially recognize natural immunity as equal to vaccine derived immunity.
nurses take years of training. where are you going to get them during a global pandemic on immediate notice when literally every area needs additional nursing resources?
nurses and doctors are leaving due to the stress of a long term pandemic. are you asserting we can just force them back into labor? that's fairly dictatorial of you. it still doesn't change that we would only revert to original levels, it would not be a significant increase in supply.
Huh didn’t say anything about forcing, please be careful about putting words in peoples mouths. I said incentivized with pay, quite the opposite of forcing.
its the natural outcome to your argument. there simply is no way to increase the supply of highly trained specialists within even a year timeframe.
'incentives' won't help. there simply isn't enough supply in aggregate. and they are not leaving because of a lack of pay they're leaving due to the stress of dealing with assholes on the daily. cash isn't going to fix that problem.
the only option left in such a scenario is literally mandating they return to work. which doesn't nothing be return you to initial workforce levels it doesn't increase capacity.
we're seeing this right now with the national guard 'mobilization' in some areas. they're literally doing nothing but sitting with patients and other menial tasks that don't require training. they're basically just in the way.
that which is asserted without evidence is rejected without evidence. you under estimate little people give a shit about money after a certain point.
plenty of people in the 100-200k range take cuts in the 30-40k / year range to move to better work environments. so the idea you'll get doctors who generally make 200k+ would be willing to work in shitty conditions for a prolonged period is pretty bogus.
nurses you might be able to entice them to come back for 20-30k bumps, but its also unlikely.
even if your idea worked, it doesn't increase the supply. it just brings us back to predecline levels.
edit: in fact a clear example of your idea not working: paying people to get the vaccine. did jack shit to actual increase uptake.
Everyone should be able to make their own decisions anyway. Hospitals are some arbitrator of decision making and hosptial admission due to covid is collapsing. Stop fear mongering this isn’t Facebook.
Depends on if politicians believe they can lift restrictions without negatively reflecting their career or not. There's a lot of Twitter mobs out there promoting "extreme caution" that will tank your political career if you aren't catering enough to their caution-comfort-level.
I don’t know. Anecdotal but I know a lot of people who had prior strains (many even vaccinated) who have gotten it. The numbers are so high that natural immunity from previous strains/vaccines seems to be very low.
If delta or OG Covid didn’t do much about omicron, I don’t think we can assume omicron will do much about some future variant.
The pandemic will truly end when therapeutics are mature. My liberal relatives become visibly upset when just the concept of therapeutics is brought up. Thanks liberal dogma/media…
I read article from Israel. It wrote: "severe covid cases are low, but flu season just started". Pandemic will finish at spring, and hopefully will not start next winter.
Of course it'll start again the next winter... as will the cold season and flu season.
The only question here is, will there be lockdowns, mandates, masks and vaccine passports, or will we finally give up, focus on the risk groups, and let the young and healthy live their normal lives.
What you're missing is that we're eventually (arguably right now) going to be referring to colds and other weak mutations of COVID as "COVID" still, and by virtue of still calling it COVID and still having these COVID dashboards, it's never ending. There is no end, it is a new normal for millions. Too many people's brains short circuited, too many people got anchored to March 2020.
It means that among recent PCR test confirmed cases, 100% of patients were infected with the Omicron variant rather than Delta or some older variant. The number of asymptomatic carriers is unknown and probably large, but can't possibly be anywhere near 100% of the populace.
Omicron evades the "natural immunity" that people were getting a hard on for. That explains a lot (not all) of the massive fitness it has - it can infect people that previously had Covid infections again.
Immunity is a spectrum, not a binary condition. Infection by previous variants appears to still provide a significant level of durable cellular immunity against Omicron.
I assume you are referring to the "There is no federal solution to covid" quote. But it was in the context of talking to state governors and Biden saying a federal plan wasn't being forced on them -- that the primary work is done at the state level and the federal level is there to support it.
I can't speak for him, and obviously tweets are short enough they can't contain it either. But apparently the plan was (a) to use federal funds and manpower to get vaccines spread as widely as possible. There was an early goals of 100M doses in the first 100 days, which was met, and another goal was set and met [1]. Another factor was sending the message: this isn't a "Democrat hoax", that it is real, is killing people, the vaccines are safe and certainly much safer than getting covid. I say that has been accomplished.
On the other hand, there is a large contingent of people and talking heads who have tried their hardest to spread fear and misinformation. We are still at something like 60% inoculated, and many doses of the vaccine ended up going bad or were shipped overseas because not enough people trust the vaccine.
Third, there is no way to prevent novel variants from causing new problems, other than getting the old variants under control to reduce the vast pool of variant breeders.
[EDIT] Also, your terse "he claimed there was a federal solution" is also subject to debate. He said he had a plan, but that doesn't mean the plan was a federal-only solution.
So what you're saying is that Biden's plan was essentially the same as Trump's plan, which also focused on using federal funds and manpower to produce and distribute vaccines as widely and rapidly as possible.
I don't want to turn this into a political debate, but I'll respond to you question. Trump repeatedly downplayed the severity of the virus, called it a "Democrat hoax", argued against many of the masking and distancing mandates that large cities had put in place, claimed that Fauci is incompetent and shouldn't be listened to, etc.
So, no, they are not the same plan. There is a reason why counties that went red have lower vaccination rates and more severe covid-related problems.
Donald Trump never called the virus a "Democrat hoax". There's plenty of room to criticize his handling of the pandemic (much of it was totally incompetent) but at least get your facts right instead of lying.
> But apparently the plan was (a) to use federal funds and manpower to get vaccines spread as widely as possible. There was an early goals of 100M doses in the first 100 days, which was met
Trump's Operation Warp Speed got the vaccines out with federal funding, and deployment under the Trump administration had reached 1.6 million per day before he was out of office - higher than Biden's original goal. That was why they had to increase the goal afterwards.
You might make some valid points, but it's really hard to see them when you don't cite sources, and when you deliberately use inflammatory language like "cronies" - and that's against the spirit of HN anyway.
I’m no fan of Biden but let’s be clear that this transcends administrations. Trump put Fauci on TV every day, Trump granted billions to big pharma. Just like Biden takes the fall for dumb wars started by Bush and Obama, he’ll take the fall for Trumps dumb fight against COVID.
The problem is that we have institutions like the Fed and the CDC and WHO that have been proven completely incompetent when power is deferred to them. They panicked and now we pay the price.
>the Fed and the CDC and WHO that have been proven completely incompetent when power is deferred to them.
I'm curious what criteria you used to make that assessment? Also, I don't know what you mean by "power" being deferred to them. What extra power was given?
It's not the end if governments keep playing covid theater games.
In Europe they definitely will with increased surveillance and digital IDs that have proven to do nothing to stop covid (as initially portrayed), but that won't stop govs from pushing them onwards and dehumanising any group who doesn't want to comply with their coercive measures.
It's an interesting time for people who really value freedom and human rights.
It’s just politicians trying to save face at this point. Trillions of dollars lost and total debasement of western currencies was all to arrive at the natural solution to a virus that was destined to become endemic from the very start: let it play out.
Two administrations, one from both parties. Same fed chair. Same people at the CDC and WHO. It’s not partisan. It’s institutional failure.
I'm not sure what you mean. Vaccine was a success, it saved millions of lives. What's becoming endemic is a less deadly variant, otherwise we would be back to square 0, confinement and developing a new vaccine. So, instead of calling it a failure I would call it success with a lucky ending, if everything continues like this of course.
It's not a lucky ending as much as it is the inevitable ending. Virus evolution tends toward becoming more contagious and less deadly. We've known this for a long time, and we have no reason to believe that this virus would be any different.
If viruses tended toward becoming more deadly as they became closer to being endemic, humanity (or any animal) would not have lasted very long.
Just giving my 2 cents. Got boosted 3 weeks ago. Now I have covid. Everything is fine, feels like the least ill i ever was from anything. But I wanted to state that omnicron is a beast. I did wear a ffp2 mask with nearly every social contact and if we didnt wear mask we would test ourself. I am sure I got it from the streets from people passing by. That said I am in the french alps and it was vacation time here.
And until now it was rare to know someone who has covid …. Now it feels like people who dont have it are getting rare
I hope so much this is the entrypoint for an endemic situation
I'll give my two cents then. People are probably not gonna like it here but I think alternative perspective is important.
I got vaccinated in June 2021 and haven't been following any restrictions or rules for the last ~10mo. No masks (unless forced or asked), haven't limited human contact, haven't stopped seeing Grandma, etc. I have traveled extensively in the past four months, including to two foreign countries. I nominally live in the epicenter of the new outbreak in NYC which accounts for the lion's share of cases as of this writing (unless something drastically changed in the past day).
I have not gotten COVID-19. [0] If I did, it was a very mild case that gave no symptoms.
I was in contact with people who had COVID-19 on Christmas and New Year's Eve (both tested positive after the fact, they did not know prior). I got tested December 23rd for a flight, results were negative. I got tested yesterday, results were negative. I feel great though I had a bad cold on the ~27th which I think was from traveling and not COVID specific given I tested negative twice.
[0]: I had a very bad, vaguely defined flu back in January 2020 that knocked me out for a week that may have been an early COVID-19 case. But everybody says this and then their antibody tests show up negative. I haven't gotten antibody tests to confirm and given that I'm vaccinated it's likely they'd show up positive for that anyway.
> People are probably not gonna like it here but I think alternative perspective is important.
Thanks, I hate it. :-)
Anecdata is the worst*, as generally only self-identified outliers feel compelled to share. So then there’s more outlying noise than there should be, and normals get confused.
Still useful in the sense of serving to illustrate probability curves mean tails exist, so a bunch of people must be outliers, oh look here’s one.
But where it goes wrong is when someone looks at 1000 viewpoints on whatever, identifies the 2 who think it’s aliens, and creates a “both sides” narrative. Or self-identifies: hey y’all, I’m a walking survivor bias!
For policy, “alternative perspective” of an outlier is worth exactly 2 cents, but must be stacked up against the 80 cents of the bell curve. In other words, yes, the case must exist, but is not illustrative of what a normal distribution participant can expect or how they should behave.
* Anecdata is also the best. Edge cases matter for bounding problem spaces, contingency or mitigation planning, or maybe even important for novel discovery. For instance, while it shouldn’t determine majority behavior, why one individual might seem immune to COVID could be very worth a quick check to see if worth looking into. If it’s not tail luck, if it’s immunity, that could reveal an undiscovered mechanism helpful to the normal distribution.
Similar story - boosted mid Nov. Travelled over Christmas. Have been wearing K95 masks as properly as I can as often as I can when out in public. No real symptoms to speak of, but took a PCR just to be sure. Bing! Positive.
Not sure from where I got it, but the contagiousness of Omicron is impressive.
> The beast part was more for how contagious it is.
A beast compared to what? Common colds in previous years? Previous influenza strains?
> As a malady it is fine with me but I am still having an eye on long covid…hoping for the best.
You got 3 shots, wear a mask (it sounds like outside), lord knows what else. And you’re still worried about long term side effects from a cold? Can you quantify your risk of serious side effects from this illness?
????? Long covid and post covid syndrom are a known thing. The vaccines dont reduce the risk of those two as good as the the other factors …. And wtf a cold… dude stop trolling its covid.
And fucking wearing mask doesnt have anything to do with long covid…
Are you straight out of telegram or what ???
> ????? Long covid and post covid syndrom are a known thing.
Okay let’s see your evidence of long term side effects and syndromes caused by Omicron. The variant was discovered Dec 20. Whatever you’re claiming is based on previous variants which are not in circulation.
> The vaccines dont reduce the risk of those two as good as the the other factors ….
Okay, how much do the shots reduce your risk of “long COVID”? Looking for quantifiable results from research, not your opinion.
> And wtf a cold… dude stop trolling its covid.
Uh literally quoting “the science”:
> Well over 200 virus strains are implicated in causing the common cold, with rhinoviruses, coronaviruses, adenoviruses and enteroviruses being the most common.[
> And fucking wearing mask doesnt have anything to do with long covid…
Not my point, if you read more carefully. Can you quantify your risk of long term complications from a mild infection? How’s that compare to risk of car accident, sports injuries, cancer?
> Are you straight out of telegram or what ???
Is this supposed to be some kind of ad hominem attack? Yawn. I can’t pretend to care about your opinion of me. If you’re going to respond please focus on answering my questions.
> Okay, how much do the shots reduce your risk of “long COVID”? Looking for quantifiable results from research, not your opinion
Use google… its not my job to do it for you
> Not my point, if you read more carefully. Can you quantify your risk of long term complications from a mild infection? How’s that compare to risk of car accident, sports injuries, cancer?
I read carefully and it was your point. And again usw google . Not my job
> Is this supposed to be some kind of ad hominem attack? Yawn. I can’t pretend to care about your opinion of me. If you’re going to respond please focus on answering my questions.
Yes it is. People like you aint indivuals. You are all the same bunch with exact the same opinion and the same way of misunderstanding things. Dude you are totaly transparent
> Well over 200 virus strains are implicated in causing the common cold, with rhinoviruses, coronaviruses, adenoviruses and enteroviruses being the most common.[
> People like you aint indivuals. You are all the same bunch with exact the same opinion and the same way of misunderstanding things. Dude you are totaly transparent
What's transparent is that nothing you've said is based on facts or rationality, it's just regurgitated hysterical opinion. And since you've been nothing but a childish and frankly rude idiot I'm not going to engage with you any further. Hope your little cold gets better soon.
Dude first learn reading. How do you get from „ i have an eye on long covid … wishing for the best“ to „ i am fucking stating everything you seem to interprete into my one sentence“
And omnicron was detected november
If you are reading between the lines… congrats there is blank space.
Btw aint you afraid that some cold could mix with hiv and go viral via telegram and sudenly you have covidaids?
And a cold aint covid … covid is the malady geniuos. Different strais of viruses. Are you for real ? I talked with many of you and can never figure out if you rly cant understand( apparantly you can read and write ..congrats first step to be a human) or if you are just trolling ?
At this point that is the best case. COVID zero is a pipe dream, there are just too many vaccine refusers and too many people refusing to do anything to avoid spreading the virus. If COVID follows the typical evolutionary pattern of viruses and becomes less dangerous, we can get back to normal life -- the question is how long that will take.
I'm not sure what basis you have for assuming it will evolve to be less dangerous, Since it still leaves most of its host alive I can't think of a mechanism that would prevent it from staying equally deadly, except of course that most of the population will have some degree of immunity.
This pandemic will inevitably end, after which Covid-19 may stay endemic, but Covid-19 becoming endemic and the pandemic ending aren't really the same thing and frankly aren't really causally related so to me it seems weird to express hope for the endemic to begin rather than the pandemic to end.
Anyway, we'll need to ride out this last wave first. I'd say hopefully last, but we may end up hoping it wasn't. Regardless let's hope it at least burns itself out in the process as opposed to smouldering for ever.
It is still more dangerous than the other endemic coronaviruses that cause the common cold. In general the selection pressure on viruses (and other parasites) is to be less disruptive to the lives of their hosts -- not just being less deadly, but also not incapacitating hosts for extended periods of time. How long it takes for a virus to become endemic-without-ill-effects can vary widely, but the hope here is that COVID19 will do so quickly, becoming "just another common cold" within another year or two.
Honestly I hope that one day it is gone for good but until then an endemic situation would be somehow better than a pandemic one.
I didnt say that clearly and hoping for a, also, bad situation is not the best thing to whish for but after 2 years of pandemic I am whishing for something less bad….
As I understand it, wearing two masks was only recommended for those wearing surgical or cloth. If your wear an N95 or equivalent you only need the one.
omicron has solidly taken over Vancouver BC. Anecdotal evidence: in the past two years (except this past week) I have only known 1 person who got covid. In the past week I know over 20 people who have got covid.
I sincerely hope that this is the beginning of the end of covid lockdowns. omicron is taking the world by storm and I wouldn't be surprised if the entire world gets it in the next few weeks.
It seems to give partial protection to Delta like 50% reduction in infections.
Different aspects of immunity seem to last different times. Antibodies fade over six months or so but T Cell immunity can last decades in general. Though obviously Omicron hasn't been around that long to check on.
> to what extent does recovering from Omicron prevent Delta?'
If Omicron is reaching 100% prevalence in so many locations, I wonder if Delta will not be as much of a threat anymore? It seems like there haven't been any infections with older variants for a long time now.
Omicron evolved from Beta, which had pretty much bottomed out in the human population. They believe it evolved in mice. Just because Delta is disappearing in the human population doesn't mean it's gone.
Last night on NPR there was a scientist cautioning people who think this means the end because it'll burn itself out.
His point was that nobody predicted delta, and nobody predicted omicron. There's no telling how serious the next variant will be (and arguably there's much greater chance of a variant given how many people are getting infected.)
+1, I work in a small, fully remote company, and up until the past 2 weeks, I know of only one colleague who had been infected. 5 people were out last week because of COVID. 5 people who live in different states.
Anecdotally from the people I know who've got covid since omicron was identified, none have had to go to hospital (all are double vaccinated, some had booster), but it can still be a rough few days/week while ill and some are still coughing/feeling overly tired a few weeks later
Also in Vancouver and similar numbers. I know at least 10 people who currently have COVID, including myself and my partner.
It's not mild for all. Two people in particular have been brutally sick for over a week. One spent three days in a self-described "fever dream".
I actually don't know whether I have it, since I'm asymptomatic and can't get a test. But the four other people at my dinner party all got symptoms and two tested positive.
13 people in my immediate circle got it in the last 7 days. A few had 2 days of fever, a few a slight cough, a few sore throats. Everybody is fine now.
I still know no one in Germany who ever had covid, only one person in the US and one in South Africa (who also died from it), so I’m not sure about that.
Yes, it’s called a filter bubble. Covid was extremely easy to avoid pre-Omicron even without vaccines if you don’t go to nightclubs and don’t work in an office and have no kids.
Even during the lockdown, a family friend of mine needed to go to a hospital for an unrelated issue, and that's when a nurse from there passed COVID19 to him. Then he passed COVID19 to his father. He was 35, no kids, didn't work in an office. Still got COVID19 and spread it with deadly results. Etc. etc.
Church, Weddings, Thanksgiving / Christmas / New Years, Birthday parties and other social events? Choir practice? Indoor sports like basketball or racketball? Gyms? Restaurants?
--------
There's a lot of social interactions between people when you start counting them up.
Hospitals can be unavoidable if you're unlucky and get hurt. Grocery stores, too, but you can minimize your trips. But the other ones? Totally voluntary and avoidable. The public health guidance around COVID has been atrocious, even as scientists learn more about how the disease spreads indoors. We're going to probably need to change our "indoor event" focused culture if we want to have any hope of getting this behind us, but it's unlikely to happen because it's inconvenient to people and there's seemingly no way to enforce a mandate. And heaven forbid people temporarily inconvenience themselves to stop a deadly pandemic!
There's no need to change our indoor event focused culture. Now that we have vaccines and other improved therapies we can just accept the risk and move on. In fact, outside the HN bubble people in some states already did that months ago.
> In fact, outside the HN bubble people in some states already did that months ago.
The issue, and this remains true today, is that hospital space is filling up fast (and did fill up in those states months ago).
A discussion must take place about balancing our individual social needs with the needs of our public health system. There was a train-derailment in Montana in 2021, and COVID19 filled up their hospitals so much that the injured needed to be driven 2+ hours away to look for hospital space / treatment.
Is that the kind of community you want to be a part of? Where your nearby doctors and nurses are not accepting any of the injured train passengers due to the overwhelming COVID19 case numbers?
-----------
We definitely need to do our part as individuals to minimize the damage we cause to our hospital systems.
------
There's something to be said that "Yes, this tradeoff is worthwhile but only for the end-of-year parties". Vs overwhelming your hospital space just to "own the libs" when no major parties / social events are even happening in the middle of August.
The thing is you can't stop it. So that leaves the question, should we stop all social gatherings for the foreseeable future and lock ourselves in our homes?
Certainly. But why is it inconvenient to people? We don't really discuss personal issues in the public space, so I'm forced to use my own examples.
My grandma is in her late 80s and soon will be 90. She's had brain cancer decades ago, recovered, but maybe that's finally catching up to her. Our family pretty much murmurs about it behind her back, but her sharp mind simply isn't as sharp as it used to be. Every year is a diminishing of her memory, her ability to focus, her ability to hold discussions and interact with us.
To the point where she's pretty much locked herself inside her own house (we're worried about her but she refuses to live with any of her children) in most situations.
So what does this have to do with parties? Well, parties are one of the only ways we can manage to draw her out of her house and interact with us.
---------
I can't imagine that I'm the only one who is dealing with the diminishing mental abilities of an elderly grandparent (or parent). But my grandma's extreme stubbornness and pride makes this entire exercise more difficult.
Now sure, maybe we do have to worry about COVID19 killing her. But on the other hand, her lack of socialization and isolationism is another issue that our family struggles to find a balance with. That certainly can't be healthy either, and arguably the social part takes priority at this point.
Furthermore: COVID19 has vaccines and booster-vaccines to mitigate that particular disease. But we don't really have a "Treatment" for the social isolation she's put herself into, or general aging issues as her mental state deteriorates over the near future.
Frankly, this is probably signs that she's on her last legs. Its something we will have to come to terms with as a family, but hosting parties where she can still see us (even in this state, before she gets worse) is a priority.
---------
Yes. Its "inconvenient" to cut out the yearly parties out of our life. And I'm sure other people have similar stories about why _THIS_ Thanksgiving / Christmas was like no other, and why it was very important to meet up again.
----------
Don't get me wrong. I'm largely pro-lockdown, and pro-mask, pro-vaccine. But you cannot underestimate the importance of social interactions or family, especially since we all are in different circumstances. Sickness and health changes the calculus in many ways.
I didn't share this story last year, because I felt like the lockdowns were a needed step (pre-vaccine). But this year, I'm speaking towards opening up again and relying upon the vaccine to keep us safe. Perhaps its two-faced for me to take different stances just one year apart, but things really have changed and pushed my calculus towards the other way. After losing Thanksgiving/Christmas 2020, people are aching to see family again. And 2021 has vaccines, dexamethasone, monoclonal antibodies and the Pfizer pill. We've cut the death rate by 80%+ on treatment alone and vaccines can cut it by 90%+.
The specific cases of people experiencing dementia has not only been noted during the covid-19 era, but also evidence shows that dementia patients have experienced a huge number of excess deaths. I'm personally sure my grandfather was one; he'd had it for years, and it pretty much sat at a steady state for years, while family was interacting with him enough to periodically jumpstart his mind back into lucidity. The decline after lockdown was precipitous.
That disease doesn't somehow make in-person interactions with family and friends unavoidable, though, when people don't have the disease. The fact that people with dementia requiring stimulation to stave off decline are also members of families doesn't magically make all interactions with family members medically necessary.
I generally agree with your conclusions about the change in circumstances, but I personally limit in-person social activities to a small circle of people who are also limiting in-person social activities precisely because I want to continue visiting my grandmother without killing her.
There's no reason at all in your comment on reasons to make your parties indoor, instead of outdoor like the GP said. It's like you are replying to a different comment.
Would you have a late 80s great-grandmother outside in the cold? Its 30F right now and I'm not even in a cold part of the country. I got some buddies out in the mid-west that are in 0F weather and -20F wind chill.
Realistically speaking, the party is going to be at a house of one of her children, or grand-children.
-------
An "outdoor" party these days is a closed tent anyway with heaters. Its practically an indoor party with the same air-flow issues except much much more expensive. Do you think I haven't looked into this?
This is a very disingenious take, don't you think?
I am also German with an average social circle as I would say. Until the end of last year, I just knew of one case of Covid among all of them. Since then, a few families got it - most of them via kindergarten.
Say what you want about our Covid response but from my point of view we made it fairly well through the pandemic so far.
I also live in Germany, and similar experience. I rarely know people who have been infected with Covid, and none with Omicron. Omicron is also a bit delayed in Germany (which is good).
I live here and know many ;) But in the north, we generally made it through it better (recent club openings with mass infections notwithstanding, I do not know people who go to mega-clubs during a pandemic).
If I compare it with Belgium it's cases are better but deaths is relatively worse to the other stat, which is kinda weird. Unless they don't test much.
But Belgium also overcounts deaths ( should be /2 when I checked in 2020), which means any untested death is counted as COVID. Most people don't seem to be aware of that.
The CDC publishes a weekly chart showing the proportions of circulating variants for the US as a whole. The Delta variant had previously driven most other variants near extinction, and now Omicron is doing the same to Delta.
i wonder what countries like China and New Zealand who are taking a zero COVID approach are going to do. COVID is endemic in the rest of the world except for those places where it doesn't exist at all? I don't see that working.
Omicron isn't significantly more contagious than Delta for the unvaccinated, however. It's just that the vaccinated can spread omicron, so anyone who wasn't vaccinated and managed to dodge infection for this long is now in nightmare-level difficulty when it comes to remaining uninfected.
There's a preprint for a study of 12,000 households in Denmark that seems to offer evidence to the contrary[1]. Take my earlier claim with a grain of salt, I'm not an epidemiologist, but this is what an epidemiologist told me.
> Surprisingly, we observed no significant difference between the SAR of Omicron versus Delta among unvaccinated individuals (Table 3). This indicates that the increased transmissibility of the Omicron VOC primarily can be ascribed to immune evasion rather than an inherent increase in the basic transmissibility. If this observation can be confirmed by independent studies, it has important ramifications for the understanding of the current challenges for control of the epidemic
There are multiple components to the immune system. For some viruses like measles, prior infection or vaccination usually triggers production of sterilizing antibodies which block subsequent infections in most patients. That isn't really the case for COVID-19. However the immune system also contains memory cells which can ramp up defenses more quickly during reinfections. The targets for those defenses are mostly the same across all SARS-CoV-2 variants.
I have oversimplified this explanation to keep the comment short. If you'd like to really understand what's going on I recommend this panel discussion by a group of leading physicians; it's long but worth a listen.
That's a potentially misleading visualization. Delta can be steady rolling even if its share falls from 100% to 5%, as it apparently has, if the denominator has increased by the same factor.
There are 15k covid RNA in every ml of sewage coming out of boston right now. Figure 200l a day of sewage per person and that is a lot of covid. I would hold off on eating oysters for a bit.
Most people are relying on arbitrary testing to figure out how many people are infected. I think this totally under reporting number of infections because the whole population is not tested on a regular basis. To get an accurate picture of people are infected, you have to look at whole populations.
One whole population group to study to get a better understanding of how bad this wave is is to look at the cruise line industry. Everyone has to get tested, and thus you are studying a whole population. According to a recent CDC report [1], between Nov 30 - Dec 14 of 2021, 162 cases were reported on cruise ships. Then the next two weeks 5013 cases were reported. This is roughly a 30x increase!
If you look at the NY Times infections chart[2], in the same time period, their 7 day average only went up like 3x. This is grossly under reporting of infections.
The sewage chart looks at a whole population and it is easy to see the increase in infection is more in the 30x scale than it is the 3x scale.
Be safe out there everybody. If you look at whole population groups, Covid is way more infectious than what a lot of news media outlets and their data would tell you.
This sewage report is about a whole population and it is clear to see infections many more times higher than what a lot of news agencies are reporting.
I’d be surprised if coronavirus can infect non-mammals. I don’t think there’s been any scientific evidence of this. For the reports of contaminated fish and what not, it’s suspected the contamination happened on the supply chain (e.g. someone at a fish packing plant coughed on food.)
Early in the pandemic researchers swabbed lots of surfaces and while they were able to amplify COVID DNA from a bunch of the swabs, they were not able to successfully culture a single sample from any surface, which included the hospital room of a patient on a respirator where the virus would have been beyond abundant.
Some harvesters will hold oysters in sterile water for a few days to clean them out (Depuration). This usually works but it is hard to know for sure if the one on your plate got this treatment or not.
You should not be eating that oyster raw if you are not sure, and that only applies to norovirus which is resistant to mild disinfectants(e.g. ethanol)
why? RNA detected != active virus. e.g. in room temperature, virus can survive the maximum of 5 days (on plastic 3 days, cardboard 24h). It's an impossible vector of transmission.
Don't forget about long covid. My covid infection was mostly gone in 3 days; yet 7 days after that I'm in the ER for peripheral neuropathy. Several days later I am still here with perhaps permanent loss of function. There are a few other youngsters like me with covid complications on the neurology floor, most with less than 2 comorbidities. Oh yea, the ER was packed, 6h to triage.
Sorry to hear about your peripheral neuropathy. Check out some of the treatments for dysautonomia. There are some cutting edge treatments that have been developed over the past few years, they just haven't become mainstream knowledge or trickled down to the medical schools yet.
Essentially you have got to get the brain producing the proper amount and type of brain waves again, and then once you have that, slowly work back into exercising while trying to avoid triggers and push / crash cycles.
Everyone in my house had COVID in September and now we all have it again. Vaccinated, boosted, prior infection - none of it matters when it comes to avoiding the virus. I think we’re at the point where the virus is part of life and the best we can do is get back to living.
i don't know why the parent was modded down. It seems to me the governments are beginning to change the narrative to "the virus is part of life and the best we can do is get back to living.".
In Colorado. Anecdotal, 6 ppl I know here all have covid. 3 of them had their boosters 2 weeks before hand. 1 unvaccinated. Was like a bad cold for all of them.
also in colorado. currently have O. the + tests from our (previously very cautious) friend groups are coming in rapidly. i was boosted in mid-novemeber. _physical_ symptoms feel like a bad cold (cough, congested head, sinus headaches) though i'm afebrile. the mental symptoms are definitely different/stronger. sleeplessness. auditory hallucinations. i'd say mental fog but i can't say that's not related to the sleeplessness.
I'm now 10 days clear of the last obvious symptoms - but I've been having major trouble focusing since the end of the Holiday and not sure if due to covid or not.
I hope you'll fully recover soon! Most people hoping COVID-19 burns through the entire population are not considering the ramifications of wide-spread long-covid.
Scary thing is. Milder disease is a constant factor improvement in hospitalization. But faster spreading (higher R value) is an exponential worsening in hospitalization.
It's probably better to have a 50% hospitalization rate and an R value of 0.8 than a 5% hospitalization rate and an R value of 2. After 3 'generations' of spreading the second situation already has more hospitalizations.
The CDC has estimated the overall hospitalization rate since the start of the pandemic at about 5%. Now with vaccines and other improved outpatient therapies the hospitalization rate is dropping.
> It's probably better to have a 50% hospitalization rate and an R value of 0.8 than a 5% hospitalization rate and an R value of 2. After 3 'generations' of spreading the second situation already has more hospitalizations.
Sure, but those aren’t the only choices. Over the last 30 days the daily case average has increased by 500%. During that same time the daily average hospitalized has risen 100%.
And the test positivity rate has increased to almost 30%, which implies an almost comical undercount in actual cases.
The contagiousness and severity are diverging in an extraordinary way. We’re likely undercounting cases by 1/5 or 1/10th.
The testing positivity rate is relatively useless at this point. For example, in my State, there is no way to report a positive test from a rapid result. Only PCR tests administered by a medical professional are considered valid for statistical purposes, even though the government is giving out free rapid tests.
This is for good reason. Rapid tests are substantially less sensitive and often give false negatives, especially for asymptomatic cases. There are also a lot of rapid "at home" tests out there that have high false positive rates, so even if non-PCR tests were added to the data the only reasonable approach would be to still require them to be administered by a medical professional to make sure the test is correctly administered and that the test itself is relatively high quality.
The idea that rapid tests are less sensitive and therefore not valuable is summer-2020 thinking and outdated.
Rapid tests are perfectly fine and should be counted by health departments.
Case in point. My family of 4 all tested positive on rapid tests. 3/4 of us had symptoms. None of us received PCR tests because the next available appointments (other than a 6 hour wait at a state run testing center) were a week away.
Thats 4 people not counted. And we were part of an outbreak that included 3 other families that all tested positive via rapid tests.
I don't think it's useless. I think it's a pretty good indication that there are many multiples of actual cases for every confirmed case. If covid cases have risen 5,000% in 30 days, but hospitalizations have only risen 100%, that's an extraordinarily positive outcome.
Maybe but “exponential growth” is a conspiracy theory promoted by epidemiologists. In reality, growth follows the S-curve, so a milder, faster spreading disease will also saturate the population (flatten the S-curve) much sooner, so overall the impact will be much less.
I've seen this argument elsewhere and I don't get it. From my understanding the limitation on exponential growth, the flattening of the top part of the S-curve, comes from total population. There is no one left to infect, basically.
If the rising part of the S-curve is steep, that means people get infected within a shorter timespan and a corresponding higher load on hospital beds and healthcare personnel, which is what we are trying to avoid with the lockdowns.
What am I missing?
Also, calling exponential growth a 'conspiracy theory' seems unnecessary
A conspiracy theory lol. When they talk about exponential growth, they are talking about an R0 > 1. Yes, after some point it drops under 1 and flattens out because there are fewer and fewer people to infect.
You want to keep the number of cases in a range that the health care system still can deal with. Reaching the the flat part of an S-curve (i.e. infecting everyone as fast as possible) is NOT desirable because that leads to many cases in very short term.
Anecdotally, the hospital my partner works at has been frantically converting almost all of their floors to covid floors due to the influx of patients. But, few require ICU/ventilator.
So yes it's bad/dangerous in that hospitals may fill to overflowing and struggle to treat covid or non-covid patients, but not bad in that Omicron is directly killing more people than Delta et al.
> Professor Andrew Hayward, of University College London, earlier told Sky News that it is unlikely there will be a variant more severe than Omicron.
He said: "This one will be hard to outcompete... given how successful it is."
Professor Hayward added that for a "variant to stick", it needs to have "some advantage over the existing variant and that advantage needs to be really in terms of increased transmissibility or escape from immunity".
He said: "There's no advantage to the virus itself becoming more severe."
> He said: "There's no advantage to the virus itself becoming more severe."
I thought the virus doesn't care about becoming more or less sever since its transmission capability is all that matters to it and symptoms are hidden (thus increasing transmission between individuals) in the first days of infection and that's what evolution is driving him to be: more transmissible.
The fact symptoms appear sooner than delta seems to be a step backward for the virus in terms of efficacy and it's compensated by being way way way more virulent.
What am I getting wrong here ?
Also:
Omicron could as well have been more severe (and the jury is still out on long covid anyway). If there's another variant less virulent but compensated by hiding symptoms longer... then this would take over omicron and this variant could as well be more severe.
Is that totally out of the realm of possibilities ?
My regular joe thinking tells me that we can only be sure of the direction it's going to take when spring comes. 2021 had 5 vocs, it's only the first days of January.
Yes, I believe the high transmissibility before symptoms appear is the most beneficial trait to Omicron. However, if a variant appeared with exactly the same traits except that it was 10x more deadly, then a lot more people would be taking it more seriously, self-isolating and driving down infections. From an evolutionary perspective, there is an incentive for the virus to become milder rather than more deadly because of how the news of a deadly virus changes human behaviour.
It's not like strains of the virus are made by intelligent design. The point is that Omicron became dominant because people due to a lot of factors, its high transmissibility and people's disinterest in quarantining among them. If Omicron 2.0 came out with the same transmissibility, but a notably higher lethality, people's interest in quarantining would have increased significantly, which could have prevented Omicron becoming the dominant strain in spite of its increased transmissibility.
I remember 6 months ago some researchers also said that Delta was so contagious that it is very unlikely that even more contagious variant arises. Oh well, sometimes unlikely events happen.
Preliminary data on the Omicron variant indicates an R0 value in the 7 - 10 range. So SARS-CoV-2 might still have a little more room to evolve even higher contagiousness.
This doesn't make any sense, unless the variants directly compete against each other. But what we've seen with Omicron is that it can infect someone who just had Delta. So if there's a mutation that can infect someone that had Omicron, but is more severe that mutation can flourish, even if it is less transmissible than Omicron. It just flourishes in parallel.
So far in the UK hospitalisations are increasing, but not dramatically so. There's also brouhaha about how London (where the wave is the worst) is at its peak, or already on the way down.
[bear in mind, the hospitalisation number is not quite what it seems. It is "people in hospital who happen to have Covid", not "people who got Covid so bad they need to be hospitalised". So if you have asymptomatic Covid and a broken leg, you count for this purpose. Still, you do require the whole Covid-safe theatre, medical staff in PPE so it's also not like "meh doesn't matter"]
According to your link there's definitely a bump in hospital admissions. Only time will tell how high that bump goes. Let's play it safe and reserve judgement just a little longer...
Just wanted to check that since (at at least one London hospital) they're on different wards (as in, even discounting that obviously you don't want 'broken leg with covid' on a general 'broken bones' ward with neg/query patients) so seems odd to me they'd report data like that vs. those needing treatment for it.
My understanding is, there's a fair few people at hospital with "bad Covid" who aren't in Intensive Care. For example, if you have steroids and Remdesivir given to you, you already need to be hospitalised.
So there's at least three categories: people with really bad Covid, people with Covid bad enough they can't be at home, but not (at the time) awful, and people who don't suffer with Covid at all but could infect others, and something else is wrong with them.
I think they are all challenging to the healthcare system in different ways. Ultimately, if you project a complex situation onto R^1, it can't be too accurate.
Yeah, at the one I'm familiar with it's (as far as I know and not necessarily limited to) may-need-intensive-care; intensive-care; out-of-intensive-care; and isolation (the covid+, but only there for the broken leg example).
> Ultimately, if you project a complex situation onto R^1, it can't be too accurate.
Absolutely, and it's all too easy to make 'obvious' armchair policy..! I was just a bit surprised since my assumption would be it counted the relevant wards (if it were up to me, I think that would be the first three; only not the isolation-but-there-for-something-else).
The "peak" in London last week (if it really was the peak) had 1 in 10 people infected. Those are huge numbers, even if most people don't need hospitalisation.
More cases means usually faster ability to spread, which again usually indicates that the virus is getting milder, so to answer you first q: yes.At this point covid realistically cannot be eradicated, i would say even if you achieve 80%+ vaccination rate worldwide(which we won't).To answer your second question i doubt we'll have more hospitalizations than delta.And to also state the obvious: by the time we get a 'jab' against omicron, we'll have another variant out there, whether identified & named or not.
Its milder than Delta but way more transmissible. The more people get this, more will be the chances of a new variant which can be more deadly/transmissible.
It’s possible, but most coronaviruses do not seem to have followed this in the past, nor flu-based viruses. More deadly variants usually don’t win it from less deadly in a selection process.
However it is important as the WHO recommends to do way more to export vaccines to countries that need it. Not just developed countries to prevent the chance of new variants.
If this is all so likely and rapid, why does this not happen constantly every single year? Why did it take so long for one particular virus to leak when it seems like with so many humans we should see some super virus come up constantly.
It does happen from time to time, but it's usually not _quite_ right. In the last couple of decades, there've been at least four or five pandemic false alarms, mostly flu variants. In the event, none of them quite made it. But now that covid _has_ made it, minor variations on the already-very-dangerous-thing can be a big problem.
>Why did it take so long for one particular virus to leak
why long? The EcoAlliance's gain-of-function (with the "Human Subjects Included" checked) NIH grant for Wuhan started in 2014, the human-specific DNA modifications of the virus were described in the EcoAlliance's 2018 DARPA grant proposal, and in the end of 2019 - voila!
With regard to omicron - we may be also witnessing the continuation of the same magic of the fast "gain-of-function" by the virus :
"By inserting this particular snippet into itself, Omicron might be making itself look "more human," which would help it evade attack by the human immune system, said Venky Soundararajan of Cambridge, Massachusetts-based data analytics firm nference, who led the study posted on Thursday on the website OSF Preprints.
This could mean the virus transmits more easily, while only causing mild or asymptomatic disease."
I guess you're alluding to the "lab leak" theory. I can't say I know how serious it should be taken, but just this: If this really was a lab leak and China knows something we don't know, then I'd be really scared of their current behaviour of locking down entire agglomerations over two-digit numbers of mostly asymptomatic cases.
It's a good article, as far as I can tell - in particular as actually presents some evidence for reasonable assumptions. Though to be fair, it was known before that GoF research was conducted in the WIV (I believe) and there is not yet any evidence that the research actually resulted in this virus.
What's new to me though is how deep the involvement of US entities apparently was and how close to SARS-CoV-2 territory the whole endeavour came. So in this case, absence of evidence is definitely not evidence of absence.
Also that one of the drivers of shutting down the lab-leak theory was apparently commissioning the WIV to do GoF research! (Though I still wonder what all the other scientists supporting that editorial were doing.)
If those FOIA papers will be used for more investigations in the near future, thing should definitely become interesting.
I don't think this logic is correct. Viruses can not become infinitely transmissible/deadly; clearly there is an upper ceiling. Second, people gain immunity after infection. We'd expect the first variant that infects most people to win, effectively closing the door behind it.
But we're seeing evidence that Omicron provides some immunity from the more dangerous strains like Delta.
If we're worried about Omicron mutating to become more deadly, why aren't we worried about the other human coronaviruses doing the same? 229E, NL63, OC43, HKU1 that have been around for ages?
There's nothing magic about Omicron, its just a repsiratory virus thats relatively new to humans so there's not so much population immunity. And looks like we're rapidly getting exposed to it, so its about to lose its advantage.
I'm not sure its that different. For example NL63 binds to ACE2 just like covid. Its just less damaging.
Many viruses can attack multiple organs in the body if the infection is bad enough and the viral load is big enough to spread that far - e.g. see https://www.healthline.com/health/viremia
Hospitalizations are down 70%, yet in South Africa only 26% of the population is vaccinated, this goes to show that Omicron is less severe than the original variant.
The reason for this is Omicron replicates mainly in the upper respiratory areas and does not invade vital organs. This is also why its so contagious.
December 27th was the first day I personally knew a Canadian that had caught COVID. Today, I know of three independent outbreaks among my friends and even more at work.
The Alberta active case rate looks like a vertical line [1], and that's even after recently switching mostly to take-home test kits that don't get reported in these numbers. In my group of friends, 6/7 tested with take-home kits.
They take samples, randomly sequence some, and use those to estimate the proportion of different variants. Apparently 100% of them were omicron in the week of 12/26/2021
I've been traveling internationally over the past couple of day. Every person seems to have the sniffles, or to be coughing. I haven't noticed this since covid began, presumably because the masks, sanitizer use, and social distancing have kept the cold and flu down.
Here in the UK there seems to be some sort of cold that is ticking all the same symptom boxes as Omicron (sore throat, headache, nasal congestion, cough) but “isn’t Codiv”. My whole family had it before Christmas. I would describe it a rotten cold, we all sat on the sofa for like 5 days but weren’t bed bound, tested negative with LFTs the whole time (each did one at least every other day for a week). We isolated anyway.
We know a lot of people who have had this experience in the last month. Most people seem to have had this cold or Covid recently.
Now, I am suspicious that something is going on here. I have a suspicion that the LFTs are not testing positive for relatively mild Omicron. The LFTs procedure here, which we followed, has been to only swab the nose (they changed it maybe over the summer?) but I have seen many anecdotal reports over the last week of people who tested negative (LFT) with just a nasal swab but positive if they swabbed their throats. This potentially ties in with reports that Omicron mostly affects the throat whereas Delta affects the back of the nose. I have seen no official studies.
It would not surprise me if we find out in a few weeks/months that nasal LFTs have a very high false negative rate with Omicron.
Edit:
Just found this about a small study suggesting exactly what I am suspicious of:
> Rapid tests do work with omicron. "But why are some people staying negative in the first days they have symptoms??" This is expected. Symptoms don't = contagious virus This is literally a reflection of the fact that vaccines are doing their job!
Mina's tweets are all over the place, and mostly speculation. It's also strange that he's arguing that the vaccines are working in one breath, and then basically telling people to retest daily if possible and go into isolation the minute they think they're going to sneeze in another breath.
The cold is a minor annoyance to most people's immune system, as almost everyone has prior exposure to cold-causing viruses, but colds still manage to spread. We don't test obsessively or quarantine for "the cold."
If "Symptoms don't = contagious virus", how in the world is the virus spreading at such a blistering pace? Is Mina suggesting that literally everyone is getting this thing, including in highly vaccinated populations, by magic? Occam's razor, combined with basic knowledge about how respiratory viruses work, tells us that people who have symptoms are very likely contagious. They might also be contagious before noticeable symptoms arise, and as they subside.
As for viral loads, with Delta, research found that vaccinated individuals were capable of having viral loads as high as unvaccinated individuals[1]. Until there's data about the viral loads with Omicron, it seems dubious for Mina to suggest that the reports of rapid tests failing to pick up omicron infections are related to low viral loads.
Instead, Mina's 5th tweet is worth paying attention to:
There is a lot of chatter about how people are getting positive rapid tests when they swab their throats instead of their nasal passages. It's anecdotal at this point, but if we're going to engage in speculation, this seems a much more valid form of inquiry.
The vaccines are very effective at reducing the risk of hospitalization and death, and Omicron seems more mild to begin with. It is very effective at spreading in vaccinated populations, which isn't surprising given that the decreasing size of the SARS-CoV-2 naive population means that the virus is now under pressure to select for immune escape. It's strange to me that a "Epidemiologist, Immunologist, Physician" would tweet as if he didn't know this.
The official guidence is that LFT are only to be used if you DO NOT have symptoms. If you have symptoms you should instead be getting a PCR (lab) test.
Official guidence:
> There are different tests you can get to check if you have coronavirus (COVID-19). The test you need depends on why you're getting tested.
> The 2 main tests are:
> PCR tests – mainly for people with symptoms, they're sent to a lab to be checked
> rapid lateral flow tests – only for people who do not have symptoms, they give a quick result using a device similar to a pregnancy test
Well, the symptoms according to the NHS are fever, cough and loss of smell/taste. If you have runny nose and sore throat, you don't have coronavirus symptoms. Technically. So you take a LFT, right?
It confuses me how different the rules and "truths" are all over the world.
At least when I caught Delta I had a sore throat and a runny nose to start. That was it for a couple of days.
There was an outbreak in my children's school so the family went to get tested.
It was only after that I got a cough and fever (and positive result). It wasn't until about day five I noticed I couldn't smell.
Public health where I'm at says basically everything is a possible Coronavirus symptom. They list headache, sore throat, runny/stuffy nose, congestion, fatigue, muscle aches, nausea, vomiting and/or diarrhea, inability to smell, and pink eye.
One of my friends tested positive for covid yesterday (via PCR test). He suspected he might have covid so he had been doing LFTs in the days leading up but kept coming up negative. Out of interest he did an LFT after he got his positive PCR and, surprise surprise, negative.
Obviously this is very anecdotal and speculative, but like you said, I wonder if LFTs don't pick up this strain of the virus as well as previous, and if that is what is causing the numbers to be so high since I would imagine it is how most people test.
There's a recent study(0) that suggests that saliva tests are more reliable than nasal swabs for detection of Omicron variants, whereas the inverse was true for the Delta variant.
Same experience and suspicions here with December being miserable for the household but no positive LFTs (around 3 each) or PCR (one each). Wife still has a sore throat every night, weeks later, and mine lasted weeks too, which is unlike any cold we've had previously.
I had this and so did my friend and we live across the country. The same symptoms at different times. It was as you describe and my cough was terrible, unlike previous colds or chest infections. I coughed for about 40 hours straight and didn't sleep. I tested myself multiple times.
I found it strange that I am boosted, masked, and sanitized, plus I am isolated as I am an unpaid carer for a family member with poor health and I managed to catch the bloody cold!
It seemed suspect to me as well but of course, anecdotal.
Just stating the obvious (but not necessarily true): could be that before covid you never really never thought about others sniffles/coughing, but now after covid, everyone who behave "sick" becomes noticeable. I certainly noticed this in myself.
Went to a new years party in California and a dozen of us got stuffy noses and a small cough. Test came back negative. Haven't had a cold in so long I had almost forgotten what they were.
Before getting the results I had assumed this was the mutation everyone would get as we leave the pandemic with a natural immunity to this weak strain.
This was said in some Covid HN threads 1.5+ years ago when Covid began. We know now it was mostly people noticing stuff they didn’t notice before. Likely the same case here
Can anyone point me to a reliable source that explains in layman's terms why one cancels out the other and it's not possible to have both (say) delta and omicron at once.
Somewhat tongue in cheek, but since cancellation seems to be the case, could we not create a version that was 100x more transmissible than omicron but completely benign? Cane toads in Australia aside ;)
Exponential growth. Lets say that there is one delta infection and one omicron infection in the population. Each delta infection causes two more people to be infected, while each omicron infection causes three more people to be infected.
The growth of a single delta infection:
1 -> 2 -> 4 -> 8 -> 16 -> 32 -> 64
Versus a single omicron infection:
1 -> 3 -> 9 -> 27 -> 81 -> 243 -> 729
Omicron started out as 50% of the cases and over 6 reinfection cycles became 90% of the cases. Delta just can't keep up. These are made up numbers but that is the general idea.
I love this self-administering vaccine as it so elegantly explains the answer to the parent's question.
BUT, it is so elegant that you just provided fuel for the new conspiracy theory of how government forced us to get vaccinated by creating this crazy new variant in a lab that would essentially spread the vaccine without our permission. Just waiting for that to start bubbling up from the fringes ;)
It does persist, all else remaining the same, but since it is so much less infectious it will go extinct if and when anything makes a dent in Omicron. Dents including lockdowns, increased vaccination, changes in public behavior or eventual immunity.
> could we not create a version that was 100x more transmissible than omicron but completely benign? Cane toads in Australia aside ;)
You overestimate our abilities to make viruses that do what we want, let alone to make viruses that do what we want and won't evolve into viruses that do what we don't want after being released into the wild.
This is also basically saying "can't we make a transmissible vaccine", and as much as I like vaccine mandates, I think there would be significant ethical issues with that.
A bit of a sidebar this was basically the plot of The Last Ship. With infrastructure of the world crumbling how do you distribute immunity without the manufacturing infrastructure.
So yeah I'd put it in a 'last ditch Hail Mary to save the world' type of plan...
I feel like I recall at least one worm that somebody released that would infect servers, patch the vulnerability that it used to get in, infect other vulnerable servers, then delete itself.
I think it's because Omicron spreads more quickly and confers some immunity towards Delta. So before Delta has had a chance to infect a given person, they've probably already gotten some immunity from Omicron.
Just a no sources comment: you can get confection of the flu and covid or any variant with any other variant at the same time. It's just over time one variant out competes the others because it's more fit.
Dumb question that's been vaguely nagging at me: If a host can have both at the same time, in what sense are they competing? There are plenty of cells to infect in a particular host aren't there?
They have different transmission probabilities. Omicron has far more presence in the upper respiratory tract. It's just a numbers game, they're not competing in any active sense.
In that case I don't understand the "omicron will outcompete other variants" thing I keep reading about. If they don't interact wouldn't the progress of one variant be unaffected by the presence of another?
I think you're correct - if Omicron and Delta provided no cross-immunity, there would be no competition, and they would just continue on their own trajectories as if the other didn't exist.
I'm not an expert (so take this next part with a very large grain of salt), but I would guess that someone with an active Omicron infection (and so swarming with antibodies) would get the biggest immunity boost against Delta. So if Omicron is everywhere, Delta runs out of infectable hosts. In principle, it could even go extinct - if that were to happen, it wouldn't matter so much if Omicron-induced immunity wanes, there would be no Delta left once the shields are down.
I don't think it matters if omicron is ultimately worse or not, nobody cares anymore. I was out visiting a gym yesterday, in an area with sky rocketing cases, and no one was wearing masks. They talked multiple times about how much they cared about health, without even a hint of irony. I was initially put off, but realized that this is just the world we're in.
In two weeks we'll find out if the calculus of lower death rate x higher case count means anything, but even if it turns out to be a complete disaster with record deaths, I just don't see anyone caring.
Pandemic is done after omicron no matter what. We already largely ignore deaths from climate change (which depending on your calculations can easily be as high globally as covid), we don't even speculate on deaths from environmental pollution. Covid is just another environmental hazard that we will accept like any other.
I have a feeling we are gonna want more things to worry about. Done with the pandemic? Let’s latch on to something to make sure 1) You have no kids 2) We keep increasing the power of the government measures 3) Equality meaning we stoop to the lowest level, not bring up the baseline 4) Keep eroding the standard of living.
Even if we are a space faring civilization, these people will make it uncool to “pollute” space or would be against fusion power if we are able. I can already see progressives against SpaceX.
This is a weird observation to make. Optimism is by far the dominant ideology in our society and has been for well over 300 or so years.
Even currently when you browse mainstream media news postings the vast majority of the articles focus on how mild omicron is and how people should get to back to work.
I'll agree that the media makes plenty of money pedaling anxiety but real pessimism is nearly forbidden in everything from mainstream media to academic philosophy (seriously, Schopenhauer is basically it and he's much more of a buddhist than a true pessimist, the majority of German pessimist thinker remain untranslated in English).
Reacting to any observation of concerning data as "against optimism!" speaks more to a prevalence of hard denial than the rise of true pessimism.
I live in Berkeley and this is basically 90% of the people I meet, see and interact with. Btw they’re also almost all vegetarian and Soylent drinkers. I felt awkward having a sausage pizza yesterday with a friend. So my observations are at the very lease factual in my area, pretty sure factual across the Democratic Party. Progressivism isn’t what it used to be (Obama era).
How does this contradict optimism? They're doing these things because they believe this will lead to a brighter, better future. Just because they disagree with your path to get there doesn't mean they are pessimists.
I wasn't speaking about optimism, but just the general culture here. I am fine with vegetarianism or whatever, but making me feel awkward and imposing that on others is bothersome. "I feel like eating meat is immoral"... while I am eating a sausage pizza. I should clarify, he wasn't a proper friend, just a co-worker.
They don't want a brighter future. That's the message I am getting. In some ways that's pessimism, no?
One more anecdote - I had a someone from work come over to help me for moving furniture. He goes "Why do you want to have kids? Do you really want to bring them into this world?". It's this pervasive sense of pessimissm that emanates from this culture. I am pretty convinced.
Nobody cared ever. At my school every year everyone takes off their masks and wears them improperly all the time. At the beach and mall every year it's still constantly full of hundreds of people with less than 1 meter space in between. At restaurants they don't do anything different than normal except put a mask on while ordering. They could just make something at home instead of being lazy and spreading COVID.
The metrics presentation on the page are very misleading. The use of color is confusing (red generally means bad or getting worse, green means good or getting better). The up/down arrows are seemingly red or blue arbitrarily. Why are the four rows each colored differently? Just a bizarre UI.
If you have to present data to a user, please read a book by Edward Tufte first. His books will change your entire perspective, e.g.
Some places have been pretty close to "let it run amok", ie indifference by the population and government, widespread antivax sentiment, etc. I'm talking about places like Bulgaria, Russia, etc. They have seen around 0.75% of the population die.
Letting the original run freely would have likely cost at least 1% of the population, plus the long covid, lack of treatment for other conditions etc.
Death counts are also hard to compare because earlier variants already killed a lot of high-risk people.
Would we rather have a widespread epidemic we know less about and can control or a less deadly one we have treatments for, but have limited control over? It's hard to say. It'll be interesting to see what happens with omicron in China where they're trying their hardest to control it.
As someone else mentioned and I agree that I hope we are at the end of covid lockdown potential but is that realistic?
Is it pure luck that Omicron is more transmissible but apparently less severe than Delta? What is to stop the next variant being more transmissible than Omicron but 10 times more deadly?
I know news outlets are really bad for clickbait titles, but I read yesterday that a new variant was detected in South France in the last few days? When will the carnival end and what does it mean?
As far as I understand that's not likely because the it would be maladaptive for the virus. If there were a really deadly variant in South Africa, then 1) it wouldn't spread as fast because viruses need live hosts to spread and 2) people would change their behavior before it reached the entire world.
That is, Omicron is mild so people likely didn't change their behavior too much. If you saw a lot of people around you going to the hospital, you would likely stop going out so much. (Some people knew many people going to the hospital during the pandemic; others saw none for years. The infection was very unevenly distributed. On HN I expect most people are remote workers and know few people getting infected.)
It depends whether it confers immunity to other variants, and how long it lasts.
If it’s good at that, it is so transmissible that quickly everyone will get it (the fabled “herd immunity”) and new variants, unless they break the mould, won’t have a large enough population of o sustain themselves in.
Otherwise, maybe we’ll enter into some kind of equilibrium, where there’s enough of not-terrible Omicron to keep everyone “topped up”, equivalent to permanently high vaccination levels.
Or, none of our happens and as you say, the next variant is more transmissible and more deadly, and we’re screwed again.
Re France, new variants pop up all the time, if it’s the same one I read about, there’s no indication that it’s special right now so for now I’d say clickbait.
It's pretty much pure luck that Omicron isn't more severe than Delta, and it's not clear that it's a lot less severe though that'll be clear in the data in another month. I suspect in 20 years this thing will look more like measles in that high levels of vaccination starting in childhood + rapid response on outbreaks will make it a negligible risk at a personal level. Who knows though, anyone promising certainty is probably trying to sell you something.
I thought that a second variant was essentially an independent stochastic process.
If I have that right that suggests that, had Omicron not occurred Colorado would currently be Corona-free.
I doubt that is true though. Maybe some of the people who now have Omicron would have gotten Delta later on? I don't see how one variant can truly extinguish another variant otherwise. But I am hoping someone here knows better than me.
How do you see them as independent stochastic processes? Assuming one person can only be infected with 1 variant at a time, then they are not independent, instead they would be negatively correlated since the more people have omikron the less people can get delta. If instead one person can have more than 1 variant at a time, and they are really independent, then your conclusion is incorrect since a 100% prevalance of omikron would not imply a 0% prevalance of other variants.
There's something I don't understand: why can't we be infected with different variants at the same time ? And does it extend to viruses (eg: can't get infected with flu if currently fighting measles) ?
well, at least with the different coronavirus strains, they are similar enough that getting one is effectively like an immunisation against all the other strains. Now you could probably get two strains simultaneously if you were independently infected separately by both at the same time. Delta, however, isn't quite common enough for that to be likely I think.
Your bodies response to a virus makes it difficult for another virus to take hold, but not impossible. There's a lag in the body's immune response when a virus first is detected, and then another lag while the body builds up the defenders (antibodies and other things). So for someone to have multiple viruses at the same time, largely the exposure has to happen at the same time. The more different the viruses are, the more likely they can be in the body at the same time in a meaningful number. When an immune system is "all revved up", it is very hard for a few thousand virus cells to get exponential growth going needed.
Antibodies (and b-cells and t-cells) for Delta work ok enough against Omicron, and vice-versa. Since Omicron is spreading so fast, it is able to get to more bodies faster than Delta, so Delta has no where to go. Delta did the same to previous variants.
There are multiple factors involved. The extremely high rate of spread of Omicron does a lot to bring it to the top. More subtle is the difference between immunity generated by each. That is, it appears that vaccinations and post infection immunity from Delta are little help against Omicron infections, but post Omicron immunity is highly effective against Delta. This appears to be related primarily to differences in the spike protein.
If having had omicron is reasonably protective against contracting delta in the short term, then this works. For now. Who knows how long any acquired immunity holds up.
Delta did pretty much eliminate prior variants in many parts of the world.
I'd love to see a numbers breakdown estimating the impact Omicron would have on the US if we had a nearly complete (say 90%) vaccination rate. How many infections would we be seeing, how many hospitalizations, how many people in the ICU? How much would this strain our healthcare system? And how would that compare with, say, the flu?
Iceland is 92% vaccinated double and I think 60% of them triple.
Half the famn population is in isoliation because of infection.
Feel free to check their covid stats in covid.is ( they have an english version ).
Most hospitalized are fully vaccinated ( 2 or 3 )
Most serious cases are unvaccinated, HOWEVER.
Out of 34 hospitalized with c19 6 were patients in cardiology that got infected in the hospital and had to be tranferred to c19.
Authorities have not wanted to comment if any of the serious c19 cases came from people who were already seriously ill, already hospitalized and not vaccinated due to that.
Since the ICU numbers are so small, this significance is easily skewed.
Much less hospitalizations than the models predicted.
Id like to add. C19 severity has a very clear link to obesity, Iceland is one of europes most obese peoples.
If omicron is not filling the iceland c19 ward ( I think we are up to 30 patiens out of thousands of active cases ). then I think this wave will pass as more of a scare than anything else.
It certainly disproves the usefulness of vaccine passports.
But that particular science is of course not followed.
If the studies suggesting that Omicron antibodies help protect against the Delta variant, and Omicron seems much more mild in comparison - looks like we're seeing an actual possibility of an end to the pandemic (at least to the point where we deal with COVID like we do with cold and flu season instead of shutting down the world).
Serious question. If Omicron was the initial variant of Covid 19, would we have seen shut downs and the level of global response we did? Is the thought it's only this level of mildness because of vaccination rates?
My gut is that the answer would be yes because this variant targets children more effectively.
The spread is so fast, all charts now look insane and would be terrifying if not for the mild symptoms.
I wonder if it is possible for a virus to wipe itself out by spreading so quickly that it ends up with very few left to infect, assuming it doesn't mutate enough in time.
> we have plenty of N95’s in supply. We also have KN95s for kids.
Are they buying Chinese masks for the kids? Or is there an American "for kids" N95 standard that creates a name collision with the Chinese KN95 standard?
I'm skeptical. The 2020 Winter wave started in October. But cases were decreasing of flat Oct. and Nov. with barely any mitigations in place. There was some sign of an increase in very late nov. and early december. Whether that is an early sign of a wave, a thanksgiving bump, or signs of Omicron spreading, it's hard to tell.
But it Florida and the South had a high degree of immunity to delta even pre omicron.
The 2021 Summer peaks in the south were much later than the equivalent 2020 summer peaks. In 2020 Florida peaked in mid July. In 2021 they only started coming down in Early September.
This would push their winter peaks back as acquired immunity would fade at a later point.
The vaccines were never purported to be 100% effective, and all the data and information was clear that they had lower effectiveness against Delta, and even lower against Omicron.
If people told you that the vaccines would lower your chances of contracting every known major variant and lower your chances of a serious illness, they were right. If they told you that the vaccines were guaranteed to completely prevent every variant of the virus, they were lying to you. If you heard the former but interpreted it as the latter, that's on you.
> According to an archived version of the dictionary's website, Merriam-Webster formerly said a "vaccine" was "a preparation of killed microorganisms, living attenuated organisms, or living fully virulent organisms that is administered to produce or artificially increase immunity to a particular disease."
> The new definition of "vaccine", published in May, reads: "a preparation that is administered – as by injection – to stimulate the body's immune response against a specific infectious agent or disease."
That's incredibly unlucky! I know several people who got Covid pre-vaccine (including myself) and we're all still alive. Although it wasn't exactly a party and most of us (including myself) have been vaccinated since so we could be fairly certain we wouldn't get it again.
The first one is a bit more user-friendly, the second one goes more in-depth into mechanics and research, but neither peddle fear or moralism. There is actually quite a bit of positive news lately:
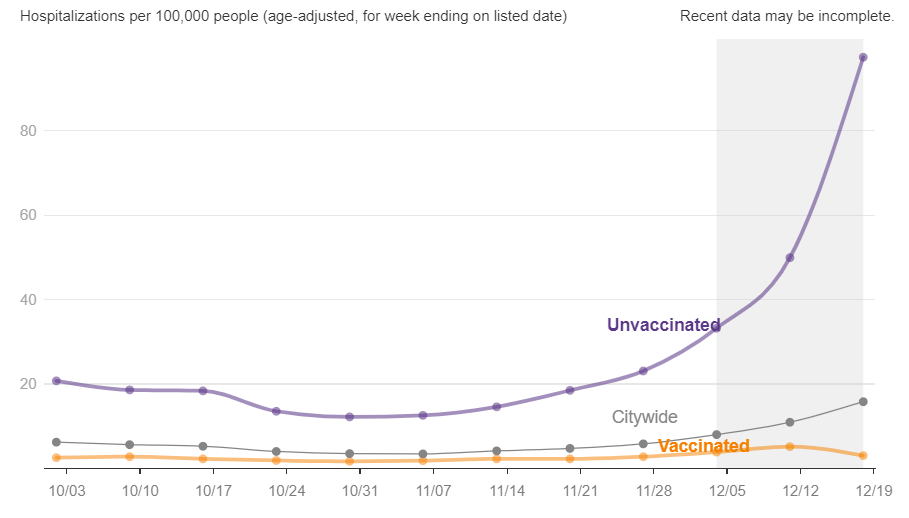{kind=link}
The potentially scary aspects: https://yourlocalepidemiologist.substack.com/p/state-of-affa...
The potentially good news: https://yourlocalepidemiologist.substack.com/p/there-is-good...
Obviously it is still early, but imo those 2 posts give a decent lay of the land.