Summary: the tests were conducted on guinea pigs because they can develop immune reactions to repeated tick bites like humans do. Mice do not seem to be suited for that for once.
The vaccine was administered intradermally. It consists of nucleoside-modified mRNA encapsulated in lipid nanoparticles like we know them from Covid vaccines already. The contained mRNA sequences encode 19 different proteins that are usually found in the saliva of a particular kind of tick in the US. These proteins were selected because of prior research it was known that they seemed to cause inflammatory reactions in the host. The inflammatory reaction that occured at the site of the tick bite hampered feeding of the ticks and reduced risk of disease transmission. The vaccine mostly seems to buy more time to remove the ticks before an infection can take place because the disease causing bacteria was not directly targeted by the vaccine.
Interesting. At first I figured the title was misleading — surely they meant an anti-Lyme disease vaccination — but it turns out that, no, they mean exactly that: anti-tick. They're training the immune system to recognize the tick saliva. This means that the immune system would recognize the bite much quicker, attack anything associated with it, and in general activate the body's innate immune system faster, leading to a faster response by the adaptive immune system.
In their trials on hamsters, none of the hamsters with the vaccine got Lyme disease, even though it wasn't a vaccine directly targeting Lyme.
> the immune system would recognize the bite much quicker, attack anything associated with it
How does this mechanism work? I once had a doctor suggest that I may have developed a food allergy due to some kind of co-exposure event. Why doesn't this happen with vaccines, for example, that anything we are exposed to the same day we get a vaccine we are at risk of developing an allergy to?
Last I heard there wasn’t a scientific answer for why some people developed food allergies like a red meat allergy after a tick based infection so that theory would be pure speculation on the doctor’s part. I’m not a doctor and this information may be old so take it with a grain of salt
The allergy is specifically to galactose-alpha-1,3-galactose, a very common carbohydrate that occurs in both the meat of domesticated ungulates and the saliva of ticks, but which is not produced by primates. The idea is that tick bites initiate an exaggerated immune response, but more study is required.
There is also interesting preliminary work on mRNA for Malaria and various bigger parasites (hookworms etc), along with traditional long-term foes like HIV, RSV, herpes family, etc.
The irony is, in the United States at least, a tick-proofing vaccine would be most useful in areas where the population has a relatively dim perspective on mRNA vaccines.
> The irony is, in the United States at least, a tick-proofing vaccine would be most useful in areas where the population has a relatively dim perspective on mRNA vaccines.
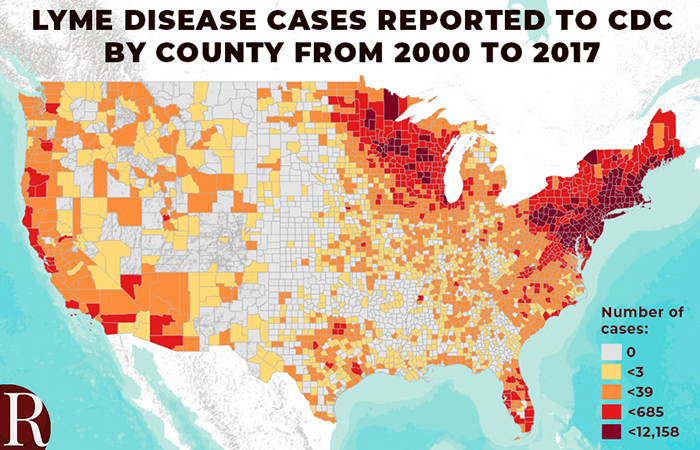
In what sense? The states most affected by Lyme[0] are generally the most (COVID-19) vaccinated in the US[1]
Lime disease rates of infection and therefore risk is higher outside of cities. Of course dramatically larger populations have more cases. So you need to look at county level vaccination data which shows some dramatic difference between urban and exurban populations.
Garret county MD with a population density of 17 people per km2 is 53% vaccination for 12+ where Montgomery county MD 810/km2 is 94% for 12+.
Bedford county PA (19/km2) is 42% for 12+ where Chester county PA (274.9/km2) is 82% for 12+.
If you go outside of the urban areas in those states, you'll quickly enter many deep red areas. Take a look at where the largest outbreaks are occurring in those states, they're often the suburban and rural areas that are 45+ minutes away from urban centers.
Antivax for COVID is different, as it became a political sports contest.
Usually the groups who have low vaccination rates are more extreme religious groups. It’s usually not a big deal from a broader population perspective - the exception being measles.
Oddly we had the current President and VP also saying they’d never take a Trump vaccine[1]. So it’s truly very political for many people and not complete science based even when now they claim to adhere to science. To wit:
September 6, 2020: Kamala Harris says "I think that's going to be an issue" when asked if she would get an approved coronavirus vaccine.
July 28, 2020: Joe Biden suggests the coronavirus vaccine won't be "real" and may not be "safe."
August 6, 2020: Biden says the vaccine is "not likely to go through all the tests that needs to be and the trials that are needed to be done."
September 3, 2020: Biden asks "Who's going to take the shot? Are you going to be the first one to say sign me up?"
September 7, 2020: Biden said he would take the coronavirus vaccine "only if we knew all of what went into it."
As I recall, the context of those comments was in response to a purported attempt to fast-track any vaccine to be ready prior to the election. The Washington Post appears to have the same recollection [1].
The parent is copy/pasting from the linked press release from Trump which exclusively links to donaldtrumpcampaign.cmail20.com. They know they're arguing in bad faith.
Sure, but the lies by omission might only exist in your head. There's no way of him proving that there's no omission, which makes it look like your argument is made in bad faith.
I have the shots. People who don’t are being either political or dogmatic or whatever and a few have legit reasons. But They aren’t the only ones whose beliefs are affected by politics where politics should not be part of the equation. This is an example to show its very political on both sides.
States aren't homogeneous, though, and rural people in blue states can be extra over the top in their performative Trumpism. For example, there's a good case to be made that California Republicans are much more focused on performative Trumpism than on actually winning elections.
There’s different cohorts of trumpists. Remember that he’s a demagogue/personality cult figure, with an orbit of parasites adjacent to him.
Rural people are lowercase conservative in general, but his real power base are blue collar low information nihilists. They see his vulgarity as “straight talk”. But the man isn’t conservative.
Somebody will figure out how to divide and conquer those groups.
Ridiculous. Among others, urban residents who enjoy rural hikes and suburban residents who walk their dogs are all at risk from tick bites. I’ve personally been bitten by ticks more times than I can count, and ditto for my dog.
Edit: and yes I know how to prevent bites, but sometimes when you’re in the US South and hiking on a hot summer day you let your guard down.
It’s fun to say that, and it may be partially true, but Lyme disease is very prevalent in the Northeast United States. If you spend time outside in Connecticut, you’ll eventually find a bite in you with the tell tale circle.
Yes, uptake may not be 100%, but even in “rural” New England, vaccination rates are very high.
Vaccines do reduce transmission, via (a) reducing the chance of becoming infected in the first place and (b) reducing the average duration of the infectious period. As far as anyone can tell, this holds up for omicron, at least for boosted individuals, though it's certainly less effective at preventing infection.
Some Covid vaccines reduce transmission. And it keeps you out of the hospital, which for a human-to-human transmissible disease like Covid (and unlike Lyme’s), is a big deal.
Unless they create a coordinated campaign to oppose an already approved Lyme vaccine to such a degree that the manufacturers think it's too much of a risk to leave it on the market.
But they might require hospitalization or other medical treatment, increasing the strain on the healthcare system resulting in worse outcomes for others.
Question (from a regular joe): is the platform used for mRNA vaccines interchangeable ? Same design and fabrication process, but different payloads ? Or do different mRNA material imply different lipid shells ?
Yes. The ‘platform’ is like a notebook in a ziplock bag. Write the code for $VACCINE in the notebook, place it in the bag, give it to a person. Very interchangeable.
At some point I read that it was useless to release IP on the vaccine itself because the fabrication process is way more complicated and has way more patents on it. Is that true ?
I think the best way to describe the situation is akin to cooking. Imagine the best chef in the world, Michelin stars and all.
Would a written recipe of a 10 course meal result in the same final product?
How about a video of the full preparation?
How about if you went into the kitchen and shadowed them for a few hours?
At what point would you feel confident in your ability to replicate the chef's final product? Would you then be considered the best chef in the world?
How much of the chef's time would you like to take away from serving at their restaurant to training new chefs? What if it was in the middle of Friday night dinner rush? What if that dinner rush was 2 years long and instead of people being hungry, people were dying?
These are the questions I don't see anyone wrestling with in these discussions. Would you trust the expert chef to train new chef's themselves? Or have some outside person, say a bbq expert chef, simply read our above example chef's notes and go for it?
This isn't like high school science where you follow a protocol and out comes a thing. You can't even see the thing you're making! What about instead of taste, you had to rely on touch only to decide if the whole thing was identical (i.e., the analytics are just as complex as the manufacturing). Making these vaccines is much more akin to cooking because the platform/technology is so new.
It took decades for biosimilar antibodies to be approved. Note they don't call them generics--because the product is so complex the process is the product. This was also because the number of experts able to start up new manufacturing took time to get expertly trained.
I would trust the chef to scale-up their apprentices to ensure Quality (with a capital Q) instead of an obviously smart expert chef from some other field to just read the recipe and go for it.
I followed the analogies and the problems you point to and I do agree it's no easy feat to reproduce but I think it doesn't address the question of patents of the many steps: do we need patents to the kitchen sink, a kitchen sink we absolutely need to cook the meal ?
My understanding is that the mRNA payload codes for specific protein production and the lipid envelope is there to protect the fragile mRNA payload during storage and delivery.
This is definitely the case for me at least. I spent a lot of time in the New England woods as a kid and had lots of tick bites. Nowadays I am more cautious, but when I occasionally do get a bite I have a strong reaction at the site and usually find the tick very quickly that way because it’s itchy and inflamed.
I don't know if I just taste bad to ticks or if I'm just lucky. I always find them just crawling around on me without ever tunneling in. Which is good because that is just a horrifying thought. (Live rural Southern Ontario, have both dog and black legged ticks here).
I once had a dream that a tick was on me, and woke in the middle of night to find ticks on the back of my neck. Yowza.
I think it’s a shame it was withdrawn, with a low effectiveness of 80% and even requiring annual boosters I’d view that as a great option if I lived somewhere with deer ticks. Lyme disease is scary.
Veterinary vaccination for lyme disease is common. According to Wikipedia, the human vaccine was withdrawn due to poor market performance.
Claims of autoimmune-type side effects led to several lawsuits, and though CDC and FDA found no connection to the vaccine, the public largely rejected it.
Oh! This happened to me, and I thought I was just crazy sensitive or something, but it turns out to be an actual thing? After a few days on antibiotics for lyme, I walked to the shop to buy sunscreen. Spent maybe 20 minutes outside. Worst sunburn I've ever had.
Anything that can help prevent tick borne diseases is a win in my book. In Western Europe, in many cases that should probably include restoring wildlife habitats...
My dad developed a sun allergy after going on a specific antibiotic following a spider bite. Been too long for me to recall what the antibiotic was, but I remember him having to apply sunscreen for even under his clothes, long sleeves, pants, gloves and wide brimmed hat through out the summer. If memory serves, it lasted several months, quite a while after he was done with the treatment.
Also, I've only seen people mentioning Lyme disease, but Rocky Mountain spotted tick fever is another tick borne disease you don't want to catch. My understanding it's also one of the main reasons a biosafety level 4 facility is being built in Hamilton, MT [0]. Though, I had thought the facility had been built a long time ago.
Doxycycline? I thought that was a known side effect. My dermatologist warned me about it when I went on a course during the summer months. This was over a decade ago, maybe they stopped warning patients?
Doctors seem to forget to do that sometimes, or the patients miss it. Someone I knew was put on a three month course and got a unusual sunburn, later I googled doxycycline and realized the likely connection.
Ooh, reminds me of my days abusing St John's Wort (amongst a great many other things) during Uni days and feeelig my skin bristle and burn in the heat of light shards of sunlight streaming between otherwise closed curtains... .
I think the problem is that the main way of testing for Lyme is to test for the antibodies. So what if you fall in the 20%? How will you know? You'll still end up being treating whether vaccinated or not.
I’m far more more concerned about “undetected tick bite => lifetime incurable Lyme disease” than “detected tick bite => unnecessary course of antibiotics”.
Last summer, I noticed an odd spot on a leg of my female colleague when she arrived at work in a short skirt.
Fortunately, we are good friends and I could tell her without any kind of trouble.
Yes, she had a tick on that precise place a week before. Yes, it looked like erythema migrans, a typical early sign of a Lyme infection (borreliosis). No, she never heard about that and was a bit reluctant about doing anything about it. Yes, I persuaded her to see her doctor now. She got antibiotics immediately and seems to be fine.
One reason Lyme disease is so scary is that it’s really common to not notice that you got bit. How often do you inspect the back of your knees? (If you live in tick country, it should be “every time you get back from being in the woods”, but many don’t know/practice this.)
It’s a common story to hear about people who don’t connect the dots, and don’t get properly diagnosed early when it’s more treatable.
Ok... and you think the people that don't know to check for ticks will know to get a Lyme vaccine? This doesn't seem logical to me. Most people in those environments know to check for ticks in my experience. The ones who don't are not the type to request a vaccine that they probably don't even know about.
It's easier to get one vaccine a year than to check 50 times (to be generous) a year. Also that would only tell you that you have a tick and then you need to check again that you see the red swelling to know you are infected. Then you need to get the antibiotics and then you need to hope that works.
Also I expect/hope vaccinations will develop into some kind of regular maintenance thing like software updates. With the mRNA technology that would be really easy. Scary for many people, also, but really, why not? Every year there are scientifical reasons to update the immunization for almost everyone against certain antigens. This way we may eliminate many strains of Sars-Cov-2, Influenza, other cold viruses, measles, maybe even HIV and the Herpes family eventually.
"It's easier to get one vaccine a year than to check 50 times (to be generous) a year."
This isn't a replacement, you still have to check even if you're vaccinated.
"Also that would only tell you that you have a tick and then you need to check again that you see the red swelling to know you are infected."
Wrong. The red swelling does no occur in all cases. You can be infected without it. Generally, one should have the tick examined to see how long it was attached (if they don't know).
"Then you need to get the antibiotics and then you need to hope that works."
You would need to do this even if you have the vaccine (assuming the tick was attached for longer than 24 hours or there's reason to believe it was interrupted from a previous meal and then but you - testing the tick will tell).
Your "refutations" don't actually contradict anything I said, I just don't dump everything that comes to mind or that could come to mind into every HN comment I write.
Prevention is always better than a cure, so yes you still have to check. Yes I know the Erythema is optional. Yes I know a vaccine isn't 100% effective. I'm actually a licensed veterinarian you are trying to mansplain here...
Most people take a shower every day, especially if they're doing stuff outside. You really only have to check once per day since the transmission risk is essentially zero if attached for less than 24 hours.
This how it’s done in germany. Just got tested for Lyme disease.
Tick bite was in late summer no rash. The skin in the area changed to red/blue after 5 months, so i got tested and the test was positive. Antibodies IgG 46, IgM 5. Now 3 weeks of antibiotics.
It's sort of the inverse. If you're treated either way, then the vaccine is unnecessary. There are risks, even if rare, associated with vaccines. Basically, there's no value added and a very slight increase of risks.
Yes, but I believe the most common antibiotics prescribed for Lyme disease are doxycycline and monocycline, two antibiotics that are used by millions daily (on a somewhat long-term basis) already for the management of things like acne.
While certainly not ideal, with 8 million prescriptions in the US alone, I'm not sure an additional potentially unnecessary course of doxycycline is the worst thing in the world when compared to the possibility that the alternative is full blown Lyme disease.
I know one of the people who is represented in that table. He got bit in New Jersey, and didn't notice the target growing on his chest until he was driving home, and didn't get treated until he arrived home in Washington (because that's where he's insured; go healthcare). The CDC would count that as a Washington State incident.
See point 3 in the study's stated limitations[1]:
> 3. Surveillance data are captured by county of residence, not county of exposure.
Given that he was 1 of 12 cases in that year, I wouldn't interpret that table as proof that the range of Lyme-infected ticks has spread to Washington state.
I'd say that the pandemic just made the mRNA technology more visible and famous. All those vaccines were already in the works.
I actually remember being told more than ten years ago in university lectures about such technologies. And that there was some technology that used DNA bonded to gold particles, and I think those would be shot through the skin or something. Never heard much of that again ... though...
I lived for ~5 months out on east long island NY (Riverhead area) and the tick situation out there is horrible. The majority of people who live out there year round have suffered from some tick-born illness.
Several of my co-workers got ticks and had to go on course of broadband antibiotics. Daily tick checks for myself and my kids was standard practice.
I hope vaccinations will develop into some kind of regular maintenance thing like software updates. With the mRNA technology that would be really easy. Scary for many people, also, but really, why not? Every year there are scientific reasons to update the immunization for almost everyone against certain antigens. This way we may eliminate many strains of Sars-Cov-2, Influenza, other cold viruses, measles, maybe even HIV and the Herpes family eventually.
Usually, there's also no reason not to give multiple vaccines in one go, even mix them up in one vial. It's usually not done for several convenience reasons. Mixing them up makes statistical analysis harder, also you can't demix them if one of them gets pulled and so on. But there's no medical reason there couldn't be a single "general update vaccine" for a dozen or more different antigens.
I was diagnosed with HSV-2 five years ago but I don’t know when I got it, I didn’t go to a doctor right away because my symptoms were so weird. In the beginning of my initial outbreak, I went to a nurse practitioner and she told me I had razor burn. After the symptoms worsened because I did not get treatment, I went to urgent care. They immediately put me on Valtrex, an antiviral medication to suppress outbreaks." I kept Google ‘herpes cure’ until i read an article on Dr Bulukona using herbal medicine to cure herpes, i contacted him. After using the herbal medicine for 3 weeks, I have tested negative for hsv 2. I am beyond enthused and so appreciative, visit website: bulukonaherbaltemple.wixsite.com/bulukona-temple, Email: bulukonasolutiontemple@outlook.com
From my university courses in veterinary medicine I remember them telling us about a vaccine against actual ticks. Particularly the proteins lining the tick guts. Normally those would not enter the blood stream and so no antibodies would be generated against these. Anyway, dogs with this vaccines would get bitten by ticks, and the ticks would eventually die...
Also, why post an article that isn't even available on scihub?
Will this be a neutralizing vaccine? I like the idea of mRNA based vaccines but unless it prevents infections and is permanent like for polio, I don’t see any great uptake if it’s expected to decompose rapidly like the COVID vaccines.
The inactivated polio vaccine used in the US doesn't elicit neutralizing antibodies, just binding ones. The oral polio vaccine used abroad can elicit neutralizing antibodies, but also sometimes gives recipients polio. There are always tradeoffs...
Ideally we’d want neutralizing vaccines wouldn’t we? Before the pandemic, my idea of a vaccine was a preventative measure that worked for long periods of time. I read Harvard did a study of tetanus shots and found boosters had no significant statistically beneficial effect.
I have never heard of a polio vaccine have this issue, I think Salk did an excellent job at testing it’s effects without forcing participants and there’s a great deal of historical data to prove it. Of course a vocal minority may have issues but I haven’t heard them on polio at all, only on relativity new Lyme disease vaccine ‘causing autism’.
I’ll look at binding vaccines more, I just want vaccines that aren’t subscription services.
> Ideally we’d want neutralizing vaccines wouldn’t we? ... I just want vaccines that aren’t subscription services.
I think you're mixing up concepts here. What kind of immune response a vaccine elicits (neutralizing antibodies vs. immunoglobulins vs. B-/T-cell response or some combination of the above) and how long it remains efficacious needn't have anything to do with one another, and vaccines that confer non-sterilizing immunity can still very effectively prevent disease spread. Lots of vaccines don't confer sterilizing immunity and still work very well. Unrelatedly, lots of vaccines' efficacy also fades with time (e.g., MMR, TDaP, varicella, both Hep vaccines, etc.), and those can also be very effective and valuable.
Obviously ideally you'd have a one-and-done, totally sterilizing vaccine for every ailment, but we take what we can get.
> I think Salk did an excellent job at testing it’s effects without forcing participants and there’s a great deal of historical data to prove it
The one that sometimes causes polio isn't the Salk vaccine (that's IPV), it's the Sabin vaccine (OPV), which uses a live attenuated virus -- see https://www.who.int/immunization/diseases/poliomyelitis/endg... for more info. But the Sabin vaccine is still widely used, because it's easier to administer (no needles), this particular issue is rare, and it generally works better than IPV does, because it elicits a gut-tissue response instead of a serum response, and polio is a fecal-oral route pathogen. Like I said: tradeoffs.
> Ideally we’d want neutralizing vaccines wouldn’t we? Before the pandemic, my idea of a vaccine was a preventative measure that worked for long periods of time.
That is because it was the common definition, which is why vaccination treatments were sometimes called immunization. The definitions had to be changed for the COVID vaccines because they perform so poorly in comparison to other common vaccines that they would not be vaccines under the previous definition.
They shouldn’t have changed the definition. I saw them as the same as flu shots. They call them seasonal flu vaccines, the COVID ones have the same issues but decrease their efficiency rapidly.
If people knew it would lose its efficiency so rapidly I doubt they’d have used it, or gotten 2 shots in quick succession.
What would a neutralizing vaccine against ticks look like? And why would it matter that much for a parasite that doesn't usually go from human to human?
The polio vaccination is 4 doses, and a booster every 10 years if you are at risk. Maybe the covid vaccines will fare similarly. Two shots very close to each other isn't ideal for immunisation, we knew that from the beginning.
It would cause tick saliva from causing infection for a lifetime, it matters so you can give a vaccine and not need to upkeep it especially in rural areas. It matters because it will prevent it forever. I think I’m thinking of something that lasts longer, someone mentioned a binding vaccine.
What does at risk of polio mean? I read that polio infections only affect Americans who aren’t vaccinated and touch recently vaccinated baby feces. If you aren’t in that situation you won’t get polio.
As I understand it that's not what neutralizing vaccine means (if it even is well defined). It means you will not get an infection when you are vaccinated, not that being vaccinated will last for a lifetime. This in contrast to leaky vaccines which make you less sick but still allow for infection and transmission. Since this vaccine does not target anything that causes diseases, it's there to make the tick detach, I don't see how neutralizing makes any sense to this vaccine.
>What does at risk of polio mean?
Going abroad to places where there is still polio for example. Checked again and apparently it's not a booster every 10 years but once after at least 10 years.
{kind=link}
The vaccine was administered intradermally. It consists of nucleoside-modified mRNA encapsulated in lipid nanoparticles like we know them from Covid vaccines already. The contained mRNA sequences encode 19 different proteins that are usually found in the saliva of a particular kind of tick in the US. These proteins were selected because of prior research it was known that they seemed to cause inflammatory reactions in the host. The inflammatory reaction that occured at the site of the tick bite hampered feeding of the ticks and reduced risk of disease transmission. The vaccine mostly seems to buy more time to remove the ticks before an infection can take place because the disease causing bacteria was not directly targeted by the vaccine.