You can argue that the ACA improved the healthcare system overall. But it's been tough for people who were already covered by employer insurance.
I think people fail to appreciate that prior to the ACA, when the healthcare system worked, it actually worked really well. I got very sick at the age of 20 while I was still on my parents very modest insurance (pre-ACA). Within 48 hours I had an appointment at the best oncology hospital within 500 miles, and I was able to get scans, tests, etc on a very short turnarounds. Ultimately I had two major surgeries in 4 months, and the whole thing probably cost the insurance company a couple hundred thousand dollars. Since my parents had already hit their out-of-pocket maximum, the marginal cost to us was 0.
Now, the "when it worked" caveat is a big one. The story would be very different if my parents didn't have insurance at all or if I hadn't been eligible to be on it. But the same story today on my insurance would cost me a lot more money out of pocket due to a much higher deductible and a higher out-of-pocket maximum.
My perspective is that the ACA made things significantly better for a small group and modestly worse for most people. I'm open to moral arguments that the tradeoff was worth it (although that's not what I believe.) But I dislike rhetoric that pretends there's no tradeoff at all.
Pre ACA, pre-existing conditions could disqualify you from insurance. People with pre-existing conditions are the people that need health care coverage the most. We can't under-weigh the moral obligation we have to this previously marginalized group, when considering service may be slightly worse for people who have employer coverage.
How I see it: if you were in the pre-ACA pre-existing condition pool, your perspective would be vastly biased in a different direction. And nobody wants to end up in that pool. Nobody chooses that. That's why it's a net win overall.
People died because they don't have coverage (unfortunately, still happens, but substantially decreased by ACA). If things are slightly worse for people who already had access, It's such a small price to pay.
My favorite one was pregnancy being a pre-existing condition so if your husband got fired (noone would ever fire a pregnant woman for no reason), you couldn't get insurance when you needed it the most.
"noone would ever fire a pregnant woman for no reason"
Companies do this all the time. My sister worked at a major oil company that laid off all the pregnant women and new moms out on maternity leave within her department. (To be fair, they also laid off about 1/3 of the rest of the company as well.) It's totally illegal, but if you've just been laid off and have a new baby on the way are you really going to have the money or energy to fight a lawsuit? And even if 10% of people affected did, it's cheaper for the company to settle for $500K or so than to pay the salaries of all the people they fired.
Though (if both spouses were working & had access to employer sponsored insurance), wouldn't the husband being fired result in a qualifying change for the woman, allowing her to enroll on her employer's insurance plan, thus covering the pregnancy?
The point of trying to get on an employer's insurance plans were that people were not excluded for pre-existing conditions because the employer plans were less selective (and also correspondingly more expensive, though the employer contributions hid the additional expense from the employees).
COBRA these days ends up being way too expensive for most people to afford. Perhaps at one time it was a useful regulation. Now it is pretty unaffordable.
If it was useful, it was a very long time ago. I remember my parents being in between jobs in the late 90’s and early aughts and complaining that COBRA was extremely expensive. The only reason the law seems to exist anymore is for people who somehow have some expensive debilitating condition yet can still work (or are a worker covering a family member with such condition). And that’s a pretty small subset of all health insurance buyers.
Why would you expect people to want to open their own wallet to pay for your pregnancy-related medical expenses in exchange for premiums that are much smaller than the expenses you already know you're going to incur?
I don't like the entire concept of "pre-existing conditions". It goes against the entire concept of caring for sick people.
We are all people. We all get sick sometimes. Sicknesses can last a long time, or a short time. Sick people need help. Help the sick people. Pay what you can (a reasonable amount) into a common pool and take what you need (only as much as you need)
> I don't like the entire concept of "pre-existing conditions".
If you have an elective health insurance system where people choose whether or not and when to participate, it implies this restriction.
Say you have private health insurance companies but don't allow them to prohibit members based on pre-existing conditions. Everyone will simply not get health insurance to avoid paying the premiums until the day they need it. That would make health insurance companies completely unviable financially.
This is why Obamacare both eliminated the pre-existing condition restriction and mandated people get health coverage. You can't have one without the other or you get the free-rider problem.
This is another reason why healthcare should just be universal. It doesn't work at all like an actual efficient market product.
Would a wait limit, like with hurricane insurance, help to mitigate this problem? You can't wait until the NWS declares a Category 4 storm is barreling towards you to buy coverage. I mean you can, but the coverage doesn't kick in until 30 days later.
Or turn it around and make it equally burdensome to both insurer and patient. If you acquire a malady while insured by a particular company, all medical expenses that are tied to that diagnosis must be forevermore paid by that insurer, even after the policy lapses, is cancelled, or the patient switches insurers.
If that sounds unfair to an insurer, that's great--now they know how we feel about it.
Insurers want to deny pre-existing conditions because they don't want to add already-sick people to their risk pool. They wouldn't have to, if the previous insurer was still on the hook for that diagnosis. But they'd never agree to that, because it exposes them to some of the same insolvency risk due to medical bankruptcy that some patients have to face.
Surely "what you can" should be relative to both your income and your need. We'd need to supervise the system to make sure people aren't taking advantage or else the whole system goes broke.
> into a common pool
We could also invest the money in the pool to make some extra cash and reduce what people need to pay in, we'd have to have an organization do that too.
> (only as much as you need)
How can we know what people need? We'd have to charge a token amount for office visits and medication so that people aren't frivolous with their medical visits, while perhaps guaranteeing an out of pocket limit in case of extreme illness. We'd also need some kind of system to verify that people are only taking what they need.
We probably have different ideas of "paying what you can". How do you judge whether someone is only paying what they can, or they are taking advantage? Not a rhetorical question.
One way is like we do today -- highly-paid positions often come with high-quality insurance, which is (ime) fairly expensive and low-paid positions have less expensive insurance that is a bit worse (all this on average, I'm sure there are outliers).
We are in different pools today but I don't see how that's meaningfully different than everyone being in one pool if the individual pools are large enough and you can't discriminate the population of the pools.
There are cases where it’s hard to tell if someone is truly paying what they can, but there are also cases where it’s easy: when it costs more than they can pay. Health insurance trivially fails the “paying what you can” criterion for sufficiently poor people.
Your employer could fire you, though, if you all of a sudden developed an expensive medical condition. HIPAA would say that's illegal to do, but it'd be incredibly difficult to prove that was the reason you were fired.
That's a slightly maddening thing about many these comments. If you were getting your healthcare through an employer, you had a lot more security both on the pre-existing conditions end and on the keeping coverage end.
I remember several stories in the news before the ACA about employees being pressured to find private insurance or even getting fired because they were raising the group plan's costs. Are you sure it's so cut and dry that it's something you should be maddened about?
I don't know the details but my understanding is that it is partly covered by tax law - if the employer kicks employees who get sick off the insurance, they (and all the other employees) lose some or all tax deductions for health care premiums. The employer can, however, still fire people to get around that.
True but we could have had preexisting without all the other garbage included. Some of it sure but overall I have yet to see any compelling data to say the tradeoff was efficient.
pre-existing conditions could disqualify you from insurance
Only if you chose no insurance before diagnosis.
Under Obamacare, people can go with no coverage at all and, once diagnosed, then get care paid for without penalty. It's like letting people drive without insurance, then making insurance companies write retroactive policies for them after an at-fault collision.
"There were supposed to be millions of people who were uninsurable because of pre-existing conditions. We heard lengthy testimony about their terrible plight. I don't think it's too strong to say that this fear--that you could get sick and no one would insure you, that's right, you, Mr. & Mrs. Middle-Class Voter--was one of the main reasons offered for the health care overhaul. It was estimated by Medicare's Chief Actuary that around 400,000 would sign up (the CBO estimated 200,000, but only because they assumed that HHS would use its authority to limit enrollment in order to stay within the $5 billion budgeted for the program). So where are all the uninsurable people?"
So if this is accurate, that is the size of risk pool isn't that large. Wouldn't be better to create a special program for people who fall into this category?
> Wouldn't be better to create a special program for people who fall into this category?
Why? The only difference between "people who have already been diagnosed with cancer" and "people who are going to be diagnosed with cancer" is that you know who the first group is. The second group is hidden among the "healthy" people.
You didn't understand what I wrote. I am talking about the group of people that were uninsurable because of preexisting conditions. This group of people was used as a reason for the ACA. However when a pilot program was run before the ACA went into effect, the size of said group appeared to vastly over-estimated.
So the reason for a special program would be to help the people that need it and not mess with the entire country insurance.
I'm not seeing the connection to the ACA in your argument. If your argument is that the ACA raised the price of health insurance, that's incorrect: health insurance premiums had been skyrocketing prior to the ACA (that crisis was what generated the political capital to pass the bill), and the ACA in fact reduced the rate of growth in health care costs.
While the growth rates for healthcare have been lower over the past decade I would be hesitant to attribute it to the ACA. Most of the higher rates over the previous 30 years were due to landmark legislation increasing demand for services. If you take a look at numbers you might be less convinced.
year | growth rate
2005 | 6.7% (Bankruptcy act passed making it harder to discharge medical debt)
2006 | 6.5%
2007 | 6.5%
2008 | 4.5% (Great Recession)
2009 | 4.0%
2010 | 4.1% (ACA Signed)
2011 | 3.5%
2012 | 4.0%
2013 | 2.9% (ACA Taxes)
2014 | 5.1% (Exchanges Open)
2015 | 5.8%
2016 | 4.3%
2017 | 3.9%
There are also a couple of timing advantages that people give credit to the ACA that would have happened otherwise.
There were a lot more prescription drugs created after the Orphan Drug Act and the Hatch-Waxman bills of the early 80's. So the timeline for that is 83-84 laws passed => research => 1990-1999 prescription drug explosion => 2010 - 2019 patents expire. This lead to a dramatic increase in costs over this period, but this is good since people now have access to drugs that wouldn't otherwise exist. The patents expire and the costs decrease, and they won't likely increase further due to the nature of those bills.
You could also make the point that from 2001-2006 you should see higher healthcare costs due to war.
A lot of the calculated savings are based on government projections of future spending. We can go off on a tangent on how good the CBO is at its job, but I think we could agree that predicting the future is hard and people are frequently wrong about their predictions.
Furthermore, lower costs aren't necessarily a positive thing. To put it simply if you are buying a BMW and I am buying a Kia, they are both cars but you aren't unhappy to pay the higher price.
Percentage increases also get harder to maintain as time goes on.
The numbers here are quite helpful. The parentheticals are harder to understand and, for that matter, so is "higher healthcare costs due to war" (we have a nationalized health care system for war veterans).
I wouldn't expect it to be clear unless you've studied the area for awhile but all of those are external shocks to the marketplace.
Healthcare expenses increase during wartime since you have to treat newly injured veterans. That statement basically can be interpreted as "people get injured on battlefields and it costs money to treat them".
First, once again: we have a nationalized health care system for injured veterans. They not only have a separate payer system but also a separate provider system.
Second: I have followed health policy for quite awhile, and it's not clear to me at all what impact you believe your parenthetical callouts had on health costs.
First: I know you're not stupid so I have no idea what you aren't understanding when it comes to veteran care costs increase during wartime. Of course they have a separate payer and provider system. That system is included in the growth rate statistics. It should be fairly obvious that people being regularly shot at have higher healthcare costs.
Bankruptcy Law:
In 2005 there were 2,000,000 bankruptcy filings, in 2006 there were 600,000. This was a result of the passing of the BAPCPA in 2005. At that point in time 46% of bankruptcies were due to medical bills. This change increased the expected value of delinquent accounts which in turn should lead to lower costs for medical services.
Great Recession:
People put off non-essential medical expenses, or delay usage of medical services. Someone who might get braces doesn't, someone might take care of a parent themselves instead of hiring an in-home nurse, etc.
ACA Signed:
Marker for before and after growth rates.
ACA Taxes + Exchanges Open:
The two main policies of the ACA intended to curb healthcare costs go into effect. I would classify these two years as overestimation of savings and regression to the mean. Most insurance companies had to backtrack after their financial projections did not materialize.
No, I do not believe veteran health care is included in the statistics you are citing, and I am similarly dubious of your explanations for how each of those other 4 events impacted health care costs, because everything I've read suggests that the impacts are way more complicated than they look (for instance, much of the health cost impact from the "Great Recession" wasn't felt until years after).
Here's the dataset that I'm referencing.[0] From the summary documents, "DOD spending in the NHEA excludes spending that occurs outside of the United States." I'm not certain whether this does or does not include forward operating bases. (Post offices count those as being in the United States so I believe they are included; but I could be wrong) Nevertheless it does include domestic spending on veterans.
Also, many veterans get care outside the VA. From my own experience working with these people, they cite long waiting times or broken relationships with the government for not wanting to take part in that system.
I'm not trying to downplay the complexity of the healthcare market, it's really complex. However, it I were to pick the things the government had control over and impacted the marketplace the most over the last 15 years, I still would pick the same things I did. I could fill several books with other changes that impacted the cost of American healthcare. (switching to e-prescriptions, subsidies for electronic medical records, medicare part D, certificate of need laws, FSA changes, HSA changes, consolidation of pharmacy benefit managers, health system consolidation, the opioid epidemic, the rise of the physicians's assistant, the expanding role of nurse practitioners, etc.)
I'd rather spend my time continuing fixing the things I know I can make better.
I've excerpted this from page 34 for your convenience.
"Other public programs include health insurance coverage provided by the Department of Veterans Affairs
(VA) and the Department of Defense (DOD). Enrollment for other public programs for 1987-2011 was
estimated using the levels from the enhanced CPS (SHADAC) and for 2012, 2013, and 2014 estimates
were extrapolated using the CPS. "
None of these appear to contain the table you posted at the root of the thread, the table you now claim also includes the increased cost of veteran care due to the wars in Afghanistan and Iraq. Can you just tell me how you made that table, so I can look at the source and evaluate your claim that it incorporates increased costs in the VA along with private health care?
The raw data comes from the following sublink from the first link in that group "NHE Summary including share of GDP, CY 1960-2017 [ZIP, 27KB]"[0] I computed the table by hand. You can recompute it if you like.
Oh, for God's sake. The Kaiser foundation just tracks the stat we're actually talking about directly. Here's the numbers for employees covered by group insurance provided by their employers:
Can you provide a reference for this data, I'm not 100% sure what I'm looking at. I deleted a previous comment on why I think the data I used is better for analysis but I want to confirm that this is what I think it is before I comment further.
I'm sorry for getting snippy, I just couldn't untangle your numbers from your source even after you pointed to the raw XLS you got it from.
If we just stay focused on commercial health care, we don't have to litigate whether the Iraq War (materially) impacted health care costs prior to the ACA. And: this thread is about whether employer shifts to HDHPs and (more broadly) the ACA has impacted those specific costs, not the total government cost of providing all health care services.
Can you give me a deeper link to the specific data from which you drew the table you posted above? There's a lot of stuff hanging off the link you just posted.
I signed up for the ACA the year it came online. Over the years I went from a sub-$100 plan that actually covered things to paying $300+ per month for the "hit by a bus" plan that was so expensive, one year I said fuck it and paid the penalty instead. I understand well what could have been had something truly happened, but I ended up saving money paying the penalty while still having a few minor doc-in-a-box visits out-of-pocket. I also say a number of insurers go out of businesses such that now your only option in my state is the BCBS.
Say what you will about the ACA, but requiring folks to purchase a product while doing not curbing the rampant greed in the industry screams of corporate welfare to me.
If you're saying the ACA didn't completely fix the US healthcare system, I strongly agree.
If you're saying the ACA harmed the health care system, strong disagree. Again: the cost increases you're talking about were a fact of life before the ACA. There is no evidence that your costs would have leveled off without the ACA, and substantial evidence that the opposite would have happened.
The increase in costs were most certainly driven in part by the ACA changes. No longer allowed to deny based on pre-existing conditions? Insurers need higher rates to cover those costs. Require a bunch of things be added to mandatory preventive visits? Those have to be paid for as well.
That said, I agree the costs would have continued to go up, but to say there is no evidence that the ACA contributed to it is just ignoring the math.
I had the same experience where as a sole proprietor health insurance for a family of 5 is now $2,000/month. $24k/year not for great healthcare, but for the privilege of paying a "discounted rate" on "select services" when you actually need healthcare.
We haven't needed the coverage for two years but when we did, what we needed wasn't covered so we paid full price anyway including $80 for a bottle of Ibuprofen that was casually offered to us. The markups are almost criminal.
For a $1M home you can find insurance for $1,500 per year. It's exponentially less expensive.
ACA was the worst possible compromise to a serious problem. A public option, universal healthcare or deregulation all would have been better options.
It'd be much nicer to be able pay a doctor to make house calls as needed and waive your right to a malpractice lawsuit than to pay to support this insurance/legal/government system we have now.
> No longer allowed to deny based on pre-existing conditions? Insurers need higher rates to cover those costs.
Is there any alternative though? We're going to pay those costs one way or another: either the government pays for all the unprofitable patients' healthcare (the wet dream of health insurers), or we tell those people to go fuck themselves.
Those patients have no coverage so get Emergency treatment for acute symptoms of their issues that rarely fix the underlying problem, and beyond that we also tell them to go fuck themselves.
You are "most certain" about something that empirical data refutes. Health care costs grew more slowly after the ACA than before it and, in particular, at no point subsequent to the passage of the ACA have health costs grown more than they did during the Bush era.
There are all sorts of things that should have (and perhaps even did) impact prices after the ACA. Not just coverage requirements (which, again: most employer-provided health plans --- which is what we're talking about here --- already complied with), but, more importantly: unprecedented instability in the insurance markets during the almost decade-long concerted effort by the GOP to hamstring and ultimately repeal the bill. And yet, the numbers are right there: health care costs are growing, but they are not growing more than they were prior to the ACA.
I don't understand this argument. The ACA changed a bunch of things about the health care system. It reduced some costs and increased others. The point is to reduce the total cost (or, in this case, the total rate of increase in health care costs).
The government subsidizes ACA plans for many participants. That was partly meant to soften the impact of requiring coverage for pre-existing conditions. And then there is/was the individual mandate, to get everyone to contribute even if they were currently healthy. The ACA also imposed a tax on high earners (IIRC, >=200K, not sure if it is inflation adjusted) to fund the subsidies, and it cut spending on Medicare Advantage, which costs the government more than the other medicare plans.
That being said, I'm not disagreeing that costs went up after the ACA more than they would have, but, IMO that was just insurers/providers raising prices because they could.
There's no evidence that costs went up after the ACA more than they would have, and, in particular, costs grew significantly faster under Bush than they have at any point after the ACA. I'm not sure I understand why we're supposed to give credence to HN-style first-principles analysis of why insurance costs should have increased; in particular, most employer-provided health plans already complied with the ACA's coverage requirements. The data simply doesn't back these arguments up.
Ours were going up sharply before too, at Matasano (2005-) and before we started Matasano, our health insurance at my previous employer also got slashed (2001-).
> If you're saying the ACA harmed the health care system, strong disagree.
The system? No. Corporate welfare is great for "the system." But the consumers? Absolutely harmed!
> Again: the cost increases you're talking about were a fact of life before the ACA.
I've been working for over a decade now. 100% increases, year-over-year have never been even close to a thing with employer plans I've held. Not even close. Typically something in the realm of $20 per year at worst for a quality plan.
Here is another fun anecdote. I recently lost a job, and my firm was too small, with only 4 insured, to qualify for the COBRA. Total premium for the plan was roughly $150, roughly $75 per party as my employer paid 50%. Comparable coverage through the same insurer through the marketplace would have cost me nearly 4x as much.
The reality is the ACA allows insurance firms to sell obscenely over-priced plans to consumers. A sane system would have seen price controls in conjunction with the requirement for insurance. Instead I am forced to pay an insurer, pay the government, or prison. I would happily pay taxes for a fully nationalized system, but the ACA is obscene.
> The reality is the ACA allows insurance firms to sell obscenely over-priced plans to consumers.
As far as I am aware, the ACA actually introduced limits on how much mark-up health insurance can have, where 80% of the cost must go to actual medical expenses, and administration, marketing, etc must be no more than 20% total. So how is the ACA the cause of insurance mark-up?
I think the actual root of the problem is not mark-up but that health care in the US is quite expensive (and always increasing). The ACA in some cases shifts who pays for it (young healthy people pay more), but it doesn't appear to change much the overall cost. It sucks temporarily for those younger people, but considering they will most likely become older, less-healthy people over time it doesn't seem that unfair overall.
> A sane system would have seen price controls in conjunction with the requirement for insurance.
If you are paying 4x more though, it sounds like the marketplace may be breaking down in your location with a "death spiral", where the price goes up, all the healthier people leave, causing the remaining insurance pool to be even sicker and the price going up even more. The whole purpose of the mandate was to prevent this, but it looks like it's been repealed. Price controls in that situation is hard since the pool is actually expensive to insure, I don't think the government can force the companies to sell at a loss. To reverse it maybe they could re-instate the mandate, or change it to a tax, or add a public option. Or, of course, give up on insuring pre-existing conditions.
> I would happily pay taxes for a fully nationalized system
Keep in mind, there are other countries like Germany and France that have private insurance markets and much cheaper care. I think it is fully possible for the US to implement a nationalized system that does not achieve the cost-effectiveness that we want. The VA system might be an example of how that might go.
> As far as I am aware, the ACA actually introduced limits on how much mark-up health insurance can have, where 80% of the cost must go to actual medical expenses, and administration, marketing, etc must be no more than 20% total. So how is the ACA the cause of insurance mark-up?
One of the issues (and I like the ACA generally), is that that limit removes an incentive for the insurance companies to control costs and the 20% markup becomes a floor, not a ceiling. If they get 20% of revenue as non-medical costs, and they want to increase their profit, the best way to do that is to allow medical costs to increase. Then their 20% is larger because the pie of costs is larger.
Presumably they could pass along the savings and increase revenue by expanding their market share, or lose revenue to a company that controls costs. I see your point though, and in a given year it might be easier to increase medical expenses by 5% than to grow market share by the same amount.
One thing I wonder though, is that even without the 20% rule, if the company can get away with raising rates by 5%, wouldn't it make sense for them to do so? If they started with a 20% margin that would increase their profits by a whole 25%, instead of a measly 5% with the cap, so you'd think the incentives would be even stronger. It seems like adequate competition is the most important thing in a for-profit insurance model rather than having a 20% margin rule or not.
In a healthy, actually competitive market, I think that would work, but there are so few insurance operators in each market, it's really easy for them to quietly collude with each other rather than compete. Additionally, everyone else in the industry wants higher prices and more profit. They are not limited to a 20% cost margin. The insurance companies are supposed to be the downward drivers on price. However, here, it's just easier to not fight the price increases, take your 20% of the increase, and move on, rather than fight hard to push prices down, and gain market share.
I think many economists would say that while you had an employee-based plan your costs were actually going up significantly, you just didn't see it because those increases were coming out of (what would have been) your yearly salary raises.
I don't think ACA plans are much more expensive that what we are _really_ paying for employer insurance. I recently became unemployed and when I priced it out, an ACA plan that offered benefits similar to what I would get with a COBRA plan were pretty much the same price - both ridiculously expensive, so I went with a cheaper silver HMO ACA plan. And my old employer charged a 4% "fee" on COBRA premiums as well - I guess the benefits companies want some of the action.
> The only connection you’re making here is that your own costs went up after the ACA.
The connection is that the ACA rates, and rate-increases are out-of-touch with the employer-offered system, even when those firms are tiny and not nearing some kind of "scale" cost-savings.
I have been hollering about this issue for years, and I've yet to have someone say "Ya know, I actually experienced something radically different." So where is all this evidence you claim but can't be bothered to provide?
I'm having trouble parsing what your argument here is. Are you saying that rates on the individual market are more expensive than the large group market is? Yes, that's true, and always has been (the small group market is effectively a facsimile of the individual market, for the obvious reason that there's not much actuarial benefit to pooling 10-20 random people).
There also isn't one "employer offered" system. In addition to the aformentioned small-group marketplace, there are also large group plans that cover big companies, and very big companies often self-insure, using health insurance companies solely to administer benefits but financing the care themselves. Can you be specific about which of these kinds of health care financing have been impacted by the ACA, and how?
When I look at what my insurance company actually covers for all of my doctor bills, I'd probably be better off just paying the penalty. At least I'd have a few hundred more every pay check to cover that 11 extra dollars that my insurance company could dare to part with for a $300 X-Ray.
The penalty has been more or less hamstrung by the GOP, so if that's your only consideration, then, yes, you're better off not paying for health insurance.
Additionally: you can (you shouldn't have to, but you can) shop around for cheaper medical imaging. Imaging in particular has wildly varying prices, and if you stay on the "happy path" your PCP and hospital puts you on, you're going to pay the higher end of the range of prices.
You are not, as a general matter of life advice, better off going without health insurance. Rather, find the least expensive HSA-qualified HDHP, fund the HSA with the savings, and pay for routine care (effectively) out-of-pocket. The point of insurance isn't to make your annual checkup cheaper, but rather to avoid going bankrupt if you get hit by a car or your appendix bursts.
From the way you write, your appendix presumably hasn't burst yet. That's great! Neither has mine! My house has also not caught fire† and I have not managed to crash my car into a fully occupied city bus. But I am insured against both of those things, too.
I should probably specify the level of "tongue-in-cheek" in which my dismissive comment was made. I'm well aware of the function of medical (as well as other) insurance. Having a family, I'd be a fool to "go it alone". But you're correct, it's my responsibility, especially as one who chose a HDHP this year, to shop for the best deals.
And nope, still on my original appendix... I change the oil regularly.
It is corporate welfare, I remember lots of libertarian arguments to that very point. But to solve health care in the US you would eventually have to start questioning the for-profit underpinnings of the whole enterprise. That was far too much to expect from the generally pro-market Democrats in office at the time.
Even after Bernie Sanders, the "Very Serious Democrats" talk more of protecting the Health Insurance Industry than anything else. Best case, we'll see a timid proposal of a expensive Medicare Buy-In added to the ACA exchange that will never get past the Senate.
I used to dabble in enjoying quips like this. They're simple and fun and sound insightful and knowing. But when I look around me I see no truth to them. We have two parties with very distinct philosophies making very different arguments for how the future of our culture and economy should function. "Capital" influences both of them, in different, sometimes overlapping, ways. But they have many differences across many axes.
In my previous career, I was an accountant, and I worked for a health insurance company, you are straight up uniformed if you do not think that ACA raised the the cost of insurance.
With that said, as a type 1 diabetic, without ACA it would be impossible for me to get insurance outside of employment, so i think there is some good in it, just needs to be actually thought through, unlike what the administration did that put it in place.
It's impossible because you both political parties want exclusively mutual results
You can't have cheap insurance without making it mandatory since only the sick will get it
You can't have easily accessible insurance without forcing healthcare companies to comply with new regulations forcing them to increase costs
You can't have good insurance if you aren't willing to pay the market price which happens to be very inflated in the US
You cant lower costs in the US without having a more aggressive regulatory body which 50% of political bodies strongly oppose alongside lobbying efforts
Overall, it's a shitshow that will keep being patchworked every time the administration changes between parties.
> You cant lower costs in the US without having a more aggressive regulatory body which 50% of political bodies strongly oppose alongside lobbying efforts
Here is the fundamental problem from my point of view. Compare human medical costs to veterinary costs. Yes, people expect a slightly higher standard for themselves than they do their animals, but you can get a major knee surgery for your dog for a small fraction of what they charge for humans. The process is performed in a sterile environment by professionals in either case. We're smarter than animals on average, but our bodies and medical needs aren't vastly different.
The problem is price gouging because the providers and insurance companies know we have no real ability to shop around. They conspire with each other to publish false rates when the true costs are much lower after you agree to them.
You could maybe solve this with regulation on prices (a socialist approach), but you could also solve it by mandating they advertise true prices and re-enable competition (a capitalist approach). Either way could fix this, and the problem is corruption (lobbying) not party ideology.
Maybe these aren't the "true prices"? I certainly wouldn't know where to look to find how much a "knee surgery" would cost, and I'd probably need to know some obscure medical code I don't have access to, as well as the intricacies of the knee surgery to know exactly what price to look up. I don't know how publishing "true prices" would work.
What kind of knee surgery am I having?
Will I have to pay extra for the anesthesiologist? What kind of anesthesia will they be using?
What about surgery preparation? What costs do I need to include for that?
What about post surgery? There's probably a dozen cost items to add to the total for post surgery.
The nurse brought me a glass of water. I'm not sure if that comes with a charge or not? Presumably someone has to pay for the plastic cup. Etc.
>Maybe these aren't the "true prices"? I certainly wouldn't know where to look to find how much a "knee surgery" would cost, and I'd probably need to know some obscure medical code I don't have access to, as well as the intricacies of the knee surgery to know exactly what price to look up. I don't know how publishing "true prices" would work.
This is exactly the problem. They publish "prices" but those prices don't mean anything.
Published medical prices are not real because most procedures are paid by collective programs like private insurance or Medicare, which use their bargaining power to pay less--sometimes MUCH less--than the public "list price".
You're right that the complexity of medical billing also makes it difficult to anticipate and compare prices. However, that might be more of a side effect of how the billing is done, rather than an unavoidable attribute of medical care.
Arguably, medical providers have the information and capability to package procedures and publish what it actually costs to do them. But they have no incentive to do so, and many incentives to not do so.
> you can get a major knee surgery for your dog for a small fraction of what they charge for humans.
I mean you can't really compare vet bills to surgery bills. Veterinarians have actual price constraints where the owner is willing to put their foot down once it gets beyond a certain point. They love their pets but they aren't willing to go financially insolvent for them.
No such constraint exists for American healthcare. You pay what they tell you until you are destitute and on Medicaid.
> by mandating they advertise true prices
I think most Americans want this to be the solution and it still won't work unless there is pressure on the entire system. Doctors, hospitals, surgery theaters, radiology, and diagnostics have such complex billing that even if you could price compare are you even capable of understanding what those options do?
Well, the start would be mandating that the cost must be same to all patients. Which means that uninsured/underinsured patients will face bills no greater than the payout the medical professionals get from large health insurance companies. Part of the problem is that no only are the prices not transparent (for comparison shopping), they are also different for different buyers.
Many many years ago, auto mechanics would gouge customers after fixing their cars. This resulted in laws in all US states requiring written estimates in advance.
We should expect hospitals to meet the minimum ethical standards of auto mechanics.
You don't even have to go all the way to veterinary medicine. This is an old article, but compare the $100,000 cost for a joint replacement in the USA vs. $13,000 for that same procedure in Belgium. https://www.nytimes.com/2013/08/04/health/for-medical-touris...
It's impossible because you both political parties want exclusively mutual results
You can't blame ACA's flaws on party disputes -- Republicans were allowed no input to the process, and it passed on Democrat votes alone. Republicans and rank-and-file Democrats* weren't even given the final bill to read before the vote*.
> you are straight up uniformed if you do not think that ACA raised the the cost of insurance.
The post you replied to said:
> the ACA in fact reduced the rate of growth in health care costs.
Meaning the RATE of increase slowed. The Department of health & Human Services estimates that the ACA saved $2.3T up through 2017 ($650B in 2017 alone). Premiums haven't gone down, and they weren't estimated to.
You're laying the blame at the administration's feet but you're ignoring the complete shit show in the legislature that resulted in what we have today. They compromised and compromised and finally surrendered major concessions to someone in their own party to get it passed. I'm shocked it did any good at all.
Anecdote, but the two years pre ACA my premiums went up about 9% each year. After ACA it was about 6% each year. Pre ACA my employer said "Sorry. Premiums went up from insurance companies." Post ACA employer said "Blame Obamacare."
Employees being people bought the "Obamacare made my premiums go up!"
lol, You might want to take in account who you are replying to. tptacek is one of the more prolific commenters on HN. And just to be clear, he was talking about 'rate of growth` in costs, not absolute costs.
The choice of covering crappy plans is the employer's choice... and crappy plans are what have been pushed AFTER the ACA was passed. Largely by the GoP...
Is that what the ACA was, or what someone(s) who want it to fail want?
There's a weird narrative where any event is tied to the ACA while they ignore what the healthcare system is in the US overall.
The cost to employers of very good plans massively increased after ACA went into effect. When this changeover happened, I was running a company where we paid 100% for one of the best healthcare plans available in the state for both the employees and their families -- people really appreciated this benefit. This was the polar opposite of a "crappy plan", and it wasn't inexpensive to begin with.
After the ACA, this plan became so expensive so quickly that continuing this plan became nearly untenable financially and now these types of plans have become increasingly unavailable in any case due to that cost escalation. If you were formerly on one of these plans, of course the post-ACA environment seems like a big step backward. This happened in one of the deepest of blue states; the Republicans can't be blamed for the destruction of health insurance benefits here because they were never involved. The cost of healthcare here has not risen nearly as fast as the cost of providing top-tier healthcare benefits did.
This happened to me. I had what is considered a "Cadillac plan" which my employer offered generously as a benefit. After ACA, the government began to tax that plan and our public company could not justify that while other companies in our market were offering much lower quality plans. Thus my medical spending rose by thousands of dollars per year (also thanks to an unfortunate @$3000 hospital stay but that would have cost me $250 on my old plan). The old plan did of course come with a lifetime max but obviously was not a factor at my age yet.
I think the ACA does good things for people who needed it. And generally I've been against repealing it, but only because there has not been an adequate replacement as part of the repeal, only "trust us, we'll do something great".
What was the lifetime max on this plan? It probably would have left people out in the cold when they most needed it. I don't think it's wrong to expect insurance to cover people when they most need it, which was largely not true with million dollar lifetime caps.
Even with the ACA, employers have the best of both worlds. Expensive older people are covered by the government, and anyone who gets to expensive can be shuffled off with a little cover and the joy of "at-will" employment.
The lifetime max was multiple millions, I don't remember the exact number. As I stated, it was just about the best policy available for any amount of money. There is no credible way to spin this as actually being worse for those employees. I like to hire "expensive older" engineers, so dialing healthcare benefits up to eleven was intended to attract that kind of employee.
All insurance policies have implicit lifetime maximums, unless the laws of economics and finance have been repealed.
> What was the lifetime max on this plan? It probably would have left people out in the cold when they most needed it. I don't think it's wrong to expect insurance to cover people when they most need it, which was largely not true with million dollar lifetime caps.
Note that lifetime caps are a lot more generous than what they have in say the UK, where you don’t get treatment if it costs more than $50-75k per year of extended life. (So to blow through a million dollars, the treatment would have to be expected to produce 15-20 years of extra healthy life. Most treatments offered when people “need it the most” can’t make that sort of promise).
> Note that lifetime caps are a lot more generous than what they have in say the UK, where you don’t get treatment if it costs more than $50-75k per year of extended life
https://www.bbc.co.uk/news/health-28983924. It’s not odd at all. It’s a basic thing that makes the UK’s health system work. US insurers (in the past) would piss away a half a million or a million on uncertain treatments. (And then the family would go out of pocket, go broke, and there would be an article on medical bankruptcies.) The UK doesn’t do that. Instead, it’s very aggressive about justifying costs with expected outcomes.
This is exactly the point I was trying to make in my original comment. Really good healthcare plans (with minimal deductibles and great coverage) used to be a benefit that employers could reasonably provide. Employees/family members who got sick would get good coverage without going broke. Now the cost is of providing that kind of coverage is completely untenable.
I don’t see what the purpose of pointing out the fact of health insurance being cheaper when it doesn’t have to provide coverage for people who actually used healthcare. Goal is to provide all of society with healthcare, problem is voters didn’t want to pay with their tax dollars. Now they get to pay with their insurance premium dollars. There never was a free lunch, only people who were unable to get health insurance.
The parent comment is exaggerated, but I think the point is that prior to ACA, employer-provided plans tended to be cheaper and have lower deductibles largely because insurance companies were able to drop or deny coverage whenever they felt like it for individual plans to keep their margins up. While logically true, this is roughly equivalent to hearing from an old coworker that South Africa was a great place to be white under apartheid...
I think it's also worth exploring how much of the difference in financial cost of health insurance plans is due to time + annual overall increases in healthcare cost in the US. ACA was passed 9 years ago. Even under the previous 9 year annual percentage increase averages, you would expect healthcare costs to be at least 20% more expensive than they were in 2010, regardless of ACA.
It's more extreme than your example. The parent is ignoring the fact his great healthcare experience is predicated on them being able to drop him the moment they could, when his illness became too expensive.
Ending pre-existing conditions was the game changer in the AMA. Treating people is obviously more expensive than not treating them.
That's just not how it worked with employer insurance. Perhaps they could drop your whole company, but the insurer couldn't unilaterally cancel a single employee's plan.
I know someone who pre-ACA had employer insurance who was dropped by that insurance after they got skin cancer. The official reason was lying during the application process (10+ years earlier).
They forgot to list childhood Asthma on their application form ten years earlier.
I would argue that the incentive was implicit and fundamental to the nature of the business, because it provided agents with a method to pick and choose their clients.
By inducing lapses in insurance coverage, insurance companies were able to convert illnesses under active treatment into preexisting conditions.
Witness all sorts of horrible behavior, like employers saying "Sorry, all, no raises this year, because one of your coworkers was using so much of our health insurance pool that they raised our rates!"
Yes: if you go back in time, health care costs go down, because they've been rising rapidly over the past 20 years. But the only thing that happens at the point in time when the ACA passed is that the rate of growth in cost falls.
It also impacted prices all the way into 2012, by moving people out of full-time employment and onto COBRA, and by reducing the number of young people on health insurance plans.
> There's a weird narrative where any event is tied to the ACA while they ignore what the healthcare system is in the US overall.
The ACA fundamentally shifted the landscape for the whole healthcare system with minimum coverage mandates (including employer plans), guaranteed issue, etc. It's also led to higher demand for medical services (ie because more people are covered - a good thing) at a time when the number of doctors has stayed fixed. The net result is that health coverage is simply more expensive. One way that could have played out would be employers eating the higher premiums themselves (which is essentially giving everyone a raise.) Anecdotally, it seems the way it's played out is that employers have kept paying roughly the same amount while employees have either paid higher premiums or received higher deductibles.
The trend of higher and higher medical costs, employer plans trending down as far as benefits and up as far as costs was established long before the ACA.
My employers have been complaining about skyrocketing health insurance costs since my first job in 1998. This all predates the ACA by at least 20 years.
Their role is to protect against very high bill of $5,000 and up due to major surgeries, illness, pregnancy, and so on. They should definitely be completed by a health savings account (HSA) for day-to-day coverage.
That's interesting data. Thanks for sharing it. In the 2017 snapshot, I'm surprised to see that HDHP plans are slightly more common for high-income families. I didn't expect that.
There's a missing variable here: What are the premiums? HDHPs are attractive to insurers (and by extension employers) because they increase employee sensitivity to healthcare costs and may lead to less wasteful spending. Advocates emphasized that the savings on premiums could be passed on employees as HSA contributions [1]. But as that chart shows, a quarter of Americans have an HDHP without an HSA, and at every point most HDHPs haven't come with an HSA. Are employers just keeping the premium savings? Or have rising healthcare costs meant that the savings haven't materialized?
I imagine it's because it provides a way to sock away $7k each year in a retirement fund that can be invested in index funds and won't get taxed after 65 on qualified medical expenses making it more valuable than either traditional or Roth IRAs that get taxed on withdrawal and when you put the money in respectively. High-income families have the spare cash to do that, so for them it's a valuable investment vehicle.
My wife's employer covers our family under an HDHP. Our out of pocket cost is 0. Our plan requires us to have an HSA, though I don't thinkone is required to contribute to it. We contribute the max $ to our HSA each year.
A more traditional plan would run us about $4-5 thousand annually in payroll deductions. Most years we spend far less than our HSA contributions and can roll that money over year to year and even invest it. The one year she needed major surgery, we hit out OOP max and probably spent about $10,000 total from our HSA.
Probably our biggest risk exposure would be if one of us needed to take an expensive prescription since I don't think there is any annual limit on those costs.
In Northern Virginia, for example, the cheapest 2019 Obamacare individual market Silver plan for a family of four (mom and dad age-40) making a subsidy eligible $65,000 a year costs $4,514. That plan has a $6,500 deductible meaning the family would have to spend $11,014 on eligible health care costs before collecting other than nominal first dollar benefits.
I am not a fan of the word "unsustainable," but it seems to apply here.
That's not necessarily true, the discounts that insurance companies negotiate can be huge, but it's hard to include that since prices are so inflated to begin with.
At least that premium is totally reasonable. In Germany, the health insurance tax is 15%, half paid by the employer and half by the employer (and it’s not progressive like the ACA subsidy). $4,500 per year is 7% of income, lower than what the employer-side tax alone would be in Germany.
Now do the math when you include total out-of-pocket. My napkin says: "Considerably more than 15%". (Unless I misremember, and the 15% German tax doesn't cover the vast majority of cost.) Not to dismiss your point completely, but I could sell you insurance for $1/year, but your total out-of-pocket cost is going to be considerably more than $1.
The ACA barely touched employer-based insurance. It definitely did not make things "modestly worse for most people". You are blaming the ACA for problems that existed in the health care system before the law went into effect. Any degradation of care for "most people" is because of crazy year-over-year cost increases that were already happening.
And the people who had pre-existing conditions before the ACA were well and truly screwed. That didn't mean insurance was expensive for them - it meant insurers wouldn't sell them insurance at any price.
My personal anecdote: Pre-ACA, I was denied insurance by Aetna at age 35 because I had "acid reflux" and I had injured my neck in my 20s (even though I had no problems with it at the time). Then all the other insurers denied me, because the first question on any application was, have you ever been denied for health insurance? The annoying thing was the ACA had already been passed, but had not gone into effect yet - so until that happened, I guess it was just business as usual for the insurers.
My family went bankrupt because the insurance companies decided my mother having a stroke and falling down the stairs constituted a pre-existing condition.
I don't think people understand how pervasive the usage of pre-existing condition bullshit was used to deny payment.
"You didn't know you had X. It had never been diagnosed. But looking at your history, your treatment for 'unknown ailments' and such were actually symptoms of X, in other words you had X, though you didn't know it. And when you signed up for insurance, you 'failed to disclose' this condition [that you didn't know you had], therefore, we are voiding your coverage effective immediately [and should consider yourself lucky if we don't try to 'recover costs'...]".
You're right. Know why you're caveating this and tip toeing? Cuz ACA had a huge propaganda/rhetoric element to it. Even after it was an abysmal failure for most, politicians behind it kept pushing it like it was just a matter of time before it improved. It had a few good components but for the tradeoffs it wasn't worth it. (No Preexisting conditions should have always been a thing).
This is the world we live in. People have to apologize while expressing perfectly reasonable objections.
All of us with pre-existing conditions that couldn't buy insurance no matter the cost feel different of course, but you acknowledge that.
I'm interested in why you think ACA itself has made anything worse. Surely premiums have gotten worse, but it's not clear to me how it is nec linked to the ACA. (And it should be said that the insurance industry basically wrote large portions of the ACA, and arguably its weakest parts or because of that!)
ACA requires insurers to cover pre-existing conditions. That's a cost that needs to be recovered, and most of that additional coverage comes by increasing premiums. Ergo, ACA increases premiums.
That's excellent, and really contributed to your quality of life.
I on the other hand had "excellent" employer-provided healthcare. But when a routine kidney stone (my first) ended up having (pre-existing, not as a result of procedures) infection and I had three procedures for it, two in the OR, the bill ended up being the best part of $100,000, which I had to come up with co-pays and others to the tune of nearly $8,000.
For a kidney stone. Something that (touch wood) I might not have again, but could also have dozens through my life.
My sense is that your experience is becoming more and more common. As far as I can tell, co-pays, deductibles, etc have been going up dramatically over the last few years (as the original article points out.)
Not in the least. Just to name a few of the ways the ACA changed things in the right direction for most "normal" ESI:
- ACA threw out lifetime nor annual limits [0]
- Essential benefits ensuring you have a more comprehensive plan that covers actual health insurance [1]
- Ability to stay on a parent's insurance until you're 26 [2]
- For every $1.00 your insurance company takes in from premiums, $0.80 has to be spent on patient care [3]
- There's a max of a 3:1 ratio of age rating for health insurance premiums, irrespective of your health. It used to be that insurance companies would raise your premium or even cancel your policy if you got a costly disease like cancer [4].
The problem with your secular analysis is that there is not positive control for the "what if?" without these sort of policies. Most healthcare economists suspect it would have been even worse without the (somewhat modest) regulations that were imposed by the ACA. Again, this is high level policy analysis that requires dedicated study, and there's lots of evidence that the market has highly benefited consumers across most socioeconomic strata.
I agree. The pre-ACA healthcare system worked well ( maybe not great but well ) for 80% of the population and not so well for 20% of the population. We paid less premium for far less co-pay, deductible, etc overall. Feels like the ACA made things worse for the 80% in order to make things better for the 20%.
Every discussion on healthcare payment structures in this country is completely asinine.
Healthcare is best managed as a risk pool. The bigger the pool, the cheaper to be in it. The biggest risk pool is everyone. Therefore, we should put everyone in a single pool.
How we manage this is a separate discussion. Private, public, maybe a federally chartered non-profit like the Fed.
But as long as we keep ourselves fractured into thousands of different risk pools, all these discussions about deductibles and HSAs and whatnot are just chasing our own tails.
No, health insurance is best managed as a risk pool, which, as you say, should obviously be everyone.
But much of health care is not health insurance because it doesn't deal with insurable risks. Your need to get an annual physical isn't an insurable risk. Neither is a one-time appointment with a doctor to see if your headache and runny nose is just a cold or an infection that requires antibiotics. The first isn't insurable because it's a predictable recurring cost; the second isn't because it's a routine service that shouldn't be so expensive that you can't pay it out of pocket.
Health insurance should be focused on the things that are insurable risks: emergency care, hospitalization, etc. Things that aren't insurable risks, like the above, should be handled differently. But our health care system insists on treating these very different things the same, which of course is going to lead to huge inefficiencies and high costs.
I might be mistaken, but here (Germany), regular checkups are paid by the insurance on purpose.
The alternative being people not doing the checkups and thereby delaying diagnosis until treatment get‘s really expensive as things get life threatening.
In the end insurance has an interest in people taking regular checkups resulting in early (cheap) action.
It would also be pretty easy to incentivize. Have an annual physical and save $X a month on your premium. We do it for other things like smoking already. Plus many examples in the car insurance world.
While this may make sense from the perspective of why people get insurance (to mitigate a catastrophic loss), it doesn't consider the insurer's incentives. No insurance company will want to underwrite a plan that doesn't bundle routine services, since those clearly reduce risk of complications down the road. A yearly checkup is cheap compared to missing a disease and letting it get worse.
> No insurance company will want to underwrite a plan that doesn't bundle routine services, since those clearly reduce risk of complications down the road
But current plans don't require you to get routine services like an annual physical; they just cover them if you get them. That doesn't make sense if the insurer's incentives that you describe are driving the plan.
Also, these incentives don't seem to be operating in other insurance markets. For example, auto insurance doesn't cover routine maintenance like oil changes or tire rotation.
I’m sure they would require you to get routine services if they could.
Car insurance doesn’t cover routine maintenance because they also don’t cover problems that arise from not getting routine maintenance. I’d you neglect oil changes and blow up your engine, they don’t care, they don’t have to pay for it.
Maybe we should have two separate kinds of health insurance?
One for true emergencies (like car accidents), and rare life threatening diseases (like cancer before 60).
Another for routine things, but as others have said, routine things shouldn't be so expensive.
I like the idea of structuring it like a term life insurance policy. If you die, you get money, and in some policies you even get some percentage before you die to have fun.
So, if you get cancer or whatever, perhaps you'd have a pool of funds available to you to deal with the disease, and you can use that money how you want, and perhaps even keep the remainder (or a portion of it) to incentivize keeping cost down.
Also, it would make sense for the pool of funds available to someone to be based on remaining years. If you get cancer when you 20 it makes sense to spend a million dollars trying to cure that. If you're 90, maybe it makes sense to treat it but not as aggressively or in as costly of ways.
From the perspective of building a society that you would be willing to be in, assuming you were randomly born into that society without knowing to what parents, I still think many people would agree they'd rather spend heavily on younger people than older.
> Maybe we should have two separate kinds of health insurance?
I agree we should have two different types of "plans". The one for emergencies and rare conditions would be insurance. The other would not. :-)
One key objective of the "other" plan (the one that's not insurance) should be to make the actual costs of services visible to the patients, who are the ones in the best position to assess the value of those services to them. One of the biggest inefficiencies in our current system is that people get all kinds of health care services without any idea of what they actually cost. That means nobody really knows whether those services are worth what they actually cost. That's a recipe for huge inefficiency and high costs, and so it's no surprise that that's what we have.
> Another for routine things, but as others have said, routine things shouldn't be so expensive.
This is basically a subscription. But this is also how health insurance already works in part today. A certain portion of your premium is paying for routine doctor's office visits - the insurance company is basically just acting as a payment processor for this portion of your healthcare expenditure. You could separate it from health insurance, but it likely won't make a huge difference in costs or access to care.
Sorry, but annual physical exams for asymptomatic adults do not reduce mortality or morbidity and certainly do not "clearly reduce risk of complications down the road"
The idea of the "annual physical" in general is a little odd because there's no standard on what an annual physical actually entails. I've been to doctors that order every blood test under the sun and don't touch me AT ALL to doctors who order zero blood tests but feel up all my organs in detail.
you need to go to both docs apparently, or find one who does both.
So you are saying that detecting early that you have high cholesterol and treats it, or a doctor noting gastrointestinal problems and tells you to get a colonoscopy, or that you have a blood sugar problem noting early onset diabetes - none of these thing will save money long term?
Is it? Here in Hong Kong, a health checkup once a year for 10 years will cost 5000 USD, which is also comparable with the cost of treating a moderately serious disease. Checkups are very expensive, and are not even remotely guaranteed to find some critical diseases.
So I would suggest that prevention is not necessarily cheaper than the cure for insurance companies, and largely their health programs like free checkups or fitness coupons are just marketing.
Preventative measures (e.g. annual physical) can be seen as a form of insurable risk management. It's arguably much cheaper to treat something if it is discovered early on.
There's no reason to try to draw the distinction you're trying to draw. You're starting with ideology and proceeding to practice, which is a bad idea. There's a tremendous benefit to society in providing clean water, and also in providing medical care, for the same reasons.
Preventive medical care generally has a negative cost to society; treating diabetes from the beginning is cheaper than amputating limbs, transplanting kidneys, etc.
This is a very interesting perspective that I never thought of before.
>the second isn't because it's a routine service that shouldn't be so expensive that you can't pay it out of pocket.
This is a little dicey. What if my doctor thinks it’s just not a normal cold and he needs to order blood work and ct scan? And that leads to a insurable risk.
Checkups and preventative care are not there for fun. They save money as a whole and in the long run, as other commenters also note.
Imagine everyone was disincentivized from doing a cancer-related checkup, get vaccinated, or check if they have a cold, the flu, or something worse. It is better to spend x now than deal with a crisis (either individual or epidemic related) spending orders of magnitude more.
To be fair, this perspective does assume that people care about the health of society as a whole. If you're willing to let others get substandard care or even die, it may be more optimal for you to have your own smaller, lower-risk pool with better benefits.
Right. And therein lies the rub. The US is quite possibly one of the worst in the world for "Fuck you I got mine" (until you don't got yours). And then there's the cognitive dissonance of people who might have otherwise screamed about "socialized medicine" who find themselves on the unlucky end of a diagnosis and are singing a different tune (or sometimes still singing the same tune, even as they put up a GoFundMe...).
How many other countries in the world consider medical bankruptcy a thing to be accepted and tolerated?
That’s what makes me nervous about socialized medicine in the US. I’m absolutely in favor of universal coverage—a healthcare system that maximizes the health of the average productive person. But I worry that Americans lack the cold realism of Brits, and won’t be able to effectively control costs by denying cost-ineffective treatments.
Insurers deny expensive or cutting-edge treatments in the US all the time! You don't have to look hard to find sob story after sob story.
And it makes sense. If a treatment is super-expensive and unlikely to be effective anyway, and that money could be put to better use to help more other people ... It's like how someone who smokes isn't going to get a lung transplant; there's too many others that need transplants and not enough lungs to go around, so give the lungs to the people who will benefit the most from them (generally, people who are young and otherwise healthy). There aren't infinite resources in this world, so in the cases where scarcity comes into play, they should be doled out in the way that creates the greatest good.
Before Obamacare, insurance plans had lifetime limits. So even if you got a really expensive treatment approved, it would potentially push you over your lifetime limit and leave you with no coverage at all.
Yes. BUT the insurance companies knew that you had hit a lifetime limit with another company and would refuse to insure you. You couldn't jump from AETNA to BCBS to CIGNA and get a fresh million dollar limit.
Some employers put a limit on how much you pay out of pocket, even below the maximum amount of pocket required by the ACA, almost, but not quite comparable to what you get in countries with socialized medicine or health insurance systems. They essentially assure that medical treatment can't bankrupt you.
Obviously, most people in the US don't have access to such a generous plan, or the amount of medical expenses they can tolerate without going into bankruptcy is below the legal out of pocket maximum (6k/yr individual, 12k/yr family). Hence the GoFundMe pages to raise money for medical treatment.
There was a somewhat common misconception that the limit was per person, not per policy.
Although, the distinction wasn't very meaningful because you could be denied for pre-existing conditions, so if you had hit a lifetime limit on one policy, good luck being able to get another one anywhere else.
Well, that article talks about blaming Big Pharma for the costs that make it expensive, not the National Health Service.
With the big pool comes big leverage. The NHS effectively said "We're not paying that much", and the pharmaceutical companies decided they'd rather be paid something. Because if someone is not getting treatment, then they're not getting those drugs.
Medicare in the US does this. "This is what we are paying for this drug".
The issue isn't so much this. It's that drug industry lobbies in the US will have far more sway over the politics of this than they would in the UK (or Canada, or Australia, or...).
I definitely don't claim to be an expert on these things. But I have lived in the UK with the NHS, in Australia with its medical system, and now in the US. In addition to that, I've worked as a healthcare provider, and for a Health Benefits Management software company, so I'd at least like to think I have something of a varied perspective.
Medicare in the US does this. "This is what we are paying for this drug".
That is definitely not true. Part of the prescription drug coverage that was added during the Bush administration was that Medicare could not negotiate drug prices.
The very first part of the article explains how the NHS denied coverage for certain breast cancer drugs because it was too expensive. My concern is that the Americans won’t be willing to do that. Here, you see all these articles talking about how terrible it is that families went bankrupt going out of pocket after they hit a $1 million cap. The UK wouldn’t have paid for that treatment in the first place.
> Her family said an antibiotic Lucas needed to treat her symptoms cost about $2,000 and her insurance company denied coverage of the medicine, leading her to take a less-effective drug. Lucas, who was allergic to multiple drugs and antibiotics, had a reaction to that medication, Lee Lucas said.
It's weird you think that insurance means they don't deny care, I worked on systems back in the 90s in the US that was focused around rationing. The source of the money is irrelevant since ultimately you have to cap spending somewhere as it's not limitless. The NHS generally does a great job in getting bang for the buck, in fact in terms of treatment effectiveness and longevity it's considered the best in the world.
This is solvable. Rather than just "deny" treatments, the insurer (public or private) can just pay the customary amount for treating the given disease. The rest is the patient's responsibility.
So rich people can still get the latest $500K insta-cure prostate cancer treatment (and they are paying out of pocket for most of it), and the rest of us make do with surgery/radiation.
I have a feeling that without the US market capable of paying a hundred thousand dollars a patient, many of those cost-ineffective treatments never get developed. People could still pay for them out of pocket, but without the guarantee of insurance payments the drug companies likely won’t take the risk.
And I don’t think that’s necessarily a bad thing — if a drug costs $500,000 and keeps my cancer at bay for 6 more months, it provides a high personal benefit from my selfish point of view; but at a high cost to society without much societal benefit. I think you’re right that Americans do lack the realism, but it may become easier if those treatments aren’t developed in the first place.
> People could still pay for them out of pocket, but without the guarantee of insurance payments the drug companies likely won’t take the risk.
this, in my opinion, points out a significant flaw in the rush to privatize just about everything:
there are many many “markets” that are either under-served or not served at all because the rate of profit would be (a) too low to “justify” or (b)none at all.
jmo but, there has to be a balance between for-profit and basic research that won’t necessarily be able to be monetized to the extent many in industry would want...
I’m not necessarily against a for-profit pharmaceutical industry... but I certainly am when the entire cost burden falls on us because the pharmaceutical companies band together to prevent our government from negotiating drug prices at the national level like pretty much every other wealthy nation...
> but at a high cost to society without much societal benefit.
People are employed and knowledge is gained. That may be $500,000 treatment for 6 months now, but that treatment may be improved and democratized until it evolves into something that is $50,000 for 6 years.
A citizen science model — which is what we de-facto have for anything that isn’t cancer — is more efficient and cost effective.
As it is, if someone finds a new life-saving use for an 80 year old drug, there are suddenly shortages of the old drug while a new, patented analog is sent through clinical trials. See also ketamine and depression.
Private insurance companies do this every single day. So you're worried that the government might do what insurance companies are guaranteed to do. At least the government wouldn't have the profit motive that drives insurance companies to these measures that literally kill people. Your argument is completely out of touch with reality.
> Healthcare is best managed as a risk pool. The bigger the pool, the cheaper to be in it. The biggest risk pool is everyone. Therefore, we should put everyone in a single pool.
No, whether or not expanding the pool raises costs depends on the cost of the added population. If 80% of the population is insured, and they consume an average of $1,000 in healthcare costs each year and the uninsured population consumes $10,000/yr then expanding the risk pool to the entire population will increase the cost of insurance. We saw this happen firsthand when we mandated that insurers take on all patients at the same cost regardless of prior conditions. The population that was added to the risk pool was more expensive than average, thus driving up the cost charged per person.
Universal healthcare isn't a magic wand that makes healthcare costs go down, these plans are affordable for the average person because they are paid for by taxes which are levied at different rates depending on income. I many of these countries if you charged the cost of healthcare per person on people's post-tax income (and adding back in the tax paid for healthcare) they would be paying a greater portion of their paycheck for healthcare than most Americans. The affordability isn't solved by dumping everyone into one risk pool, it's solved by changing the way healthcare is paid for. Furthermore, most universal healthcare implementations don't put everyone in the same risk pool they tax and give citizens funds to spend on healthcare but the risk pools themselves are managed by insurance companies.
Healthcare in the states is asinine, no doubt. But when I see articles like this I have to ask, "why aren't these people making 75-100k using HSAs and FSAs"? They would eliminate many of these scenarios that people are seeing.
There's the elephant in the room that many people are absolutely terrible with money, buying entertainment goods and completely skipping on savings, HSAs, etc that could prevent these media sob stories.
Why should we, the conscientious readers, trust your claim that you know what's best? Cuz it sounds like something that sounds good but which has no verifiable backing.
If you were designing a society starting from scratch today and said, "I think we should make having health insurance largely dependent on having an employer.", you would be laughed out of the room.
I think we are running along some tracks that were laid long ago, and rather than all jumping off, some people in comfy Pullman cars are content with letting the train run off a cliff.
Employer-provided healthcare is an aberration created by government interference in the market.
> Employer-provided health insurance has its origin in a tax policy passed in 1943, which made insurance provided by employers tax free. At the time the United States was engaged in World War II and had enacted wage and price controls, preventing employers from competing for scarce labor using the normal mechanism of offering a higher salary. Instead, businesses used the availability of newly tax-subsidized healthcare as a means of differentiating themselves.
> The tax advantages were made even more attractive and fully codified in the 1954 Internal Revenue Code. Over the next few decades, the government's subsidization of employer-provided health insurance lead to the dominance of that model of healthcare delivery...[1]
So steps that got us here:
1. Enter into WWII
2. Enact price & wage controls
3. Create tax loophole for employer-provided plans
4. Enshrine loophole into the tax code
These are not market phenomena, since government intervention got us here.
It's dumb that we're here, but knowing the history suggests a possible solution.
What if the government was able to pass legislation banning employer healthcare? I imagine the issue of healthcare coverage would resolve very shortly thereafter.
I find it odd that some executive gets to pick which 401k and health insurance plans you get, and that you must pick from their few choices that allow you to have. I can see why the providers love it, they can target all their advertising, marketing, etc, at a few key people at large employers, but not sure how that benefits the average worker..
You can get an individual 401K or IRA and make all your own choices. If you're talking about an employer matched 401K, I don't think it's unreasonable at all for them to select it.
> If you're talking about an employer matched 401K, I don't think it's unreasonable at all for them to select it.
What's special about 401k matching that requires the employer to choose plans? My employer doesn't force me to have a checking account with a particular bank they chose if I want to receive my salary. They should be able to match contributions to any account anywhere.
I don’t know if you understand how 401K matching works on the backend.
A lot of times the employers are capped on their own plans at a percentage rate that matches their employee’s participating. So matching is often in their best interest, esp at smaller companies.
But, easier version is this is a perk, not your base salary. They are paying you with legal tender and there are freedoms associated to that. There is no such thing for perks.
You aren’t entitled to make the administration choices for something they are gifting you.
> I don’t know if you understand how 401K matching works on the backend. A lot of times the employers are capped on their own plans at a percentage rate that matches their employee’s participating.
I actually do not understand this. Could you please explain more? What does an employer being "capped on their own plans" mean?
> But, easier version is this is a perk, not your base salary
When I make a decision on a job offer, the 401k match, health insurance premium, free lunch and snacks etc. all factor in and they're all worth a certain amount of money. Money is money and how it's labeled, "perk" or "base", is irrelevant. If my employer ends 401k matching, I'll treat it as a pay cut mentally.
My ultimate "fantasy" is to eliminate 401k altogether and instead let everyone contribute whatever the 401k annual limit is to an IRA. The employer can simply add matching funds to your IRA and you're free to have your retirement accounts anywhere you please.
There are no "free perks" in employment contracts. These are money equivalents, just like RSUs, free lunches, and other benefits. I make employment contract decisions based on these benefits. If my employer materially alters these benefits I would change my place of employment, just as if they lowered my base salary.
If I was designing a society from scratch, I don't think I would create "insurance" that is expected to pay for almost every routine, non-emergency, completely predictable cost just because it's a medical cost.
The employer-provided system--which arose out of WWII-era wage controls, for those who don't know--has not only created the "have/have not" dichotomy in U.S. healthcare, it has also warped expectations about what "insurance" is supposed to cover--and broken normal pricing mechanisms.
I happen to agree that the system is broken and getting worse, but that's not necessarily a good metric for whether you should change any given system now.
Individualism in America is the main cause... if you just got taxed and didn't have to worry about healthcare, people wouldn't care, but they all think that it could never happen to them.
Americans think the poor are slackers and they don't deserve anything. Even poor Americans think the "other" poor are slackers and don't deserve anything. Nothing will change until you change this mindset.
High-deductible health plans were always designed to benefit employers. My company switched us to one with a big PR campaign highlighting how everything would be better (contributions to HSA - free money!). The only "advantage" is that companies have to pay smaller premiums and employees are greatly discouraged from getting care due to high costs.
> The only "advantage" is that companies have to pay smaller premiums and employees are greatly discouraged from getting care due to high costs.
In principle the advantage is that employees are greatly discouraged from paying too much for care. If the insurance pays for everything then what do you care if your doctor is charging $1000 for a physical instead of $50? If you're paying out of pocket, now you care.
The problem is we also have a lack of price transparency, so it's arduous to actually determine the price you'll be charged for routine care and avoid the places who are overcharging, which correspondingly becomes nearly everyone. The states would do everyone a favor to pass and enforce some price transparency laws.
And the advantage of lower premiums is that it allows you to receive that money. If your employer is raising your plan's deductible and giving the balance saved in premiums to you, that's the advantage -- you get the money. If they're not, go ask for a raise or find another employer who will pay you more, in the same way you would if they lowered your compensation in any other way.
And even list prices themselves are typically starting points for negotiations when a provider is dealing with a large payor whereas an unwell individual (y'know, one who is about to spend a lot of money on healthcare) is not in a great position to bargain with her caregivers, and so is forced to negotiate after the fact, from an artificially inflated starting point, under the guise of bill reduction, or worse, debt relief.
A lot of the issues with pushing price negotiation to the individual also seem to be assuming (or worse, lying about) that most medical professionals, procedures, facilities, et al are entirely fungible. Even if individuals had full price transparency, that doesn't change the fact that certain facilities will always be closer to home, certain procedures inescapable, certain medical professionals decades or life-long relationships to build, etc. Medical services aren't just interchangeable factory goods on a retail store shelf that you can easily pick based on price alone and then slot it right into its widget shaped hole, and never will be.
> Medical services aren't just interchangeable factory goods on a retail store shelf that you can easily pick based on price alone and then slot it right into its widget shaped hole, and never will be.
Almost nothing actually works that way. Walmart doesn't stock exactly the same goods as Target. One of them may be closer to where you live than the other.
Which is why price isn't the only criteria. If the office closest to your home charges $250 and one which is fifty miles away charges $200, you can perfectly well choose to pay the extra $50 for the convenience.
The issue is that when the nearest office decides to charge $1000 and the one fifty miles away is still charging $200, that should maybe change the outcome. But not if you aren't aware of the price difference to begin with.
And this even applies to the beloved family doctor -- there is a limit to the amount of price gouging that a familiar face is worth.
That is one of the major ways prices get to something reasonable. Once you have people taking cost into consideration when choosing a provider, it becomes a competitive advantage to have a lower price in a way that it hasn't previously.
Obviously you have to execute this well and without the rules getting corrupted by inefficient businesses that want to keep their margins, but "rules are not corrupt" is the sine qua non of reducing prices regardless of which specific mechanism you use.
One way to fix that central problem is to decentralize it. Eliminate the federal rules to be replaced with state and local rules. Then you may get one city or state screwing things up, but it at least puts the upper limit on how expensive things can get there at the cost of traveling to a different place with different rules and lower costs, and the travel cost is naturally lower between cities or states than between countries. (And having the option to do that generally prevents you from having to actually do it, because the local providers still want your business more than they want the higher margins.)
401k are tied to employers, but I don’t see what HSA has to do with employers since they’re just as easy to have without an employer. It’s just a savings account with tax advantages for people with HDHP.
Yes however it is definitely a way for employers to save a bunch of money while convincing employees that they are better off too. The whole smokescreen of we will give you a bunch of money "for free!" that goes to your HSA and somehow that is better value for you than a traditional PPO. In much the same way that 401k contributions are better than a pension.
401k are better than defined benefit pensions. I want control of my money, why would I trust a random pension board of trustees? And even though 401k isn’t really under my control, I trust an index fund more than an opaque board of trustees doing god knows what with the funding.
The only defined benefit pension that is doing okay is taxpayer funded pensions, and that is only because government has the power to tax. And even then some have been cut and some states are seeing economic decline because of them.
Edit: In fact, the employer's HSA custodian (unless it's Fidelity), probably charges you a few basis points for investing your HSA funds, so it's actually much better for you to transfer the funds out into your own Fidelity HSA immediately.
If you spend a lot on healthcare (i.e. have a family) then a HSA works fine since you hit your maximums really quick and then only pay some small % of the sticker price after that.
For everyone who isn't gonna spend a few grand in healthcare every year it totally sucks and is a massive incentive not to have routine care done.
That doesn’t make sense. If you spend a lot on healthcare, then why would you want to spend it out of pocket from HSA instead of letting insurer pick it up with a non HDHP?
Healthcare costs whatever it costs, no matter what the premium / deductible is. The more of it that is used, the more someone has to pay, and you can be sure the insurance company is going to adjust the premiums or deductible or coinsurance/copay to make sure it's not them (in the long run).
The HSA/HDHP option just lets you gamble that you won't need enough medical care in the year to offset the investment and tax gains of contributing to an HSA. And if you're lucky, you'll make it all the way to Medicare eligibility. Although I'm pretty sure we'll see Medicare start being means tested in the next decade.
Regardless of whether it benefits employers, it makes sense for healthy young people, no? If your health care spending is low, you get free money every paycheck. Also last time I looked at my HSA account, it's both pre-tax contribution and tax-free growth. So you get double tax break.
Healthcare simply does not line up with the incentive structure of the free market.
People can't opt-out if they're getting a bad deal.
Risk outliers get turned down as bad business decisions, or the drugs they need to stay alive are impossible to afford because of "low" demand.
It's left up to employers to choose the product that's best for their employees (and ensure that market competition functions), but that assumes they actually care about their employees' well-being, which most don't.
Denying care to the unemployed is a strong force deepening the poverty cycle, preventing people from working their way back up to being productive members of society.
Healthcare doesn't even really fit the model of insurance, because it isn't just a guard against unlikely catastrophe, it's an ongoing, chronic, inevitable cost of being a human being.
Yet here we are. Remember when Obama fought to have healthcare prices made transparent so that we could shop for the cheapest medical treatment, and that was beaten back severely by the lobby? The compromises the ACA made to bend over backward for for-profit insurance companies were an example of how much power the lobby has. I think if we've learned anything is that we need to go all in on single payer and completely remove for-profit insurance, IMHO, because of exactly what you're saying about the free market: it doesn't work for certain things (if anything, really): military, education, healthcare all the three classic failures of the freemarket. I think this is why all the dems are embracing Healthcare for All: everyone is getting screwed by healthcare except the 1%.
I think the free market does a good job of solving problems, just not of deciding which ones are worth solving. The military follows a hybrid model that (mostly) works, where a semi-free market is created and guided exclusively through governmental leverage, theoretically giving the best of both worlds. Utility companies work a similar way, as do (I think) some first-world government-run healthcare systems. I think the ACA was aiming for this type of thing, but was so hamstrung by compromises and by the sheer complexity of the system it was trying to reshape, that it ended up being a pretty mixed bag.
Maybe in the case of American healthcare, the current state of things is just such a horrible rat's nest of problems that we really do need to burn it all down and start over.
The insurance companies and the AMA were vehemently against Medicare when it was initially proposed. They fight for it now. Given all of the established interests in the medical system, and the amount of money flowing around, any reform that is actually going to make a major difference is going to be one that they strenuously oppose.
Isn't the point of an HDHP that you're supposed to set up an HSA to go with it? Premiums for HDHPs are significantly lower than for normal health plans; the idea is that you're supposed to use the premium savings to fund the HSA, which is then money that carries over year over year, right?
I think the value of this really depends on the employer. At a previous role they started switching to an HDHP with an HSA and did a great job (initially) making that fairly attractive versus the low deductible plan with higher premiums.
At my current employer, the deductible per person is close to $4000 and the family limit is ~$10K. The employer provides some money if you have an HRA, but very little if you take the HSA. The premium savings from the low deductible plan (which isn't available any longer) really doesn't make up for the higher deductibles. All it takes is one small series of events (e.g. a complicated pregnancy) for $10K to go out the window. If these series of events happens from December - January, that's 2 years of deductibles out of your pocket.
I work for a huge company and I'm surprised the insurance is so expensive. For the first time in my life I think one of major criteria of my next job will be the healthcare benefits. Previously I was just happy to have insurance - no longer.
Same, Work switched to HSA medical. Pre-ACA single employee had basically medical paid by work, Post-ACA, they moved to an HSA (almost mandatory I guess) that work kicks in money per paycheck. BUT, now I have to match the minimum and have a high 8k deductible. So everyone just took a pay cut post-ACA, and if we use the medical, we even pay more. No more co-pays, I have to pay full price doctors visits.
Its easier for me to go to urgent care, say I dont have medical insurance, so I get a cheaper uninsured rate, then submit my medical care expense to my HSA for reimbursements, then if I hit the yearly deductible, claim I have insurance.
Something that really frustrates me about my current HDHP/HRA plan is that it feels like it only makes sense if somebody in the family has a minor issue(e.g. the flu) that is covered by the few hundred dollars the employer puts in the HRA, or if somebody has a major medical issue that would have destroyed our savings.
Between those two extremes, the value of having insurance is just all the mysterious insurance "adjustments" on every medical bill. As you pointed out, there are probably lots of situations where saying I have no insurance makes more sense from a financial standpoint.
Yes, one of the benefits of a HDHP is that you can use an HSA which can help since pre-tax dollars can be put directly into an HSA by your employer either as a part of your compensation package or as deductions from your paycheck (you can also make deposits with post-tax dollars and deduct them at tax time but you don't get the FICA taxes back then). Many company provided HDHP don't have THAT low of premiums and the tax savings for many middle class families is minimal due to an HSA due to the recent tax reforms providing a $2k per child tax credit.
For example, I enroll my family in my employer's HDHP. The total premiums from our plan is about $19k this year (employer pays about $14k, I pay about $5k). For this, we have $4k deductible and an $8k max out of pocket coverage. Once we hit the deductible then insurance covers 80% of the cost of most things until we hit our max out of pocket and then they cover 100% of most things, in-network. The most I can put into my HSA is $7k per year.
For about $19k/year in the NY state run insurance marketplace I could buy a HDHP with a $2k deductible and $5k max out of pocket. For $24k/year I could buy a plan that has a $35 copay for pretty much everything. My employer's plan isn't any better than what I could buy on the open market but it IS better for me because I only have to pay a fraction of the premiums.
> For example, I enroll my family in my employer's HDHP. The total premiums from our plan is about $19k this year (employer pays about $14k, I pay about $5k). For this, we have $4k deductible and an $8k max out of pocket coverage.
Posts like this really emphasize to me how broken healthcare in America is. This is a fairly standard setup and yet you're paying $23,000 per year before you get anything from your insurance other than price negotiation. The median annual personal income in the USA is $31,000.
Regarding price negotiation, my wife and I have asked multiple doctors, nurses, and billing departments to tell us how much a given service we have received will cost. Both before the service and after the service. We've even called the insurance company with the billing codes from the doctor's office to get quotes.
NO HUMANS CAN TELL US HOW MUCH ANYTHING COSTS!
We are continually told that we have to wait for the insurance company to come back with the pricing after the service has been rendered. This is the most infuriating part of it, there is no way for us to understand the costs of services which are recommended to us by our doctors. We are not able to shop around or to understand if we could/should delay any particular service because of cost/benefit ratio because we do not know the cost of anything ahead of time.
At least our preferred local pharmacy will usually call us prior to filling any expensive prescriptions to make sure that we understand the cost. I assume the pharmacy has enough people balk at the cost after they've already filled the prescription and then they have a bunch of headache dealing with putting the pills back so they've gotten proactive about it.
When I was shopping around I was told by hospital rep, that they can't tell me the price, because of a) they don't know until they talk to insurance company, b) EMTALA prohibits that.
I had to negotiate an emergency CAT scan for my daughter about 8 years ago, and they ultimately had to make up a price on the spot for me ($1000).
Lack of price transparency is an enormous problem with our current system. Of course, it's a problem on the provider side of the system, not the payer side, which is where everyone spends all their attention.
There's also a weird income range where in effect the government funds the HSA.
For example, in my state for someone of my age, someone making just enough to not qualify for expanded medicaid gets a subsidy of $1000/month. As income rises to 400% of the poverty level, the subsidy amount drops to $660/month. The subsidy drops to $0 if the income rises above that.
Since an HSA contribution, like a 401k or IRA contribution, comes before taxes, it lowers the income used for ACA subsidy calculations.
The result is that if your income, after 401k or IRA contributions, is such that you do not qualify for an ACA subsidy, but you missed qualification by less than the HSA contribution limit ($3500 in 2019, $4500 if you are 55+), then if you go with an HSA plan and contribute enough to get under the subsidy limit, the subsidy that will get may be more than your HSA costs. Whether or not it will be depends on your age, and how much over the cutoff you were.
It's a ridiculous situation.
Even more ridiculous, the way the subsidy goes from several hundred to nothing as you cross the cutoff means that there are people who are better off taking a pay cut to get into subsidy territory. I know someone who by putting the maximum into his retirement accounts and his HSA was able to just get into subsidy territory, but is now going to have to watch carefully near the end of the year to make sure dividend income from investments doesn't push him over. If there is any danger of that, he might have to go on unpaid leave for a while from work.
I'm self-employed, so I get insurance through the marketplace. The plans that qualify for use with an HSA are more expensive than plans that are not legally HDHPs, but just happen to have a $6000 deductible and $7900 max out of pocket. They are so much more expensive, in fact, that they completely negate the tax advantages (which are significant.) As a result, I contribute to a basic savings account instead of an HSA, but I could see many people hoping for the best and not saving at all.
This has been my experience, too. I've been self-employed since 2004 and had an HDHP w/ an HSA prior to the ACA. The premiums from 2004 to 2014 were lower than equivalent non-HDHP's, but post-ACA (we dumped our pre-ACA plan because I had a pre-existing condition that was not covered in our pre-ACA plan) we've seen equal or high premiums for HSA-capable HDHP's to non-HSA-capable plans.
The point was that the premium was lower so you could save the difference and instead of that difference going to waste each year, it could compound over time.
I mean, if a HDHP plan costs 400 / mo and a regular plan costs 1000 / mo, you get to save the 600 and let that compound over many years (if you don't use it), rather than lose the 600 in insurance premiums.
tathougies was referring to the difference in monthly health insurance premiums. I don't see what their comment has to do with Flexible Savings Accounts.
From what I understand, even the HDHPs have such high premiums that the point is not being achieved, especially if you have to go through the marketplace rather than the employer.
Due to rising healthcare costs, and employers reducing the portion of health insurance premiums that they want to pay for their employee (aka a paycut), that's going to be true regardless of HDHP or not HDHP.
There is no requirement for your employer to provide the HSA. Frequently the employer can get better deals on the HSA than you can individually (like no waived maintenance fees and the like) but you can for sure open your own.
In fact once you have enough money in there that you are moving out of liquid investments then you definitely want to shop around for HSA much like you would for an investment account.
Can you actually fund a non-employer HSA with tax-deductible funds, or is that a benefit that only applies to payroll HSA contributions? If not, a lot of the benefit of an employer HSA disappears.
(FWIW, I have an HDHP, employer HSA, and an individual HSA that I roll my employer funds to annually for lower-fee investing.)
Only partially. If you fund your HSA outside of your company's payroll system you can deduct your contribution amount from your MAGI for income tax purposes, but you still have to pay FICA taxes (social security and medicare) on that income.
If you have your HSA contributions made through your company's payroll department, then you don't have to pay FICA taxes on it.
HSA Authority (part of Old National Bank). Last time I ran the numbers, the break-even point on annual expenses vs some other options was about $10k in HSA balance — where smaller balances would pay more at HSAA than some other provider(s). But they cost less than other providers for larger balances (again, last time I checked).
Yes you can, go to Fidelity and sign up for one. Takes like 10 minutes. Transfer money, buy a fund, away you go. Just like an IRA, except never taxed at any point. Besides employer matching it's the best freaking retirement deal there is.
Example
HDHP plan where you pay $30 every month
Full price at doctors, deductible of 5k (80/20 after), max out of pocket 10k
Setup HSA to contribute $200 every month (tax benefit)
If you go to doctor 2-4 times a year for minor stuff it works out great for you.
If you use if for 4-5 years, savings add up and have some security in the future towards medical related costs.
Does not seem to work great for families with kids or someone who frequently visit the doctors, for young singles with no health issues it can work out great.
If it's an employer-provided plan, though, you don't generally see the premium savings. My employer provides the option (through one of the major payroll/HR providers) of a "regular" plan or a high-deductible plan, but neither choice affects my take-home pay. I still chose the HDHP though because I'm generally healthy and it lets you invest pre-tax money with no capital gains tax, which is nice.
Ok, so then, the nut of this story is that employers are adopting HDHPs as a way of reducing their own costs, but not passing the savings to employees, which defeats the purpose of HDHPs and just amounts to screwing employees over?
Or employers can reduce pay raises. Or cut pay. Or do any number of things to hit whatever net income targets. Ideally, we wouldn’t have employers involved in all this price obfuscation, and it would be easy for employees to compare compensation.
I'm not sure - since I have either option, I don't feel screwed over, but if an HDHP were the only option I would definitely expect to see an increase in take-home pay.
In a decade of employment I've not had an employer offer a plan that wasn't an HDHP. It seems to be somewhat regional, but in my part of the country the last plans that weren't HDHPs were phased out in the late 2000s and seem unlikely to ever return.
I think yes that is an effective strategy, especially given the economic incentives to having a HSA and how it is possible the manage the money in the account. However, the economically “supposed to” decision for the monetary difference is now up to the insured who may not understand nor desire to put some of that difference towards the same health causes rather than change spending habits. Awareness is important here.
I really like the idea of high deductible plans. The idea for me is that insurance shouldn't cover regular costs that most people pay every year. Insurance should just be for unusual events, like car insurance is only used if you have an accident.
So now I got a $2k bill from ER for something that wasn't really an emergency. It makes me think carefully about next time this happens where before the cost didn't really affect me. Changing people's behavior is important part of reducing costs of the health care industry.
EDIT: Yes I'm not happy with how expensive prices are now. That is the problem that HD plans have.
I'd like to know if there's any empiric data on how many people go to the ER for something that "wasn't really an emergency."
Then I'd like to know how many people have died because they didn't go to the ER for something that really was an emergency.
My guess would be that the latter greatly outweighs the former. And I'd follow up that guess with a wager that a large percentage of those people failed to go to the ER because they were worried about the cost.
If that's the kind of decision that high-deductible health care encourages, I don't think it's worth it.
Encouraged in part by a system where finding "Urgent Care" outside of 9-5 Monday to Friday can be very difficult to impossible in many locations.
Only thing worse is dentistry. Following a bad toothache, I walked through the directory. Not a single dentist in my entire County (quarter of a million people) was open on a Friday, let alone the weekend.
The fundamental problem is when you cover emergency care but not preventative care, you get more emergency care.
Because emergency care is more expensive, this is worse for everybody in the long run, except for profitable hospitals and insurance companies who enjoy the increased revenues.
This is only a problem if preventative care is expensive to begin with...
In India, a visit to the doctor for a general checkup can cost anywhere between Rs. 100-1000 out of pocket, with no insurance whatsoever. For reference, this is basically the price of a movie ticket.
What if preventative care cost $15-30 a pop out of pocket?
Whenever people ask me what's the biggest difference about living in the US vs. where I'm from, I always say the same thing: "People have to think twice before going to the doctor". It's just so damn weird. I think it's the equivalent of being a woman in Saudi Arabia and having to ask your husband's permission before going outside. Both scenarios can result in your life being completely ruined.
I like it too, except that my (bronze level in the marketplace) high deductible plan is ~$1300 a month for my family, that is not sustainable. A recent ER visit with 1 night stay cost us about 8k out of pocket, the family deductible for the plan is $13k a year.
Be glad that "recent" wasn't in December, prior to the deductible reset.
Fun fact - my company (who sells Health Benefits Management software) added functionality so an insurer could do a "rolling window" for deductible / out of pocket management, i.e. "In any given 12 month period, your costs will not exceed $x" (where given unfortunate timing, your out of pocket could actually be 2x).
Except it was less profitable to the insurers, so no-one was interested. But spun as "will be too complicated for consumers".
Ok, but what if your doctor says you need an MR enterography because there is something really suspicious going on in your stomach? The problem is many people just say, "that's all out of my deductible. I'll take my chances."
I seem to be the only one that thinks this way, but I view health insurance as a plan to cover catastrophic events. I view it kind of like auto insurance. I don't use auto insurance to get my oil changed or to replace the wipers or to add a rack to the roof.
So the high deductible plan I get at work is perfect for me because it has a high deductible, yes, but it has a lower overall ceiling. Meaning that if I get in an accident or I come down with a disease I won't go bankrupt because after a certain value things are covered 100%.
I do use the HSA, since my employer basically puts money in my savings account if I agree to put so much into it. So it's both an incentive to save and free money at the same time. I do use it on tests and appointments occasionally, but I often go a year or more without touching it.
Of course, I have the luxury of doing this because I don't have a chronic disease and don't have dependents to worry about. I understand that.
Agreed, the main wrinkle is that buying auto parts is a simple transaction. With my HD plan the provider still bills insurance first who negotiates a rate then sends me the bill which is hugely inefficient.
In theory, I think it's true that healthcare costs are high because most people aren't paying them, their insurance companies are. And then the insurance companies just turn around and charge more, so they aren't really (enough) incentivized to lower costs either.
In practice, the current system screws a lot of people at the bottom. We live in a world where by-and-large, the people with the most clout are also the most likely to have better insurance with lower deductibles. If you work at Google, McKinsey or JP Morgan, you probably have the option to get a low-deductible plan with 80%-100% of premiums covered. Work at Walmart? Your lowest deductible for a family is $3,500 with an annual out-of-pocket maximum of $13,700 [0]. And Walmart actually has better insurance than many low-paying companies, presumably because they are a behemoth with a lot of negotiating leverage.
> So now I got a $2k bill from ER for something that wasn't really an emergency. It makes me think carefully about next time this happens where before the cost didn't really affect me. Changing people's behavior is important part of reducing costs of the health care industry.
Yeah, but there are two big issues here:
1) Sure, it prevents some people from going in when something isn't really an emergency. But it also prevents people from going in when something really is an emergency. I recently heard a story of a poor family whose toddler accidentally drank something poisonous. They knew that they couldn't afford to go to the ER, so they drove to it and waited outside to monitor the kid and see if she started having seizures or other side effects from the poison. She luckily ended up being okay, but that's a horrible decision to have to make. I'm personally very lucky to be in a financial situation where a few thousand dollars is significant to me, but not significant enough to take chances with my child's health.
2) Why is that bill $2K in the first place? I once had some chest pain and went to the ER. They took an EKG, everything was fine and they discharged me. Bill was a few thousand bucks. EKG machines are ubiquitous, not very costly to purchase (given how much they are used) and the test takes less than 10 minutes to administer and look at. In almost any other developing country, they'd be able to do exactly the same set of tests for a few hundred dollars, insurance or not.
It's because there's nothing to gain by lowering costs.
If you get a bill from a ER for $36 dollars, you'd be less likely to buy a $200 insurance plan, so we have to make ERs as expensive as possible so we can guarantee customers for the poor insurance companies. They won't pay that full 2K anyways.
Funny story about that. This was prior to the ACA but the issue remains particularly salient.
When my mother had her stroke, there were major concerns about the cost of going to the ER. We at the time didn't know she was having a stroke and so my parents put it off.
If you're at all familiar with how strokes work this is the worst thing you can do. The sooner you get the victim to a hospital, the better chances of recovery. She was lucky to survive because we did eventually go to the ER, but she suffered from partial paralysis of her body as well as massive brain damage. She's struggled a lot with mood disorders and has trouble doing some mental tasks.
So put yourself in this situation. Are you prepared for potentially permanent mental and physical impairment because you were afraid of going to the hospital? My family ended up bankrupt anyways because this was prior to the ACA, but if we had gone sooner things would've been vastly different.
Insurance is not suited for health care. It's suited for emergencies. Sometimes health care is that, although preferably not often, and less often if proper care is given when due.
But general health care—the practice of keeping people healthy, rather than fixing them when ill—is not suited to the insurance model, and the insurance industry is too powerful to let control who gets which treatment.
A proper model pays the actual healthcare provider to keep you healthy on the regular, and then it costs you nothing in the event of sickness or emergency (like you need more stress at that moment).
The very idea of mutual indemnity is out the window with modern insurance, it's all about squeezing stats for margins, at which point there is not real mutuality, only competing risk profiles. Of course, a group of people might want to pool for emergencies, or even general health, but is there any benefit to the current scale of insurers? It only makes them more powerful.
I wholeheartedly agree. That and employer-based access to health insurance. Imagine if you had to change auto/life/home/rental insurance every time you changed jobs.
I have a HDHP with an HSA. When my company first rolled it out I barely gave it a glance (why would anyone want a high deductible?) and stayed on the low deductible plan. However, the next year I looked at it closer. I ran the numbers and realized that I could have x dollars come out of my paycheck to the insurance company under the low deductible plan, or I could have y dollars go to the insurance company and z dollars go into my HSA. And y + z = x (within a $100 or so).
So I could give all the money to the insurance company and that money would disappear at the end of the year, or I could give a portion of the money to my own HSA and I would get to keep any leftover at the end of the year. Well, now I had instant regret that I didn't sign up the first year.
The first year was rather rough because we had to pay all health care expenses out of pocket until we met the deductible, but we couldn't reimburse ourselves out of the HSA until the money was in the HSA. But, we met the deductible by April and after that our health care costs were equivalent to what they would have been under the low deductible plan.
By the end of the year we had $4000 left in the account which we then used to pay health care costs in the new year until the deductible was met. Now our HSA is growing year over year.
I have not seen mental health mentioned here yet as a factor in rising healthcare costs. My HSA/HD Plan has almost ZERO mental health doctors in network. Providers have been fleeing in droves (especially from UHC) because the insurance companies continue to lower payouts.
I went from spending a co-pay for mental health care for 3 of my kids to paying out of pocket until I reach my out-of-network deductible, which I never do because it's 10K. I spend thousands of dollars per year on this and there is not much I can do about it.
In some cases I've reduced frequencies of visits but the value of these types of doctors cannot be overstated in some cases. I credit my son's psychologist for his ability to function in society today. But she told me she can't take UHC because after costs she was making 10/hour.
Lack of in-network mental health coverage is a huge travesty.
By all accounts we have a good PPO available but this is exactly why I haven't even evaluated leaving Kaiser's HMO. Not that I don't like them. It does have positives and negatives but I've been happy so far. I just can't even consider it.
I've been trying for a while to figure out what would be a good metric to judge the ACA by. Most of the time it's success is talked about in terms of number of people insured, but that doesn't really capture how well insured they are. Life expectancy seems to be the only well known (at least to me) stat that begins to capture the health of the nation. We've now had 3 straight years of declining life expectancy in the US [0], a single year is virtually unheard of in developed nations. Now there are lots of confounding variables, and it's certainly not possible to say the ACA is the cause. And 3 years of downward trend, isn't historically unprecedented. However, it certainly makes it hard to paint the ACA as a success, I'd want to see some compelling evidence that the ACA had made America healthier, which doesn't exist right now. The question to me is how long we can accept a downward life expectancy trend before we start looking at the ACA as a potential cause.
I hate on the ACA as much as the next guy, but the article you linked blames drug overdoses and suicides. For that I would blame the for-profit health care system pushing opioids and the (Great Recession + inadequacy of our mental health care system). To blame that on a law that sought to eliminate preexisting conditions and to establish a baseline as to what a health insurance plan ought to provide seems like a stretch. Having a free yearly physical isn't going to help your crushing depression and economic anxieties.
I was just linking that as a reference for the declining life expectancy. I don't think they even come close to establishing opioid and suicide deaths as the cause, that's just journalistic conjecture. If you look at the number of opioid and suicide related deaths it's very small compared to the total population of the US, so the math just doesn't seem to work out for me. I remember an HN comment a while ago that worked out how many deaths you'd need from those causes to lower the life expectancy as much as we're seeing and it was a lot higher than what we're seeing now. Unfortunately I can't seem to unearth the comment.
Apropos of anything else, as of 2019, you are more likely to die of an opiate overdose (accidental or deliberate) than you are in an MVA. That's staggering.
Of course, not unexpected in a country that has 3% of the world populace but 81% of the world's opiate use.
A good metric is - did it do what it was designed to do? I think the answer is yes. It was designed to be an unsustainable failure, in order to trick people into thinking single-payer was the next best thing. In that regard, it has been a resounding success.
For those of us who are self-employed, I'll mention that low or no deductible health plans may provide better value.
When they sort of work, health deductible health plans are nice because: (1) monthly premiums are low and (2) they give access to a health savings account (HSA) where some amount of money can be stored pre-tax and then used for health related expenses. Of course, none of this saves someone that gets hammered with a $5000 bill like those in the article.
Anyway, the pre-tax HSA account seems to be an attractive to many, and it may be benefit some. However, if you're self-employed, you can deduct your premiums off your income through the self-employed health insurance deduction:
This means that there may be higher tax benefit for a high-premium, but low or no-deductible plan. Personally, I find it much easier to handle than going through the trouble of an HSA.
All that said, it's pretty much all the same in a catastrophic case. Just take the premiums x 12 + out-of-pocket max to figure out the "maximum" yearly liability. At least on the ACA exchanges, this number is typically $11-15k on what I've seen from either high or low-deductible plans. If you can't make this number, you're not fully covered for catastrophic. Alternatively, if the hospital sends a bill to an out-of-network operator, you're probably screwed as well.
Anyway, this is not to detract from the article. This is a huge problem. Mostly, I wanted to pass on some information that I had to sort through when picking and choosing plans over the years.
The tax savings on the difference in premium between high deductible health plans and low deductible health plans is probably $2k at most ($6k in extra premiums @30% tax rate). That’s for single coverage, but even for family total year tax savings can’t be more than $5k.
In either case, triple tax advantage of HSA is far more, especially due to compound growth.
If you have the cash to be able to deal with $10k of medical expenses in an emergency, HDHP + HSA is a no brainer
This is not to say that you're wrong, but I don't completely understand your numbers. My understanding of the triple-tax advantage of HSAs are that
1. Money going into the HSA is pre-tax
2. Investment gains from the HSA are not taxed
3. Money used from the HSA for qualifying health expenses is not taxed
That said, there are many restrictions and two of these benefits seem to be included for self-employed individuals. For example, an HSA can not be used for over the counter drugs unless there's a prescription:
Alternatively, the above link also states that things like office visits to a physician can be deducted, which are things normally an HSA are used for.
Basically, the one benefit that seems unique to an HSA is that the investment gains from the money in the account are not taxed, which is great assuming that this money is used for medical expenses or you make it to 65.
Again, I'm not saying you're incorrect, but it looks like self-employed individuals automatically benefit from 1 and 3 above, assuming itemization. As such, it's seems like the trade off is whether the higher premium, which is less high due to the tax write-off, is worth lower the lower cost of a physician visit. Assuming, of course, we haven't gone catastrophic. What am I missing?
If you save your receipts for any medical care you or anyone else has received that you paid for, you can withdraw from your HSA to "reimburse" yourself at any point in time, including the future.
Q39 at bottom of page 18 of following IRS document:
Have a baby? Save that receipt showing payment for $5k from your post tax dollars, and let the money in your HSA grow tax free for however long you can, and then when you need it (e.g. in retirement), reimburse yourself for the birthing expenses.
It's the first place your savings should go. It's easiest to just model the HSA as a triple tax advantage savings account as long as you pdf receipts for payments for medical expenses. Which you might not in 20s and 30s, but surely will into 40s and definitely 50s, and you can use it for payments you made for other people's medical expenses too. And even if you need to withdraw from it for an emergency, the penalty is only 10%.
Alright, if I understand you correctly, you're essentially using the HSA kind of like a Roth IRA, except that
1. Money contributed is tax free
2. There is a $3.5k contribution limit
3. Money can be withdraw tax free prior to 65, at any time, as long as there's a receipt for the qualifying medical expense that occurs after the HSA was established
Then, from what I can tell, the drawback to this approach is that there needs to be enough cash flow to cover for medical expenses. Certainly, money could be withdrawn from the HSA, but the real tax benefit comes from pretax contributions and that capital gains, interest, and dividends are tax free. Overtime these can provide a huge amount of savings, but they need time to develop. Sound about right?
Correct. There's a higher contribution limit ($7k in 2019) if you have family HDHP coverage. Also, after retirement, money can be withdrawn without paying the 10% penalty and just paying the regular income tax, in case you don't have receipts for medical payments from the past.
I wonder how the IRS would prevent a tax evader using the same receipts for payments for medical expenses for different withdrawals in different years.
How many years do you get audited for? I thought it was just 7. So if you use it every decade, I presume they’re not going through every year and it wouldn’t be seen. Unless they’re keeping a database.
Have you tried an HSA? What are the caveats on yours? Does the money roll over? Are there limits on how much you can put it? Does the bank that owns your HSA invest it? HSA's look like they were designed to save people money, but they are really just another way for banks to get more capital to invest, which is why there are so many caveats on them. I think it is abhorrent that an HSA even has to exist. An easier sol'n would be to allow no minimum limit on tax deductions, it just makes more paperwork for people. But I think HSAs are a bandaid to a broken system.
my last employer had 3 plans, all high deductible. The one with the lowest deductible was significantly more if you hit the max out of pocket and included the higher premium. It was like $10k vs $6.5k, worst case.
Of my past 3 employers over the past 8 years (all family plans):
$3000 deductible, no HSA
$6000 deductible, HSA
$9000 deductible, HSA
I pay $370/month in premiums... $100 of that a fee because my spouse is eligible through her employer but the plans are even worse, so we declined it.
So we pay $4,500/year in premiums. Which equates to roughly a 20% effective income tax instead of ~15% normally.
This is ridiculous. Whomever seems best to get a single-payer plan in place is who I'll vote for. Absolutely no reason it should matter who my employer is for what doctor I can go see or how much I pay in private, personal medical bills.
Retirement accounts I feel the same way, but that's a long way off for the US.
Other countries have solved this fucking problem, I'm tired of elected congressmen firing back with "BUT VENEZUALA" quips every time someone mentions "Medicare for all".
And the proper response to that is "So we should eliminate Medicare altogether then, right? Where's your bill for that?"
One of our company's primary products "helps employees make an informed decision when choosing their health insurance plan". Basically, during open enrollment they are presented with their choices of plans and the "expected total cost" of each plan over the course of the year as calculate based on either, if we have their consent, their historic data or, if we don't have their consent, the historic data of a representative cohort.
The product wasn't getting traction based on employer's wanting to provide such a service to their employees, so the sales pitch was changed. The sales pitch became, "You can save your company money by moving your employees to High Deductible Health Plans. Our product presents data that encourages employees to choose HDHPs over other plans." I'm not sure if that is currently the sales pitch, but it was the primary one for two-ish years. Our customer base is now non-trivial.
I've overheard some of the conversations as to how the "representative cohort" is determined and about our data sources. It wouldn't pass a peer review. Additionally, in the past we have re-worked the numbers because our customer didn't like the results. That is, feedback from the company, not the company's employees. They did, after all, hire us to get their employees to move to a HDHP.
And to top it off, the product hasn't been a great revenue source. So we're effectively compromising real people's health care coverage, for our company's business interests, and it hasn't even been that profitable.
Our health insurance plan at this company is a HDHP...
I tell you all that my company works with employers to move their employees to HDHPs based on sketchy data, sketchy calculations, no transparency, and based on profit motive, and,,,, nothing.
Interesting.
Side note: The chances that some HN readers have used our software are, very good.
I currently have a high deductible health care plan because it is all that is offered by my wife's employer. The deductible is $4,500 per year.
If we just have normal well checkups, normal dental cleanings, normal eye glasses, and a few recurring prescriptions we would never hit the $4,500 deductible.
It is insane going to the pharmacy and having them tell you that the cost is $180 per month and have no choice but to pay it.
I went for a normal diabetes check and the lab work was over $600. No choice but to pay it.
I needed new glasses and no choice but to pay the $150 eye exam and then many hundreds of dollars for new frames and lenses (and I had no choice to get new frames or be without my glasses completely for 1-2 weeks).
To make it worse, we don't have any other choice of plan.
If you're taking a high deductible plan-- which you should be-- you should be contributing the (often substantial) savings on your premium to an HSA. In fact theres very little reason not to max out the HSA for the year. Once your HSA is at the IRS annual maximum, you have an enormous buffer between the often 20% rate post deductible and the Out of Pocket Maximum-- which the HSA will usually cover most of. You should also participate in an FSA, which being frontloaded can absorb early-year shocks.
An HSA is among one of the most tax-advantaged programs you can participate in; I would argue that it is better to contribute just enough to your 401k to get the full employer match and stick all the rest into an HSA.
While I am satisfied with my HDHP + HSA, I'd be a lot more worried if it were my only option (I'm only young for now) or if I didn't make/save as much.
People are getting hit with HDHP only and no HSA? That's rough.
An HSA with no employer contribution, or even administrative assistance, is like throwing money into a trash can, except at least if you throw money into a trash can, you can wheel it down to any hospital and they'll probably accept it.
I didn't know they were available. I thought it could be open to everyone, but employer ones do have advantages.
https://www.fidelity.com/go/hsa/why-hsa
> You could also use it in place of an employer HSA. If you do this, you may miss out on opportunities like pre-tax payroll or employer contributions, so check with your employer to see what they offer.
You can still deduct contributions from income taxes, and you can also transfer funds after contributing to your employer sponsored HSA to your individual one.
I was recently introduced to the idea of gluing and/or stitching one's own body parts or open wounds in case of a severe injury due to the costs associated with US healthcare. I found the nonchalant discussion of such horrible suffering absolutely incredible and would advise everyone to try some medical tourism. Here in Bosnia&Herzegovina, abdominal ultrasound is 20€, colonoscopy is 100€, one tooth filling 15€ and a tooth implant 600€. Nearly all my friends have settled outside B&H but I stayed simply because healthcare is so cheap compared to other, wealthier countries.
The ACA hasn't been what it was supposed to be since 2015. Republicans in Congress gutted the market when they took away risk corridor payments. Small health plans priced with the payments in place, then when they didn't come through, everyone in a loss position went under. The big plans could weather the storm, market consolidates, prices rise.
At Mess (my agency), we were sort of forced into going with a HDCP, but we found a way for it to be a win for everyone.
Our absolutely-perfect no-deductible no-coinsurance plan was retired, and every year, for five years, the cost of our reasonable-deductible no-coinsurance plan kept going up.
Eventually, our broker convinced us that HDCP was the only way.
But I absolutely hated it.
We have quite a few employees with chronic, expensive conditions. Moving a HDCP (in our case 2K/6K family), effectively meant we were cutting their salaries. They were absolutely going to be paying that deductible.
We also employ a LOT of younger people, who just don't go to the doctor more than once a year, maybe. The HDCP wasn't that big a deal for them.
We looked into HSAs – the thing our broker recommended. These are garbage. In theory, we'd put in some amount of money each month, and eventually, over time, the entire premium would be sitting in an account for the employee. For the young and healthy, this was free money. The move to HCDP+HSA was basically a raise for them.
For the chronically-ill, the rate we'd contribute to their HSA was never going to be fast enough to keep pace with their expenses. And for most people, with most savings levels (near $0), a $1500 bill you'll "eventually get back" is just as unaffordable as one they'd never get bet.
I hate HSAs.
"Look, we know most of our folks are NEVER going to hit their deductible. We know a few folks will. Can't we just give everyone a credit card with a 2K limit that they can use to pay for stuff?"
Meet HRAs.
HRAs are like HSAs, but they're not incrementally funded. Instead, it's basically a credit card whose balance I, the employer, pay. It has an annual limit, which matches each employees annual deductible.
These things are amazing.
1. The employee never has to worry about out of pocket cost. They go to the doctor, the doctor charges their HRA.
2. The company has MUCH lower premiums, because we're on an HCDP. I think we saved like 30% or something moving to it.
3. We have a maximum annual additional cost each employee can ring up in medical costs. Worst case scenario (every employee hitting their deductible) isn't fantastic, but we can plan for it.
4. The normal-case scenario is a that a handful of employees hit their deductible very quickly at the beginning of the year, and the rest barely use their HRA at all.
I do not understand why more companies don't do HRAs given the above.
Taxes. HRAs can be a huge headache for employees (never employers). SEHRAs also have a bad reputation for being the worst of both HSA and more traditional insurance plans: underfunded, high overhead for employees, all for severely limited provider choice.
ICHRAs (individual-coverage) are the real bridge between HSAs and traditional insurance—you can use them as an HRA-style account _or_ use the money to buy an insurance plan off a marketplace. While it still pushes the burden of choosing and managing health care onto the employee, they at least have flexibility in coverage as well as tax benefits for both employees and employers.
They, uh, also don't exist until 1 Jan 2020, and they give total control to the employer. If you're a good employer, that's great. If you're a shitty one, the employee is easily fucked over.
I don't get how they'd be headaches for employees? HRA contributions are 100% tax-free and aren't treated as income. It's a pain for my co-founder and I, or would be, if we didn't have someone else doing our taxes.
My company did something different. They couldn't negotiate a decent price to keep the already bad $X deductible (which wasn't terrible, but was still classified by the IRS as a HDHP). We have a lot of young people who don't even hit the deductible as it is.
So, their compromise was to get a plan with a $2X deductible. BUT they reimburse you for any penny spent over $X before the deductible has been payed. The reimbursement if handled by another company, so the company I work for never sees any medical information.
I believe that ACA was partially designed just to get everyone in the same sinking boat. That way one day you could actually fix fundamental structural problems when the real crisis hit.
This error message from Google Chrome Browser is one of the most common problems that everyone faces in our day to day life. Google Chrome warns you whenever it finds out any abnormal tracks taken while you browse things on the web. If you are getting the SSL error in chrome, it means your Internet connection or your computer is preventing Chrome from loading the page securely and privately. However, there are few changes or settings which help you to get rid you of this error.
Check System Date and Time
Disable Antivirus SSL Connection
Clear Cookies and Cached Files
Reset Chrome Browser
Open Chrome in Incognito Mode
Expired SSL Certificates
Update Chrome Browser
This is the point of high-deductable... to cast more spend on the average healthcare consumer. Also to make them price sensitive. Wellness programs are designed around making unhealthy people pay more and not trigger any of the non-discrimination issues as well. Single payer is best model proven at scale in modern countries, but it probably will take a couple decades of watching loved ones not get care before it escalates to action.
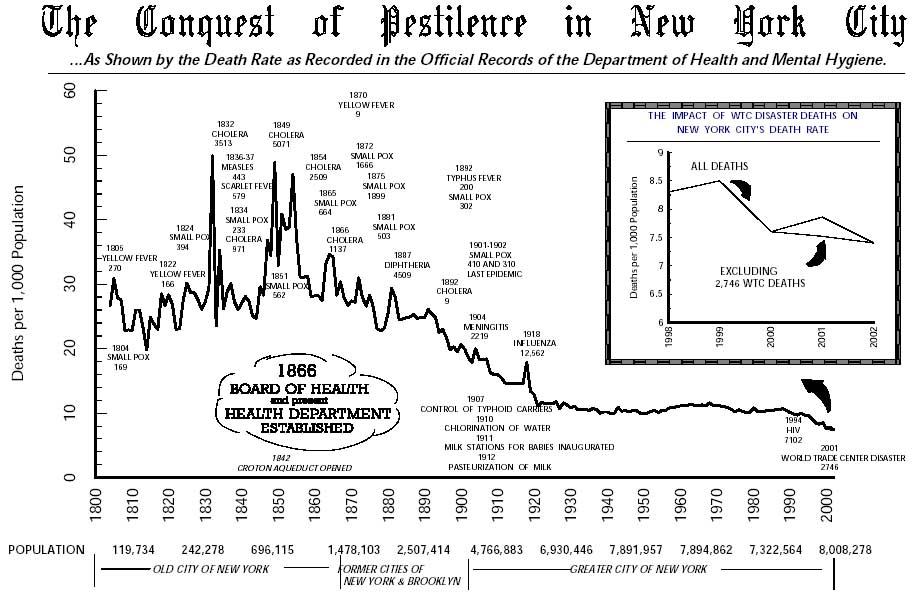{kind=link}
I think people fail to appreciate that prior to the ACA, when the healthcare system worked, it actually worked really well. I got very sick at the age of 20 while I was still on my parents very modest insurance (pre-ACA). Within 48 hours I had an appointment at the best oncology hospital within 500 miles, and I was able to get scans, tests, etc on a very short turnarounds. Ultimately I had two major surgeries in 4 months, and the whole thing probably cost the insurance company a couple hundred thousand dollars. Since my parents had already hit their out-of-pocket maximum, the marginal cost to us was 0.
Now, the "when it worked" caveat is a big one. The story would be very different if my parents didn't have insurance at all or if I hadn't been eligible to be on it. But the same story today on my insurance would cost me a lot more money out of pocket due to a much higher deductible and a higher out-of-pocket maximum.
My perspective is that the ACA made things significantly better for a small group and modestly worse for most people. I'm open to moral arguments that the tradeoff was worth it (although that's not what I believe.) But I dislike rhetoric that pretends there's no tradeoff at all.
Edit: Added substance to a one-liner.