This is absolutely shocking to me. Had my ACL replaced in the UK privately about 8 years ago (no health insurance, paid out of pocket). Total cost was £3000 (+ £600 for initial scan). I could have got it done for free on the NHS but it would have messed up my term time at university.
Like the OP I had meniscal tearing too so more or less directly comparable. (Although obviously 8 years is probably a long time in medical devices so worth bearing in mind).
To put in perspective, that is approximate the same total cost (~$5000) as just _one_ of the pieces of equipment ("Cannula Fast Fix CVD") that the OP lists.
It's one thing if doctors are more expensive because they have to carry higher insurance charges to protect against negligence lawsuits, etc, but that the equipment alone is multiple times the cost seems crazy.
Similar to my experiences as well. I once compared the price of a knee MRI scan across several countries by calling folks I knew.
This is why I was dumbfounded by the call for "innovation" in medical industry at the end of the post. There's plenty of innovation is going on, it's the corruption and extortion we're looking at here: $60K were simply extorted from a person in pain.
Or more specifically from all of us. The author only paid $2400. The whole system is designed to be opaque and non-competitive so they can just bill insurance companies for whatever. I wonder what it would have cost if he said he was paying in cash (hint: a lot less).
You'd think that it should be "a lot less" for someone paying cash, but this is almost never the case (in the U.S., anyway). Insurers can threaten to remove a hospital from their network if the prices get too high. The hospital doesn't want to risk losing the large stream of sick/injured patients from the insurer, and usually couldn't care less about one person deciding to have surgery else for reasons of cost (edit: see last paragraph).
Individuals paying cash (and individuals without insurance) are generally stuck with the "sticker" price for care (higher than what private insurers pay, and significantly higher than what medicare pays (medicare basically gets to "declare" what they're willing to pay for a given procedure and hospitals generally have to go along with it or they'll lose some/all federal funding)).
It's usually very difficult to renegotiate the sticker price without an insurance provider or the government working on your behalf. If it's a time sensitive or life threatening procedure, you'll often have other more pressing action items than haggling over the price. It's even harder to negotiate after the fact, since hospitals make you sign away whatever bargaining rights you may have had before they'll agree to treat you.
[edit]
Finally, hospitals generate the bulk of their revenue from insured patients. They can and do quote higher prices to uninsured patients, but the fact remains that this is a fairly risky patient pool for the hospital, since many of these patients will sign whatever they need to sign in order to get treatment, despite being completely unable to pay the (relatively huge) prices quoted.
Hospitals have incentives to keep this pool as small as possible, and occasionally resort to extreme measures (legal or otherwise) to get rid of these patients [1]. Though the hospitals often aren't able to collect the full price from many of these patients, you would be naive to believe that they won't send collections agencies after you and utterly ruin your credit rating if you find yourself unable to pay.
I've never had major surgery so perhaps it's different for that, but I've found (through periods of no or crappy insurance) that doctors visits are significantly cheaper when you say you're paying in cash.
I got my ACL replaced in Argentina and the cost including rehab was about U$S 3000 having one of the best insurance companies (about 120 U$S a month). If I wanted to use the public care, it could probably cost almost nothing.
It always amazed me that in the US the health of a person is not a right and if you get hurt doing anything you have to pay huge fees.
That's because in Libertarian Utopia everyone of importance will be independently wealthy, and those who aren't, deserve to be trampled by the others. /sarcasm
Libertarians have been complaining about the USA's complicated health bureaucracy for decades. Hell, they've written dozens of books about it. It doesn't take a genius to find perverse incentives in US medical pricing schemes.
But don't let me get in the way of your 30 seconds of hate...
I've met plenty of people whose political views on health care were along the lines of:
Person 1: "You should pay for your own care"
Person 2: "What if you are poor and can't?"
Person 1: "Sucks to be you."
With the possible addendum of:
Person 1: "But charity organizations will cover
the costs for those that can't pay,
because then I can choose of my own
will to put money towards the cause."
Person 2: "What if not enough people donate?"
Person 1: "Well, it sucks to be poor."
[I'll note that "sucks to be you" as an answer could probably be translated as, "I have not thought out my position that far, and I don't like you challenging my views, so I'll give you a short and curt answer."]
Can the issue of who pays for healthcare be adequately separated from the issue of its cost? I think so -- given how wide the disparity in health COSTS (put aside the payer) are between not only countries, but even counties in the US [1].
It would be great if we can talk about the origin of these health costs without getting entangled into who should be paying them. But maybe that's an impossible task.
The Libertarian-in-Chief Ron Paul himself a Physician who claims that the exhorbitant costs in health care are a more recent phenomenon. He quotes how much his costs were to do house-visits (remarkably small), and compares that with the ballooning in costs more recently. While one can argue that Libertarianism is a Utopic view, the rapidly escalating prices of healthcare are not something that is espoused by Libertarian philosophy. I.e. Low health costs and individual responsibility for health paying are not incompatible. Then again, neither are low health costs and universal health coverage. Right now, we have the worst of both worlds: high health costs and individual responsibility for payment.
Can (some of) the ballooning costs be attributed to the costs / time investment in medical school? When Ron Paul went to medical school how much did it cost (adjusted for inflation)? How much more knowledge are doctors expected to have now than then?
Maybe, but not any significant part. As evidenced by this post, only a small portion of the costs are attributable to the work performed by the surgeon. The majority of costs are allocated to facility costs (whose increases in price are not related to tuition costs) and equipment.
Indeed, if there was such a direct correlation between the two, the easiest way to control healthcare costs would be to reduce doctoral school tuition rates. Clearly, this is not a viable solution here because the two are not directly correlated.
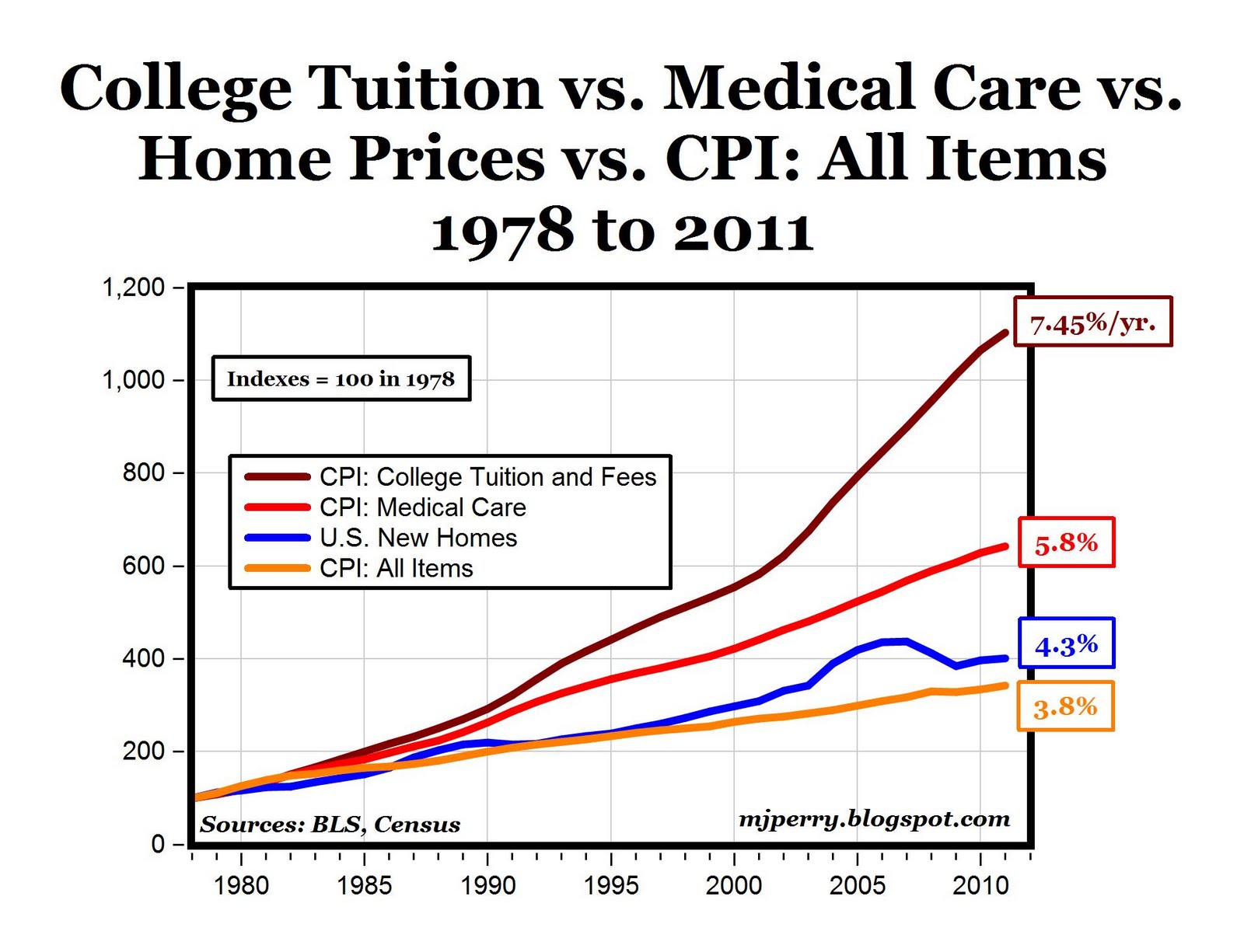
Now, it is true that Tuition Costs have risen at a much higher rate since 1960 than Health Care costs on a percentage basis compared to inflation [1] [2] [3], but in aggregate the actual health care costs on a per-individual basis dwarf total tuition costs as part of household income [4].
To be fair, comparing the costs of ACL surgery to Ron Paul's costs for 'making house calls' isn't exactly an apples-to-apples comparison either.
I'm merely pointing out that this is a complex beast with many contributing factors:
- The money/time investment to become a medical professional.
- The increase in the number / complexity of procedures over the years. Our medical knowledge keeps increasing we keep getting more and more ways to fix things.
- Comparisons without details. For example, people like to compare how cheap MRIs are in Japan, but the MRIs that people get in Japan aren't as powerful/accurate as the ones that are charged for in the US. Does this justify the cost difference? Maybe, but maybe not.
When an ACL costs $68k in California and $20k in Illinois and $32K in Delaware, you know that it's not an issue with simply the cost of getting medical training. Something else (I agree, something a lot more complicated than simply the cost of education or differencies in country-specific medical practices) is at work.
I think we actually agree here - the dramatic rise in health care costs doesn't have a single root cause, or even perhaps a readily identifiable root cause. It's systemic, rather than simplistic. Education is a factor, but a small one. Insurance and health liabilities are probably an equal factor. But neither explain disparities in cost within the US (no need to look at comparisons between Japan for that). See my [1] reference two comment posts up for the chart on cost disparities intra-US.
It's quite possible that medical suppliers are using information asymmetry to overcharge in some instances and properly charge in others. Could it be as simple as that? Why is it that the same procedure with the same equipment using similarly trained staff in similar hospitals with similar liability exposures would have such different costs? The only thing I can think of is that medical purchasing is sufficiently complex and with such little visibility and transparency between different establishments that medical suppliers and providers can get away with pricing them "as much as the market can support". But that's just an unsubstantiated theory and maybe there is a reason why the same procedure is cheaper in another state, county, or city.
It's difficult to see which factors are contributing without a similar breakdown for a similar procedure from somewhere else.
Are doctor's costs more expensive in CA due to the increased cost of living? Ditto for administrators, driving up the hospital costs? Is it due to a scarcity of hospital beds / operating tables that the hospital charges 'what the market will bear' in more densely populated regions?
Today with the US-based insurance system, there's usually at least one whole employee at every doctor's office whose only job it is to figure out who pays what, and do all the related phone calls and paperwork. For example talking to every patient's insurance company and turning medical procedures into ID numbers.
If the doctor sends you to get lab work, the lab has its own person that fills that role. If the doctor sends you to a specialist, ditto.
Of course the insurance companies have their own hordes of employees who write all the rules of who pays what under what circumstances, keep the books of all the patients' deductibles and all the providers' bills, etc.
None of these employees does anything economically productive. They just move money around.
Obamacare requires that people buy health insurance, which protects this bureaucracy with a legal mandate to purchase their services, and creates more bureaucracy, on the government side, to administer the law.
How can you guarantee the health of a person? Doesn't that incentivize risky activities? If someone else will pay to stitch you up if you get injured, or cover your drugs if you get sick, or keep you going in your old age if you make terrible long-term lifestyle choices: wouldn't that skew the overall population toward cheaper, more convenient, or more fun decisions at the expense of the state?
I live in the UK, so all my medical costs are covered by the state.
However, I still don't go base jumping. Even if the costs are covered, I still don't want to spend six months in traction after I break my back because the parachute didn't open. Similarly almost all the people I know either don't smoke, or want to stop smoking, because even if you can do it free of charge lung cancer just isn't much fun.
You mean your medical costs are covered by taxes you pay and taxes other people (and corporations) in the UK pay and the costs of medical research and development that might benefit you are paid by people in the US.
I think that getting hurt or sick has enough pain or tragedy for itself and thats why people dont want to feel it.
If you hurt yourself and someone patchs you up, its not the same, my reconstructed knee will never feel the same as the other.
I think that you pose people that whant to benefit as much as they can from the state, and I think that I know noneone that does that, at least in health care, nobody wants to go the hospital
There are debates about how much "defensive medicine" adds to the cost, but those aren't all that relevant here since the costs presented are exclusive of additional tests, etc.
$7,638 per person per year. That just can't be right. I and 90% of the people I know haven't made a significant trip to the dr or hospital in years. Where the fuck is that money going?
Incredible! Even more important, I suspect nowadays, most people live more years after 40 than before. Maybe a goal should be figuring out ways we can push back that age.
Cancer elevates cost dramatically. I had cancer at age 41; I kept track of the full costs (not what my insurance negotiated downward) but stopped after my surgery, chemo and radiation treatment passed the $500k mark. I still go in for tests on an annual basis, so my guesstimate is that my total cost just for my cancer has probably surpassed $1 million. Even if that got negotiated down to $100K, that's still a lot. All it takes is one life threatening event, or a chronic condition to skew things out of what we would normally think is "normal" and rational in expenditures.
P.S. Thanks to my excellent doctors, Nathan Green and Richard Pitsch...
> $7,638 per person per year. That just can't be right. I and 90% of the people I know haven't made a significant trip to the dr or hospital in years. Where the fuck is that money going?
Even if the people you know were somehow a representative sample, that's not all that surprising. A significant health event can easily cost orders of magnitude more than $7,638, so even if 90% didn't have one in a period of several years, the average cost could still easily be $7,638 per person per year.
Try getting even a relatively minor health problem like appendicitis and you can go through several times that much in one day. Healthcare would be much cheaper if only we didn't have to deal with all of the sick people.
Also, liability caps are the stupidest way of dealing with the potential for frivolous ligation. It punishes the people who were actually injured, not the ones who filed a nuisance suit hoping for a small payout. It's utterly non-sensical!
We hear about medical tourism from the US to India, Thailand, etc., but with these kinds of price discrepancies between the US and UK private practices, I wonder why there aren't more Americans who go to the UK for surgery?
The fraction of patients without insurance but with enough cash and motivation to fly to the UK purely to seek savings on medical treatment has got to be fairly tiny.
My impression is that medical tourism from the U.S. is not typically for cost savings, but rather because particular procedures are either completely unavailable (experimental stem cell treatments) or could require long wait times (liver transplants). I'd love some data on this. Wikipedia's rather poorly written article suggests MT is more popular from countries with socialized systems in order to reduce wait time, but I'm skeptical.
> The fraction of patients without insurance but with enough cash and motivation to fly to the UK purely to seek savings on medical treatment has got to be fairly tiny.
Well, if my options are to spend 60 grand on an ACL repair in the U.S., or significantly less than that on a first-class ticket to London, some serious fun, and an ACL repair...I know which one I would choose.
Those weren't your options. As with most things health related in the US, someone else was paying (the "insurer" in this case). Given the choice between you paying $2,400 in the US (and the insurer paying an amount you don't see or care about), or you going to the UK and paying 3,000GBP plus accommodation and tickets, I'll bet you pick the former.
Were we looking at the same Wikipedia article? Its first sentence is "Medical tourism (MT) is patient movement from highly developed nations to other areas of the world for medical care, usually to find treatment at a lower cost." Later: "[I]n the US, the main reason is cheaper prices abroad." And while I agree that it's not especially well-written, it does provide some hints as to why even insured people might like to go: elective cosmetic surgery, elective orthopedic procedures that may not be necessary but may improve quality of life (knee replacements, etc.), or reproductive procedures like IVF, all of which may not be covered by insurance.
> I wonder why there aren't more Americans who go to the UK for surgery?
Because a sizable share of the Americans who could afford even the UK surgery prices plus travel and accommodations to/in the UK also have health insurance which covers the procedure in the US, and makes it cheaper for the patient to have the procedure done in the US even if the total cost is more expensive.
We don't really have any price signals for the vast majority of our health care system, when in reality only a tiny minority of it is hard to price (emergency care is hard to price).
One point on disposing of fancy, potentially reusable, tools: We do more than a little precision machining in our lab. When a job matters, the shop buys new tooling. It's lower in cost, especially time, than verifying that a tool is sharp and correct.
At first, it seems wasteful to throw away a once-used tool, but if all you do is critical work, you must be certain that your tools are reliable and correct. Once you have a complete set of nice hand-me-down spares squirreled away for coarse work, any subsequent used tools go in the recycle bin.
For the computer-inclined, this practice is no different from taking a perfectly functional linux installation you've used for a little while for a side project and using it on a mission-critical task. It's easier and more reliable to reformat and reinstall than to inherit whatever curiosities might emerge from the past.
To be fair, you're doing exceedingly delicate machine and test equipment manufacture. The machine shops I know will buy new tools as needed, but reuse them on large job runs--and throw them out once they lose tolerance.
Something like the $900 knife in the article is/could be a mass-produced stamped piece of metal, perhaps sharpened on-site or at the factory; unit cost for that should be easily less than $10.
> The machine shops I know will buy new tools as needed, but reuse them on large job runs--and throw them out once they lose tolerance.
Hospitals aren't machine shops, though, so it would be a significant additional cost to equip and staff them to evaluate tools for reuse.
There's also particular costs around requiring additional handling of used surgical tools rather than disposing of them that may not exist to the same extent with used machine tools.
And its quite possible that even breaing all those additional costs, a large percentage of tools would be out of tolerance or otherwise unusable after being used once, so you'd be paying the additional cost and still disposing of them.
Right, right--but the point here is that economies of scale have driven the cost of machine tools low enough that they can treat them as disposable for the type of work they're doing.
This whole thing seems more a collection of specialized widgets that offer only marginal utility over a stock scalpel, and which aren't priced to reflect the sheer triviality of their manufacture.
Maybe somebody finally needs to be enough of an asshole to say: "Look, we're done with stupid one-off tools. Shit doesn't scale."
It sounds like medicine is trying it's hardest to be the same sort of logistical nightmare as maintaining automobiles.
I guess part of the one-off nature is that post-op sterilization isn't cost effective; perhaps you simply can't remove the bits of the previous patient from the tool cheaply enough or without degrading it in some way) to justify not just opening another one.
Another point is that this tool (to take an example) offers one huge advantage over a scalpel; it will make both cuts simultaneously, reducing the margin of error. I wouldn't want to hear "Well, we messed up taking the first piece, so we need to do it again on the other side". It HAS to be right first time.
How special are we talking about? There are 100,000 of these surgeries in the US every year (and then tons more globally). It's not like this is a part for the space station.
A quick search on ebay turns up, for example, a set of 4 for $35.
They're plastic with (I hope) steel blades.
In general, though, the cost is certification (+ liability insurance) and documentation of provenance. Basically, every time it's touched by a human, add $100, because the person has to be "trained", they have to log any actions they've taken with it, and they have to make sure the certificates go with the tool wherever it goes.
"Something like the $900 knife in the article is/could be a mass-produced stamped piece of metal"
Very well could be some liability potential wrapped into reuse of a device. After all part of the cost does go toward covering things that go wrong for whatever reason.
If you take the device fresh and something isn't right you can claim it was defective. If it was used for another operation who is to say when something happened to it?
An inverse analogy might be the difference in potential problems from using a hard drive that has been previously used where something is later found vs. using a brand new hard drive.
What do you want to bet that the US is the only place in the world that this product is sold for anywhere near $900? It's a plainly ridiculous price (and I'm sure the insurance company didn't actually pay it, but that's another debate).
>If you take the device fresh and something isn't right you can claim it was defective. If it was used for another operation who is to say when something happened to it?
There's something on the order of 100,000 ACL tears per year. Even with no reuse, it seems odd that economies of scale can't get that well below $900.
And human medical procedures that aren't typically covered by insurance. LASIK for example, imagine what laser eye surgery would cost if it was billed like an ACL reconstruction. Instead you have to pay yourself and doctors compete, the entire bill (at a nice place) ends up being what a couple of ACL knives cost.
Gah, excellent point. Elective retail procedures such as vision improvement surgery and dental crowns, bonding, veneers, etc., all seem to top out around the average FSA limits of $5,000 or so. It's especially notable around the end of the year when advertisements encouraging people not to waste their FSA funds start picking up on the radio.
Now that the IRS has apparently imposed a limit of $2,500 on FSA deductions, I wonder if that's going to create pricing pressure on the "high end" procedures such as custom/wave/whatever LASIK here in the USA.
If I weren't a lazy sod, I'd look up capital equipment costs for medical procedures such as those and compare them to MRI, EKG, and other items used primarily for "need" based, insurance paid, procedures.
(Actually, I haven't used any fancyhands requests in a couple months. I'll be lazy and have someone google for me.)
In the case of medical equipment, the gold standard to prevent contamination from previous patients' biomatter is to use new equipment each time. There's a demonstrably lower rate of infection than even if the equipment is cleaned to approved standards. I believe I should be able to find the paper I read discussing a while back, if you'd like.
Interesting read, and a valid criticism of the costs associated with ACL repair in the US.
It would be nice to know, however, how much your insurance company actually paid for the procedure. There's probably a large discrepancy there.
My own thoughts are that if there were a true free market for healthcare, with insurance only for real medical emergencies, the costs of a lot of these services would drop, including physician fees, equipment etc. Most of the population would not, and likely could not, pay 68,000 for an ACL repair, which would leave medical providers the option of 1) lowering prices substantially or 2) being out of work. Having put ourselves on high deductible health plans, we are super vigilant now about how we spend our healthcare dollars. And having realized the impact of this, since we are medical providers ourselves, we are now transitioning to a model where we are not participating with many insurance plans, but our fees will be completely transparent - published online - and fairly reasonable (I think).
"with insurance only for real medical emergencies"
You then have people putting off preventive care, tests etc and then you have to cover a bigger problem down the line.
I'll give you an example. You are a landlord with a tenant and you tell the tenant "you have to take care of minor repairs I will cover anything major". As a result they don't do normal maintenance either because they forget, don't care, who knows. Then because of lack of that maintenance the compressor fails on the HVAC and you end up having to replace a unit. Good luck with trying to tie that to the lack of maintenance. Or saying you won't cover it.
The idea is to have the right incentives in place. The premium for medical emergency insurance would go down as you are more proactive in your healthcare.
For example, by having an annual physical, maintaining your weight, etc. you would get a discount.
"care now to avoid paying the $5,000 deductible down the line."
Does not answer the question of what to do with people who don't have a pot to piss in. You aren't going to deny them medical care. That's the problem. Just like you can't say "if you smoke we won't fix your lung cancer" (forgetting even if the link could be clearly established).
Bottom line: You have to prevent people from their folly. Although certainly some people would respond to the incentive in your example.
You're right, there is a discrepancy and I didn't think to put it in the article.
I couldn't find the doctor's charges on-hand, but the total cost for the facilities/drugs/equipment was $48,851.82. The insurance ended up paying $14,742.88 of that post-adjustments.
$14,742.88 is the real cost since hospital are running off of the income from what insurance actually pays. if average people were able to pay the "insurance adjusted price" for most things they would not need insurance for most things.
Somewhere within the regulatory frameworks in which health insurance and hospitals operate, there's got to be the leverage to make pricing and other metrics like infection rate, readmission rate, etc., transparent.
Otherwise you can hide some serious price gouging in that fog of bogus prices.
I'd rather just let any citizen/taxpayer pay the medicare or medicaid rate for a medical procedure out of pocket if he wishes. That's even lower than the insurance negotiated rate, and hospitals/doctors would have every right to exclude all medicare/medicaid patients if they want (many private doctors do, but generally hospitals don't, since they depend on the volume from medicare, and there are some other benefits for residencies).
There's a slow trend toward doctors not taking insurance. A few of the higher profile cases have seen private practices reduce their prices between 50% and 80%, while still making a very healthy profit. For those that need charity care, they're actually able to provide it due to having a huge block of resources (time and money) not being tied up dealing with insurance claims.
I commend your move toward transparent prices for the services you provide in the medical industry.
When I was in college, I couldn't afford health insurance (no parents + financial aid does not cover it). I played rugby (generally not the safest sport) for two years, in addition to playing pickup basketball all four years. I very fortunately did not sustain any major injuries.
Six months after graduating (and getting a job with health insurance), I tore my ACL while playing pickup basketball. The costs were as insane as outlined in this post, but, again, I had health insurance. However, to this day, I'm horrified at the thought of what would've happened if I'd sustained the injury in college when I didn't have health insurance. Shame on me for putting myself in those sorts of situations, but it feels like there's something wrong when the penalty is so harsh.
You wouldn't have paid anything like $68k. As mentioned in the article, those prices are inflated for charging the insurance company, who in turn negotiates a much better actual price. Similarly, the hospital would have likely worked out a better deal with you. Or, if you qualified (and it sounds like you would have), then Medicaid would have initially picked up the tab and they would have negotiated a better deal for themselves.
In none of these scenarios does anybody actually pay the made-up $68k number.
The hospital would have worked out a better deal with you if you asked. However, if you don't ask, and just put yourself horribly into hock to pay them, they'll take the money. Likewise, if you refuse to pay, and they have to go to collections or the like, they'll apply the full, inflated amount.
Possibly, but look at the picture of the sliced out tendon. ACL replacement is an inherently complicated operation, from a highly skilled practitioner. The take-away from that is: you can't afford to play a dangerous sport like rugby if $5-7k is financially crippling.
The most useful aspect of this article is the pie charts and line-item comparisons. Ignore the dollar amounts themselves. Why? Because almost no one pays that. Why?
- In California, MediCal (state-wide health insurance safety net) pays about 20% of the cost (not price) of treatment for those without insurance. So if a surgery costs $10k, MediCal says "Here's your $2k. That's all you get."
- Nationwide, Medicare pays something closer to 90%. Much better, but still a loss to the hospitals.
- Insurance companies negotiate with hospitals, but (from what I've heard) generally pay 115-125% of the cost, giving hospitals a 15-25% margin. Certainly better, but not necessarily making up for the above.
- Some patients with no insurance, especially at major academic medical centers, are rich folks looking trying to get the best care in the world for something particularly complicated. UCSF in my neighborhood even has an in-house Saudi liaison for Saudi royals. These folks pay the full rate, which may represent an enormous markup, which does help subsidize the care of the top two categories.
For those without insurance, who don't have the money to pay the full fare (meaning you're not a foreign prince or similar), you're going to get freaked out by the bill, which is based on the last category. But in reality, the moment you ask a billing person about the costs, you'll almost always get knocked down into the insurance rate tier, just for asking. Show proof that you have next to nothing, and you could get well down into MediCal levels.
In order to get the ultra-rich to subsidize the patients that generate the loss, the price card needs to be high. Really high. So they give breaks to everyone else, since you can't do it the other way -- "Oh, you look rich, so we're going to charge you double the rate sheet."
This doesn't happen in community hospitals quite as dramatically, since they don't have the ability to handle the crazy conditions that will result in the high-revenue customers. So their rack rate for an ACL will be at the low end, while the academic medical centers that offer the $2MM neurosurgery will have rack rates for every procedure on the high end.
Is it messed up? Sure. But does it mean that normal people are paying $65k for this ACL procedure? Usually not.
This is true, but often the discounts aren't as steep as you'd think. I had a mitral valve replacement a couple years back (at age 29, due to a one in a million condition), and the insurance company was billed ~350k for the surgery + recovery in hospital. Even after their discounts, the total still came to $~250k (this is not the normal price - I had a complicated recovery, and spent an abnormal amount of time in the cardiac ICU). I, however, only had to pay ~$4,500 or so (high-deductible plan).
Yup, and if course it varies. Complications are a huge driver of costs, so making marginal improvements to the complication rate (either by improving the standard of care OR by insisting that you go to a place with a low complication rate) can have an outsize impact on the cost of care in the aggregate.
Companies like ConsultingMD (horrible name, http://consultingmd.com) are taking this approach to reducing costs.
1) You can't turn an operating room immediately. A 1hr surgery requires significant prep time _AND_ cleaning time. These rooms are used for many different kinds of surgeries — changing everything takes time. To make matters worse, each surgeon has their own preferred set up, and it needs to match that.
2) All medical supplies are expensive in part because your body is pretty sensitive, and you need to be careful about what's in there, but also because doctors almost always have _COMPLETE_ control over what equipment they use ... including screw and tool brands. This means that hospitals have little-to-no leverage to get lower prices. This is particularly true for implants & other complicated equipment.
So, have a deal that says "Hey, if you want to be able to receive Medicare/Medicaid payments, you have to standardize tools."
All the hospitals will say "Wow, holy shit, alright", and the surgeons will have to play ball--because a surgeon without a proper OR is basically just a butcher or barber.
EDIT: Please explain why this is a bad idea instead of just downvoting.
As an anesthesiologist, this is a bad idea for various different reasons. There are a numerous reasons why a physician needs the tools that he needs. The type of procedure, the type of patient and the familiarity of the equipment. I routinely intubate patients with a particular type of tool because that is what I feel most comfortable with and I have trained with. Yes, I can intubate with the myriad of other devices but there is that 1 out of a 1000 chance (slim but not unrealistically slim because I do >1000 intubations a year) that I cannot intubate you and you need to have a tracheostomy or worse, you die.
Some may argue that we should all train with the same equipment, but even then, what about inherent differences in the physician or the patients. Maybe where I trained, all my patients had large tongues and I need a particular blade more often so I became better skilled with that or maybe my hands are just better with a particular blade.
If I dropped a Linux admin off at a shop which didn't have emacs on their boxen and he refused to work because he might accidentally screw up a config file, he'd be laughed out of the joint.
If I dropped a plumber off at a job site and she didn't have a particular type of ergonomic monkey wrench she'd grown accustomed to and said she couldn't do the job, she'd be mocked endlessly.
If I dropped a line chef off at a kitchen and they didn't have their favorite knife available and they held up orders for a whole night, their boss would fire them.
~
This custom bespoke medicine nonsense is increasingly seeming to be just that: nonsense.
Sure, there's this .1% chance that you might screw up an intubation, but that seems to be more of an issue of bad training than bad equipment.
As far as your point about differences in patients or physicians: that's a cop-out. Part of being good at what you do (as a dev, as a maker, as a person) is being flexible enough to make do and succeed.
In a system which costs as much as ours does to people who simply can't afford it, we (as a society) cannot afford to cater to the whims of overspecialized professionals.
> If I dropped a Linux admin off at a shop which didn't have emacs on their boxen and he refused to work because he might accidentally screw up a config file, he'd be laughed out of the joint.
The kind of errors made by a Linux admin who is more familiar with emacs using vi don't have as much likelihood of ending up with dead customers and massive liability for the Linux admin and/or his employer as the kind of errors that could be expected from a surgeon being forced to use non-preferred equipment.
So the situations aren't exactly parallel.
> In a system which costs as much as ours does to people who simply can't afford it, we (as a society) cannot afford to cater to the whims of overspecialized professionals.
In a system which costs as much as ours does compared to every other advanced country, while providing worse access and not producing better outcomes, we certainly can't afford to not do some research to figure out what everyone else is doing right and we aren't.
But somehow I don't think letting surgeons choose the tools used for a particular surgery based on their own expertise and understanding of the needs of the particular surgery, rather than having one standard kit used for all surgeries regardless of the specific details of surgeon and patient, is the difference.
"But somehow I don't think letting surgeons choose the tools used for a particular surgery based on their own expertise and understanding of the needs of the particular surgery, rather than having one standard kit used for all surgeries regardless of the specific details of surgeon and patient, is the difference."
In isolation, your intuition is correct. But, with thousands and thousands of surgeons performing hundreds of thousands of surgeries a year, we end up with a logistical nightmare. This doesn't scale.
It's perhaps not the main difference, but I'm willing to wager it is at the least a symptom of whatever the underlying problem is.
> It's perhaps not the main difference, but I'm willing to wager it is at the least a symptom of whatever the underlying problem is.
I doubt its even a symptom: because I don't think the other OECD countries that spend less for broader access and equal or better outcomes use one-size-fits-all-surgeries standardized equipment kits, either. But even if it was a symptom, it would be better to treat the underlying problems.
If an engineer or machinist used to working with SI tools goes to work somewhere using metric measurements, perhaps building equipment for space travel...
Oh wait.
Obviously, doctors can get things done under less than ideal circumstances. I'm sure every TV show has had an episode of someone doing an in-field tracheotomy with a swiss army knife and a biro cap.
A license is not necessary for a Linux admin to work (in general). Screwing up a service file isn't on average going to result in the CEO of his company having a meeting with the company's attorneys and practice review boards to determine how much to pay the victim of his edits.
Worst case based on negligence (maybe taking all the zones down for a DNS provider), the admin loses his or her job.
You're comparing something minor with something that has both a high risk of serious damage or death (throw the statistical average value of life in here) plus an environment (especially in the USA) where attorneys advertise on bloody public buses for people who were "harmed" by a doctor, and there's a lot of ass covering with best practice behavior.
The human body is not a car (there's the metric/SI thing again). Things are bigger, smaller, in a slightly different location, softer, harder, or any of a million other combinations of complications that make it safer to use appropriate customized equipment.
In all your examples, you aren't dealing with a person's health or (potentially) life. The risk-benefit calculation changes (and people become, understandably, somewhat irrational) when the stakes get that high.
This kind of thing leads to ridiculousness like the "death panel" meme. The American healthcare system prizes choice and expansive options at the cost of, well, almost everything else. This means that wealthy people can receive a higher standard of care, but does make things very very very expensive.
One thing to be aware of in how all of this stuff works; oftentimes medical billing codes don't map 1:1 to exactly how things work in the hospital, so the medical staff puts together a statement of everything they did, and then the billing staff (approximately) maps it to billing codes.
This means that they'll overshoot on some codes to make up for other acts and overhead that doesn't have an exact billing code, and every medical provider has different places that they'll overestimate, and by different amounts.
Additionally, as most people know, the billed amount is usually FAR in excess of what the insurance company actually pays.
I'm not in the industry so I may be off base here, and someone who is can correct me, but I just finished Oreilly's excellent ("Hacking Healthcare") which is about how patient services and billing work.
His expense report comes back from accounting with everything approved except the umbrella. He appends a note to the report explaining that the umbrella was destroyed in the line of duty and resubmits. Back comes the expense report, with a rather severe note from accounting to the effect that umbrellas are not on the list of allowable expenses.
...Our frustrated manager tears up the old report, then sits down and fills out a whole new form: $3.94 for lunch, $12.75 for laundry charges, and so forth. Which he sends to accounting with a note attached: SEE IF YOU CAN FIND THE UMBRELLA NOW!
I had mallet finger once and they coded it as a broken bone with the associated costs. They wanted to charge me for a full broken bone and typical time spent with hundreds of dollars of costs when all the doc did was spend 5 minutes, give me a plastic splint and tell me to not bend the finger for 8 weeks.
After many phone calls I finally got someone on the phone who realized how idiotic the code was and changed it to something more reasonable to the service rendered.
I was expecting this to be about Access Control Lists being slow or requiring more complex security reasoning (vs owner/group/other). It's not, it's about health care and injuries and something that's part of your knee.
(I am slightly hesitant to publicly share info like this, but what the heck...for science!)
I tore my ACL 1.5 years ago playing soccer, and went through a similar surgery as the OP at NYU Langone Medical Center in New York. Interestingly, my final bill for the surgery (including the same things as the OP) was almost the same - $67k and change.
However, more importantly, the actual amount paid to the doctor/hospital etc. was $18k, of which I think I had to pay around $2k, insurance covered the rest. So while the sticker price might be $67k, the actual cost is significantly lesser. In the bills that I saw from my insurance company (BCBS), for each line item, they would have a column for "Allowed Amount" or something like that which generally varied between 20-30% of the billed amount.
On a different note, I don't whether the cost would have been the whole $67k if I was uninsured. I hope not. But if yes, that's really punitive to the people who can least afford it. For that matte, even a 18k cost is prohibitively expensive for someone who cannot afford insurance.
The way understand it, yes, the uninsured person would receive the $67k bill, but can then go and negotiate to lower the amount payable. Insurance companies just did that negotiation beforehand and have a standing agreement with the provider. All of this reeks of huge inefficiencies to me. There are people at both the insurance companies as well as at every health care service provider whose full time job is to negotiate rates with each other?
I've been in this situation, and there is no comparison at all. Nobody but the very wealthy can afford to pay out of pocket for healthcare. A single, minor injury can cost you $50,000 - $100,000. A chronic condition, cancer treatment, or major surgery can easily head north of $1 million.
Sure, you can try to negotiate pretty much anything. But what kind of leverage do you think you have? Insurance companies can put many millions of dollars of revenue at risk with the threat of dropping a stubborn healthcare provider from their network.
In contrast, your negotiation position is A) please? and B) I may be forced to declare bankruptcy, in which case you may or may not get your money. If you have enough assets, then option B is basically another form of A: "please, don't take away my house or the savings I've spent my life earning." The bigger your bill, the greater the incentive to deal with the annoyance involved in collecting from you. The likely consequence of your personal financial ruin doesn't enter into their calculations.
Yeah, I wouldn't recommend this route, either. I read an article in The New Yorker about body parts harvested from cadavers that were used in transplants. The parts were way past their harvest-by date. This was discovered, at least partially, by someone having an ACL transplant from one of this bad parts, and the recipient of the bad part died from bad infection due to a mold on the tendon.
The lack of controls on that business forever made me wary of using cadaver parts for transplants.
The lack of controls on that business forever made me wary of using cadaver parts for transplants.
I didn't know that, but cadaver parts freak me out so when I had my ACL done I did the standard patellagraph. If I tear the same knee again I'll have to go cadaver or hamstring, but hopefully that never happens (knock on wood). The problem with the hamstring is it never quite heals as strong.
As an aside, pro-athletes typically go cadaver because the time to heal can be quicker. They probably aren't getting bad ones though.
ACL stands for Anterior Cruciate Ligament. (In case I'm not the only one who didn't know and was surprised to see this was never mentioned in the article or the comments.)
I had ACL & torn miniscus surgery 16 months ago and live in Canada, here are my experiences (excellent breakdown btw). It changed my life in many ways, but that's another story.
Though surgery is voluntary and I injured it playing soccer, the operation is covered by Medicare (which is a mandatory $64/month as I am self-employed).
So not including opportunity costs for missed work and time for pre and post-op doctor's visits (about 8 of them), my costs not covered were:
- Post-surgery pain killers: $30 for T3's for a week. I refused the Percocet's, although the pain was bad I could still sleep.
- Physio visits. They'd have you 2-3X per week for the whole duration if they had it their way, at $70 per appointment. I can't afford that, so I went once a week for three months = $840.
- I declined the $900 custom knee brace that helps you get back playing sports sooner.
- Rental of crutches for two months $25
And crutches are NOT as easy as I once thought, when you'd hop around on hour friends crutches for a few steps. I'm pretty fit, but a few blocks in them has you sore and sweating. Take care of those knees!!
I also had my ACL replaced (hamstring autograft), in SF, about 2.5 years ago after a basketball injury.
I'm pretty sure these prices are starting 'list' prices, whereas the negotiated/'allowed' cost that you and your insurance company actually wind up paying tends to be 1/2 to 1/3 these numbers.
My surgery was also about 3 months after the injury, which isn't optimal. It took me a few weeks to see a doctor, I didn't like the 1st doctor I saw, and by the time I'd settled on a preferred one, I needed 6 weeks of physical therapy to undo some of the post-injury weakening of surrounding muscles. (Since there's also atrophying due to surgical damage and post-surgery immobilization, it's best for recovery for the muscles to be as strong as possible going in. So diagnosis/surgery ASAP after injury, with muscles nearly at their pre-injury best, is preferred... if you suspect your ACL is torn see a doc quickly!)
Depends. An ACL tear can feel better on it's own after a few weeks assuming you don't go running into any hard direction changes. Many docs would prefer pre-hab prior to surgery in order to get maximum flexibility and strength for every patient, but most insurance will not pay for it.
I saw a doctor right away, but they still wanted to wait a month until ACL reconstruction surgery (cadaver achilles heal) so that all the mobility could be returned before the operation to help speed up the post op rehab.
For comparison, the full cost of a hernia repair (http://en.wikipedia.org/wiki/Inguinal_hernia_repair) in a private hospital in Poland is below $1500. Sure, this is a much simpler procedure than the OP's one, but still -- it involves an operating room, a surgeon, an anesthesiologist, assistants/nurses, and 2 days of hospital care. I don't imagine the materials are much different to the ones used in the US.
Even accounting for the lower cost of labor, the prices in the US are insane.
I don't know the statistics overall, but in my case the comparison of the inguinal hernia repair is even more damning: I'm positive it was more costly, but to add insult to injury, it (my hernia repair) was done as an outpatient procedure.
Although I am not a doctor (just a patient), if anyone tries to pitch you this as a good idea, run. The effective recovery time was insane, and not to mention the pain/temporary disability (also insane). An inpatient stay wasn't even offered, but in hindsight it shouldn't have even been optional.
By contrast, an unrelated abdominal surgery a few years later, despite being a much more involved procedure, had a much faster recovery. (10 day inpatient stay + probably 5 days of that with some physical therapy.)
Health care costs are a secondary issue to me, right behind health care quality. Unfortunately, I don't think either can be fixed unless they are entirely divorced from each other.
I'd be interested in seeing this analysis using what the actual final cost incurred was (normally the fees you are shown are negotiated down by your insurance company to the amount they actually pay).
I am actually 4 months out from my own ACL surgery, tore mine skiing and one thing the OP forgets to mention is many insurance will never pay that $60k as they have pre-negotiated rated with the hospitals and doctors. My surgery was done in SF (not the cheapest city in the world..) and according to the bill came out to just over 100k, but, my insurance paid 17k. What happen to the rest? Well I assume it was just inflated costs that the hospitals adds to the bill so the insurance can negotiate down.
This is amazing to me. I am from Australia and did my ACL when I was 15, and the cost was around $3000. It was an overnight stay in hospital, the only costs not incurred for the actual surgery and operation were MRI's and physiotherapy. How that could cost 20x the amount in America, I could not possibly fathom.
It is always a struggle for me to understand how health insurance is such a major expense in America, but when relatively routine surgery such as an ACL repair costs that much, things are put into perspective.
I had this exact same surgery 7 years ago after tearing ACL/meniscus playing basketball. Patellar tendon graft FTW! (I joke that real men donate their own tissues)
For me, the ACL has been perfect ever since. Wish I could say the same for my meniscus and cartilage - I subsequently tore my meniscus 2 more times (each time in a non-vascular area so they just sanded it down, no sutures like you had), and then 5 years later I tore a chunk out of my articular cartilage that had probably been weakened years before when I did my ACL.
That led to an OATS procedure where they took bone plugs from a non-weight bearing part of the knee and transplanted them in holes bored where the lesion was. That last procedure was pretty fun as it entailed 6 weeks on crutches, non-weight bearing, during which period my wife and I had our first kid (yay for timing!).
Anyway, that just to say hang in there (I imagine your rehab is pretty much over by this point, but it probably still aches?), and I hope your ACL graft (good call with the patellar) holds up as well as mine and your meniscus better. Oh and enjoy the achiness that comes with changing weather. I was rather amused that that apparently is a real thing. :)
As a side note, medical insurance much like construction is a 'cost-plus' industry. The insurance companies actually have incentive to make prices go up.
For example, insurance companies are required to spend 80% on medical expenses. So if cost of an ACL surgery skyrocketed $100,000 then, they would make $20,000 off of it. Instead, they only made about $14k off of Calvin's surgery.
I ruptured my left ACL during the final year of our college during a cultural fest (in India). It was a complete tear and required surgery to return to normal knee movement (Instability due to knee cartilages tears/injuries suck, and lead to further secondary injuries).
I had to differ my surgery for a couple of months since we had our final exams and I had to walk with a brace and avoid injury-causing activities. The surgery at one of the leading hospitals in the country cost me around ~$3000 and was completely covered by my Health Insurance, the care I received was exceptional and I could see why "Medical tourism" to India is on the raise. The costs are mostly around 1/10 of what any procedure costs elsewhere.
P.S. Incidentally, I had a freak accident a few days back and I'm positive I tore one (or many) of my ligaments in the other knee, and I had just started training to run a marathon within the next year :( (Lady luck hates my knees)
Interesting to read of a 'normal' person sustaining an ACL injury and the subsequent fixing thereof (especially detailed costing breakdown - thanks for the detailed analysis). There has been somewhat of an 'epidemic' of ACL injuries in the AFL[0] this year. So far at least 15 players, some of them quite well-known, have succumbed to a season ending ACL injury already[1], much more than previous years. The difference? They have access to a complete rehabilitation package of priority surgery and follow up physio program. Such is the professional sports industry I suppose...
I wonder how the cost would compare at a special-purpose orthopedic surgery center vs. a general hospital? I actually thought that otherwise healthy people are encouraged to utilize specialty facilities rather than hospitals as they can be optimized to the procedures performed, and may have lower risk of post-op infections.
$1,600? My Saint has had two TPLO's, which is the most common surgery for an ACL(CCL in canines) tear. Each Surgery was $5,000+. You got out on the cheap!
I doubt that has a significant impact on the cost of the procedure, though, right? I mean, sort of like replacing the clutch on a car -- the cost isn't (necessarily) based on the lifetime/quality of the new clutch, but rather the labor required to pull the engine, install the clutch, button everything back up.
I had my ACL repaired in 2007. I don't remember the costs any more, but I had essentially the same procedure using my patella and a meniscus tear repair. While I was able to put weight on my injured leg and was out of physical therapy after only a few months, it has taken several years to "fully" recover; even then I have the occasional gentle reminder that my knee is not the same as before my soccer mishap.
Here is an idea for an awesome law that might fix some of the problems with the medical industry! Remove the ability of the billing departments to determine who has insurance and who doesn't. That way, everyone is charged the same amount for similar procedures. The whole practice of over-billing insurance companies has simply become ridiculous.
Why do the insurance companies tolerate this practice?
I would like to pose a question to the Hacker News community. If you had to, where would you cut costs? Do you think doctors are paid too much? Or nursing staff?
Obviously, we think these services are overbilled but the reality of it is that most of these bills are not paid at all or paid for a fraction of what is billed.
I'd like to see the actual negotiated rate the insurance company paid for those items. I'd be surprised if it was more than 40%, and perhaps it might be less?
It's quite bad that those who can afford it the least pay the highest(sticker) prices, though. If Obamacare fixes that one thing, it's done the US health care world good!
The article ends with "this sector needs innovation". Even though it does, what it really needs is better (and tighter) regulation. The situation in the US (costs through the roof, a lot of people that can't get medical care), health is something that can't totally be left to the private sector.
In fact, in the link you provide, the 7559 euros also cover 75 sessions of physical therapy, a nurse coming at home every working day during a month and various drugs.
It would be interesting to have a global comparison (operation+therapy).
Here, the operation including all appointments before is about 5274 euros.
It seems to me that the balance of power has shifted far over to the providers and away from the insurance companies. Would allowing more mergers give them more bargaining power and bring these costs down? Or is that just too simple?
> It seems to me that the balance of power has shifted far over to the providers and away from the insurance companies.
That's because you are looking at an accounting of the nominal charges, and not what the insurance actually paid. If you look at what the insurance actually paid based on those nominal charges, you'll see that the balance of power isn't where you think it is.
Oh yes it is! I know exactly what my insurance company's negotiated prices are (because I pay them!) and they are astronomical. I just had an emergency visit and the nominal charge was $1700. The negotiated charge was $1500. That's _nothing_. I added up the medicare schedule prices for the entire visit and it was about $350. So, yes, a large insurance plan (like medicare) seems to be able to negotiate far better than my insurance company.
There is a lot of cultural resistance in the US to any kind of price pressure on health costs. This problem will exist regardless of whether you have a private or government system.
The medication costs, especially the fluids, are much higher. I checked a UK pharmacy for costs for buying small amounts so the discount they get for buying in bulk suggests a very large mark up in price.
Did you include the cost of having a trained medical professional administer them? The cost of hospital aspirin isn't the pill it is the doc deciding to give them to you and the nurse who dispenses the pills( don't forget the billing person who charged you for the pills, the staff lawyer who was retained just in case you sue over the aspirin, and the payout to the last guy who sued and won).
As with every service industry from the local pizza joint on up COGS(Cost Of Goods Sold) is one of the smallest parts of the pricing puzzle.
If you read the recent Time cover story about medical costs, you'll see examples of people being recursively double-billed for items, at least according to the Medicare guidelines. e.g., and my memory's a little fuzzy on the specifics, but I believe one case was being billed for the operating room, then billed for the prep kit (which is supposed to be included in the room charge), then billed for every individual item in the prep kit.
If I hire a contractor to do something and he charges $X/hour, I don't expect him to mark up the materials he might use, too. I'm already paying for his time and expertise. I shouldn't also be paying the drywall for his expertise.
Hard to tell from the post, there was zero mention of staff costs besides the surgeon and anesthesiologist. So they fit in to the bill in one of two places equipment\drug cost or facilities. My guess is some of both. Time spent changing iv fluids is probably covered by the iv fluid line item vs time spent changing sheets being part of the facilities line item.
There is a cost in not getting your ACL repaired. I waited 4 years (due to the fact that the buffoon physios / doctors I saw didn't diagnose it correctly) and put on 20kg in the interim because I stopped playing sport.
Coming from the mobile app market where consumers are reluctant to spend 99 cents on your app/game, this is revolting.
Something has to be done (in the medical field and in the mobile app field as well)
I've heard from someone who was involved in this that sterilizing medical equipment that you can't autoclave is seriously non-trivial.
And certainly not free, nor is autoclaving, including the inevitable human errors that will result in incompletely sterilized equipment, plus there are all sorts of tradeoffs made here. I'm just old enough to have had glass syringes used on me, they're thick, heavy and obviously much more easily broken, which is less than ideal for taking blood and the like.
One other advantage of disposables: you can more afford to stock up a lot in case you need to surge after a disaster, they'll get used in the normal course of operations. Whereas the reusable stuff is generally/always? more expensive up front.
Okay, but for various sharps, blades and other cutting tools, keep in mind that repeatedly heating and cooling innately dulls them. Taking metal through temperature ranges that result in expansion and contraction mess with the honed edge. Think about metal as if it were a malleable wax candle.
Not to mention that mere pressure against skin on a cutting edge effectively bends and dents the edge until it becomes dull. That's what happens to IV needles, just the pressure to pierce skin alone ruins the point. How many times do you get to re-use a safety razor after shaving your beard or legs/armpits? Was the activity really very stressful on the blade?
And yet, maybe you'll get 5 passes (with a multi-blade razor on a thick beard) before it's pulling at the hair and skin, and you notice it's painful to shave with.
So too with surgical tools. After so many cycles of cutting, then heating and cleaning, you're pressing a dull butter knife against skin and whatever else you're cutting, relying more on cutting by sheer pressure than using the sharp edge to separate the tissue.
And then you can't stop the bleeding because the cut was wrong, the patient dies, you get sued (you DO get sued), and maybe you lose your license, reputation, time and money. So balance it against, just buying a $900 object brand-new.
But, yeah, how about sharpening them again? But with what? An angle grinder plugged into an extension cord? A stone wheel down in the metal shop? Not quite... I really don't know all that much about cutlery, but getting a blade perfectly sterile after sharpening it is probably something that is best done by automated factory machines, at which point the blade may as well be new anyway.
Why are they $900 in the first place? Seems like about an order of magnitude more than any reasonable cost. It's not like it's that rare of an item, there are ~100k of these surgeries performed annually just in the US.
It's very hard to be sure of removing all viruses and prions from a surface... especially if that surface is porous or worn-down from any use.
Deep, long superheating might do it... but that itself can wear or destroy many materials, and the item would need to be kept in 'like-new' sterilization until next use.
Hospitals might not be the best place to try to do that; in 2002 there were about 30,000 deaths in the US due to hospital-acquired bloodstream infections, per the study referenced at:
Some do, and it appears he was only billed for the ones that don't. For blades and other sharp things, it's probably cheaper to just use new ones than to have the equipment and staff to sharpen old ones. Some of the other stuff, I suspect, isn't autoclave-able, which is the standard for sterilizing surgical stuff. That pretty much precludes reuse of plastic things, for example.
> Would they not be able to just be disinfected and resealed?
Blades that need to be very sharp and of very particular dimension are going to need sharpened, which is going to change their dimensions. So there is limited, if any, reusability in any case.
And the keeping, transporting to a cleaning facility, cleaning, sharpening, etc., is going to come with an additional cost cost and risk of accident that you don't have with immediate disposal.
I had ACL surgery in November in Italy and it costed 2200€(I did not pay anything we have public health care luckily).
US health care system is just crazy in my opinion.
> Going in, I had anticipated that doctors would take the lion’s share of the costs. I was surprised when the facilities ended up being the dominant cost; over 40% of the total.
Is that because you're paying for the cost of nurses here, rather than breaking that cost out elsewhere?
> This centimeter-wide cutting machine cost $900 according to the price sheet.
That seems to be a bit much. I'm used to silly prices for tools and equipment in electronics, but still. Perhaps they're charging you for the whole tool, and not just the disposable blade? (Which would seem to be a bit cheeky.) Have you tried to get a price quote from anywhere else? (http://www.arthrex.com/products/AR-2285-10) Because they sometimes turn up on Ebay (http://www.ebay.com/itm/Arthrex-AR-2285-10-Parallel-Device-1...)
> but the blades get thrown out after just a single use
One reason for that, at least in the UK, and maybe this is historical, is because of diseases like CJD.
But as ISL said a sharp blade is a good blade and when you're slicing people you want the best blades you can get.
> Most of the other drugs cost between $40-60 per dosage.
In England everything is free at the point of delivery. Medications are a bit different. If you're in hospital they're free. Most people get exemptions from paying. The people who do pay need to pay about £7.50 per line item per month. There are discounts for people who need a lot of meds.
> The screws and washer are made out of titanium. I haven’t had any problems with MRIs or the metal detectors at the airport, but they do show up very clearly on my x-rays:
When my father died he had left me his artificial knees in his will. Luckily he had also asked to be cremated, so it was nice and easy to get them.
What I'm particularly curious about is why this market doesn't seem to work.
Insurance companies want customers to pay them. Insurance companies don't want to pay too much to hospitals because that's cutting the margins. So why don't insurance companies seem to be driving the costs down? Are insurance companies equipped to investigate the costs reported by hospitals?
Some kind of anonymised crowd-sourced data would let people know if their operation was around the same price as other people were paying. Perhaps you'd need to break the price down so people were able to compare similar things.
I hope your knee heals well and that you start to feel the benefit of that surgery!!
> So why don't insurance companies seem to be driving the costs down?
They are driving down costs -- as the OP mentions elsewhere in this thread, while he was billed nearly $49k for facilities/equipment, the insurance company only paid $15k.
There certainly are a lot of rich doctors and hospital executives who are being paid ludicrous amounts of money (especially considering the hospitals themselves are billed as not-for-profit), but the insurance companies are making money hand-over-fist in the current regime.
The easiest way for insurance companies to drive costs down is to find technicalities to not have to pay at all for the most costly ~.5% of their customers and stick them with the bill.
this is an amazing article for me since I also tore my acl and am considering getting the reconstruction described in the article done, any one out here who recommends/ does not recommend this ? I am developer with a 9-6 desk job and usually go jogging rarely and don't find time to work out due to a busy schedule
If you don't plan on playing semi-competitive sports ever again, I wouldn't recommend surgery. It's all about the planting of the foot and changing direction, which you don't do with straight line activities like running or biking.
Forget about working the first week after surgery. You need to elevate and extend your leg constantly for the first few months, which gets uncomfortable when sitting.
Pre-surgery you need to strengthen the muscles around the knee to speed up recovery, so my physio got me to go to the gym 3X a week for two months, biking hard. Post-surgery you need to use some gym equipment as home rehab doesn't cut it.
Also it takes two years to fully heal. After seven months I could hike and bike, but now I'm sixteen months in and only now have started to play light competitive sports again. However mine is more complex as I have torn miniscus and some residual scar tissue that may be removed in the future. Let me know if you have other questions about the process, it's a long one!
great presentation and vibrant discussion. I wonder: how much attention does this article owe to effective use of highcharts, a clean palette, and freight sans pro? Not knocking, just wondering.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Like the OP I had meniscal tearing too so more or less directly comparable. (Although obviously 8 years is probably a long time in medical devices so worth bearing in mind).
To put in perspective, that is approximate the same total cost (~$5000) as just _one_ of the pieces of equipment ("Cannula Fast Fix CVD") that the OP lists.
It's one thing if doctors are more expensive because they have to carry higher insurance charges to protect against negligence lawsuits, etc, but that the equipment alone is multiple times the cost seems crazy.
Mental.