We’ve been on the road to this for a while, and it’s so exciting to see. I switched to injectable prep a few months ago to avoid having to take a daily pill - it’s an injection once every two months, and my doctor told me that the guidance might soon change to once every three months.
It sounds simple but for a lot of people it’s not a trivial thing to take a pill every day or adhere to a strict appointment schedule to get an injection. I’d imagine that adoption & compliance goes way up if it’s that much easier.
I have been debating on switching to the shot but Havnt yet.
Just to avoid the accidentally missing a dose or the chance interactions (lower efficacy) with dairy and many fiber supplements, this would be amazing.
Would be nice to never need to worry about that or think, hey I missed a dose is it actually true that it doesn’t matter or do I need to wait a full week. Half a week?
My only concern here though, if it’s in your system for 6 months what if you have an adverse reaction or just some unpleasant symptoms.
I'm going to assume a bit and for that I'll apologize in advance. I'm assuming you're in a high risk group for HIV. Why not just use condoms? Is it because they aren't 100% effective?
Why not just save money and not install those ECP brakes on your vinyl chloride freight train?
Why not just use one unshielded Raspberry Pi on that spacecraft instead of a 3-of-5 quorum from the output of 5 identical engineered-for-space systems?
Using/requiring condoms AND being on PrEP helps me live my best life with less fear-based inhibition and cognitive load.
It is. I interpreted the parent post as a neutral question, and I intended my reply to involve playful analogizing. I'm sorry that it didn't reach you as such through the side-channel-impoverished medium of text.
Also this is wrong. Most people I know use multiple versions of birth control. Access to the morning after pill and abortion is a form of birth control. Being on the pill and also using condoms is common.
While that might be true for "most" people, plenty of people do still use multiple forms at the same time - including people who do not engage in a lot of casual sex. But lots of people also do have lots of casual sex, and that is a choice they have every right to make.
It’s not that complicated. A lot of people don’t like condoms, either wearing them or having a partner wear them. PrEP, to many, has rendered condoms unnecessary.
A lot of people out there have managed to get past stigmatizing STIs, viewing bacterial ones as no more remarkable than sinusitis so long as they get tested and treated.
Between PrEP and vaccines for hepatitis and HPV, risks for the scariest STIs can be annulled, outside of exceptional, treatment-resistant cases.
Why not just not have sex unless trying to procreate? It's amazing in 2024 this line of discussion is happening.
We all know exactly at a individual level what to do and not. We can keep asking "Why not just use a condom?" and see how far that gets us, or actually understand psychology and use patterns and work with what people actually do (good or bad).
Same can be said about (illicit) drugs, why not just not do drugs? Simple!
It is a well known fact that people (except incels & asexuals) will have sex whether you like it or not. It's part of the human experience. Policy must deal with the real world.
You don’t, but people do. And even if they “shouldn’t,” the cost of contracting HIV—which very few people set out intending to do—adds up to an eyewatering sum over a lifetime, no matter who’s paying for it. Not to mention rendering someone, often young, dependent on heavy drugs to stay alive. Forever. Assuming the drugs remain effective.
What other risky lifestyle decisions do we advocate to punish that severely? Especially when the technology exists to ameliorate the risk?
Wouldn’t it be cool if simulated guns were as fun as real ones? Then your hypothetical person could get drunk and shoot guns all they want, and there’s no problem anymore! So what’s the virtue in leaving the real loaded gun lying around to test their willpower?
When all it takes is a daily pill, or an injection, to reduce the risks of drunk-driving a motorcycle to practically nil - wouldn’t you want to do it? You don’t even need to wear a helmet, you can just do whatever on your motorcycle and not worry about it.
You never have to think to yourself “hoo boy I’m at two beers, and I don’t know, should I have the third? Will that be too many? Am I going to need to get on my motorcycle in an hour? Or will it be more like three hours? What will my blood-alcohol level be at that point? Is this legal? Is this safe?”
You can just have fun getting fucked up and driving your motorcycle.
Modern medicine has given us this incredible thing, and you’re really going to be like “Naw I don’t know about all that.”
> Modern medicine has given us this incredible thing, and you’re really going to be like “Naw I don’t know about all that.”
I think that the only actual complaint I've ever heard against Prep is the costs being socialised and covered solely not by the user (ie insurance or public healthcare or whatever). It is (was?) not cheap!
i'm confused. are we acting like we don't full-well know that using a condom sucks for everyone involved? it's like wondering why people didn't like using a face mask during covid: because it sucks. that, of course, is independent from whether it's prudent, but if something sucks, it's no surprise when people avoid it, right?
> are we acting like we don't full-well know that using a condom sucks for everyone involved?
What do you mean "acting"? We all know it reduces the sensitivity. That's the trade off. You feel less pleasure, and your fucking doesn't get to kill you.
> it's like wondering why people didn't like using a face mask during covid: because it sucks.
Similar analogy. It sucked, but that was a similar trade off. It sucks a bit, but there's less chance it'll kill you or you'll kill others.
> it's no surprise when people avoid it, right?
I think those people would have to be fucking morons, but sure, morons exist.
People have a risk level they're comfortable with, and sometimes people feel added excitement pushing right up to or past that level, and sometimes they're just happy to pay extra for something they feel is within that risk level if they enjoy it more.
We all choose to take risks all the time and often pay for the privilege, sometimes explicitly seeking out the thrill of a risk.
I'm guessing what makes this specific scenario weird for you is more likely that this risk doesn't seem worthwhile to you relative to what you get from it (and I agree with that - I've never had an appetite for taking risks with STDs)
Being horny also counts as being “in an altered state of consciousness that biases against use of condoms.”
As someone who took the condom off in a risky situation recently, there’s no comparison between the on and off feeling. It’s like licking a piece of candy vs crushing it with your teeth and sucking it all at once.
Maybe you want the real thing. I get that, even though I have never had sex with a prostitute or fall into the risky sex category. I'm not going to go as far as to be childishly disrespectful and say I'd rather die doing the real thing, but I do understand the apprehension of using artificial barriers during the most intimate act know to humankind.
When somebody else takes a risk for you, you have to pay them more than if they are not taking a risk. We pay soldiers more when they are at war than when they are not. People who want to raise money by selling bonds have to pay a higher interest rate if their credit is worse. Etc.
Prostitutes would consider unprotected sex more risky, and thus charge more.
A better analogy would be to buy a '60s sports car that predates nearly all modern safety tech at auction for $$$$$$ instead of just buying a 2024 Corolla with modern safety features.
This is obtuse. The intent of expressing that if you are paying someone else for a service, it predisposes them to demand a higher price if you're asking them to take additional risks if they have any negotiating power at all was pretty obvious.
The comment above the one you replied to was. The comment you replied to was not, and it'd be reasonable to suggest it didn't really address what it replied to. But its intent was clear.
Besides the other nice reasons people offered, because "stealthing" (when someone removes a condom during sex without the other person's consent or lies about having put one) is remarkably common, and not as easily noticed as you might expect.
Condoms are less effective at HIV prevention, but also they’re unpleasant and don’t prevent most STIs because of oral sex. Nobody’s giving or getting head with a condom. People who stay on top of preventative measures tend to not bother with condoms since PrEP became prevalent.
Preventative:
1. Gardasil 9 (vaccine against 9 strains of HPV, prevents genital warts and cancers caused by HPV)
2. Monkeypox vaccine
3. Meningitis ACYW vax
4. Meningitis B vax (35% effective against gonorrhea)
5. doxyPEP (two pills of doxycycline taken after sex, 90% effective against syphilis, 80% chlamydia, 50% gonorrhea)
6. PrEP (prevents HIV infections)
7. and the usual suite of vaccines against the rest like hepatitis A/B, mumps etc
Treatment of the bacterial ones (which transmit through oral too):
1. syphilis - butt shot of penicillin
2. chlamydia - 1 pill of an antibiotic
3. gonorrhea - a week of doxycycline pills or one butt shot of ceftriaxone
Remaining: HSV. Half of the population has it, so no big deal. Condoms dont prevent it either.
As for hepatitis: even though it requires blood contact and as such is not necessarily considered an STI, hepatitis c is curable these days thanks to DAAs taken over the course of 8-12 weeks. a/b have vaccines.
> 5. doxyPEP (two pills of doxycycline taken after sex, 90% effective against syphilis, 80% chlamydia, 50% gonorrhea)
Preventatively using antibiotics is a horrible idea, for one it increases the risk of creating resisitant strains, and we are already running out of antibiotics (especially broadband ones). Moreover, antibiotics in general are known to mess with you gut biome whose importance we are just beginning to understand (we know it plays a role in many physical and mental illnesses for example). Then there are the side effects which for doxycyline include diarrhea, increased risk of bowel cancer, higher sensitivity to the sun (and associated risk of skin cancer).
This all feels really general—precipitated on the idea that there’s one Right Way for everyone to use these drugs, about which the doctors and public health professionals recommending doxyPEP are somehow uninformed.
Suppose you’re immunocompromised. Wouldn’t it be worth the diarrhea to avoid infections your body couldn’t fight off?
Suppose you’re in a situation where you’re having lots of opportunities for infection. Whether you can or can’t control that situation, the end result is the same: you know your body is going to be challenged by infectious disease frequently in a way that most people’s bodies aren’t. Isn’t it plausible that the infectious agent may have less opportunity to evolve if you didn’t contract it as frequently?
Different forms of therapy might be both individually and collectively optimal for people in different situations. What’s right for a person who isn’t at risk isn’t the same as what’s right for a person who is at risk.
Thanks your professional healthcare research expertise will really come handy to all the researchers studying effects of doxypep and routine anti-acnne doxycycline prescriptions.
The people responding to this seem to assume you’re doing so for funsies, which might be true. But that’s not what you said. So for their benefit, it’s worth pointing out that daily doxycycline is a pretty normal therapy for a range of chronic stuff—malaria prophylaxis, rosacea and skin that’s prone to infections, I’m sure there’s more.
If loopdoend’s doing this, it feels like a good bet that there’s a doctor in the mix judging that it’s medically appropriate for them.
This is really surprising to me since there is a lot of evidence that oral antibiotics can mess up your gut flora, creating all sorts of bad side effects. Do you have any digestive issues?
In the early days of AIDS (wasn't called HIV back then) the recommendation was to use a condom or dental dam (depending on the hardware of the recipient). That's how I learned what a dental dam was. Later it was suggested that plastic food wrap would work (the jokes just write themselves).
Sadly the ubiquity of paper toilet sheet covers in US bathrooms dates back to the 80s due to straight paranoia over AIDs + widespread and overt anti-gay prejudice, so every time I see one of those dispensers I grit my teeth.
Reminds me of the early days of COVID (not the anti-gay part, but the weird practices when nobody really had yet a good theory of what's going on).
HIV (human immunodeficiency virus) is the virus, AIDS (Acquired Immune Deficiency Syndrome) is the syndrome caused by untreated HIV. Everybody with AIDS has HIV, but not everyone with HIV has AIDS.
The reason for the reversal in terms is treatment options. When HIV was first found, there were no treatments so AIDS was inevitable. Nowadays, medication can permanently prevent HIV from progressing to AIDS, so AIDS is much less common than HIV.
> In the early days of AIDS (wasn't called HIV back then)
You might be thinking of “GRID” (gay related immuno deficiency), the original name of AIDS when it was believed it only affects gay people. Once the virus causing the illness was identified it was called HIV.
Although we have to admit the moral hazard element too: by altering the risk calculus, it does seem to have helped weaken cultural norms around condom use and risky sexual behavior. Business is booming for bacterial infections.
Personally I’d say that’s a pretty good tradeoff: fear, stigma, and death for a different problem that’s more an annoyance than a mortal threat right now.
I think another overlooked portion is that we shouldn't be using meds (for infectious diseases) to enable fun (which seems common with sex). Eventually those meds will lose effectiveness, that's just evolution. Then the people who really do need them will be out of luck.
https://pubmed.ncbi.nlm.nih.gov/9141163/
1997, "reexamination of HIV seroconversion studies suggests that condoms are 90 to 95% effective when used consistently"
...And your odds of making it through that pharma-minefield with zero side effects are not encouraging.
Worse still--large scale casual sex is a great way to introduce new, novel and un-contemplated STDs into the population. STDs are opportunistic that way, just ask Mr. triple-resistant Gonorrhea.
It's decidedly not the way I want it to be, but that's just how it works. For casual sex to be safe I think its more like "Hi, please spit into this tube so we can get busy" and red means HIV, Green means Monkeypox, comprehensively.
It's not just about casual sex though is it. There are many people in long term monogamous relationships with a partner who has an STD, but who don't want to catch it themselves. Vaccines and medications can allow them to have active sex lives while staying healthy and in some cases even help women go through pregnancy and childbirth while preventing the spread of an STD to the child. For these people minor side effects (and at times even more severe ones) can be entirely worthwhile.
Or perhaps maybe a future for occupational health. My wife is a nurse. Needle sticks happen. When it does, she has to get tested, full works. The hospital pays for that and the treatment. Maybe with a shot that lasts a year rather than the current 2-3 months(?), hospital staff can just opt that route then the test and treatment. Apparently the treatment is rather gnarly.
The odds are perfectly fine lol. If you think spitting into a tube before sex is preferable to being immune, I think you have a huge misunderstanding of casual sex
I looked through the literature and it seems that condoms are quite effective at preventing HSV infection when used, especially from male to female (on the order of 99%), and less so for female to male (around 60-70%). I would suspect the reason for failure is behavioral. People probably don't apply the condom until after most of foreplay is over and HSV-2 can be transmitted during "outercourse".
HSV-1 and -2 transmit through contact from skin location to skin. Including through asymptomatic shedding. Only sometimes is that location covered by a condom - in location and in timing.
See also: Wrestlers' "Herpes gladiatorum" which is just HSV-1. Which demonstrates how HSV-1 survives for transmission far more easily or broadly than just genital contact. Is there "HSV-2 gladiatorum"? Apparently it's usually HSV-1 but probably yes - neither HSV-1 or HSV-2 are really location specific.
The vaccines are just common sense for everybody. If you’re worried about “putting your body through” vaccines I suggest asking yourself what exact you are worried about on a molecular/cellular level. PrEP blocks HIV’s transcription to DNA so that it can’t take hold - it is cleared by your kidneys like a zillion other molecules in your body. DoxyPEP is the most broad acting, and least popular, item on the list.
Why not just not have sex unless trying to procreate? It's amazing in 2024 this line of discussion is happening.
We all know exactly at a individual level what to do and not. We can keep asking "Why not just use a condom?" and see how far that gets us, or actually understand psychology and use patterns and work with what people actually do (good or bad).
Same can be said about (illicit) drugs, why not just not do drugs? Simple!
Condoms aren't perfect, and PrEP is cheap and has basically zero side effects. Plus, rapists don't use condoms, no matter how nicely you ask.
Edit: lmao touched a nerve? I will never understand why folks here get so prudish when we talk about sex... "Just wear a condom!" is remarkably insensitive, as though 100% of HIV transmission is your own fault, and not, say, someone else who has bad intentions.
Some of us prefer to enjoy sex as a beautiful act of human connection and condoms detract from being in the moment of joy.
This is like saying to someone killed in a motorcycle accident why didn’t you use a car. It’s a reductive, unempathetic and frankly unproductive take. Please think before asking this again.
I think the GLP-1s are subcutaneous injections - tiny, tiny needles you can stick in a variety of locations - Apertude is intramuscular, it’s a much larger needle, I’m guessing there’s some level of skill involved.
I get an intra muscular injection of testosterone every two weeks and it's true that it's not as easy as a sub q injection would be, but it also definitely doesn't require a nurse.
there's a few good injection sites (upper arm, buttock, thigh or even pecs) and after I was shown once how it's done, I can do it myself. it's also essentially painless.
Off topic, feel free not to answer if it's too personal but I'm curious how is every two week injections working for you for Testosterone? Are you on TRT for Hypogonadism or is it something else? I haven't heard too many people be on that kind of protocol..
I'm Hypogonad and I'm on self administration of sub q injections twice a week and it's quite annoying. My urologist told me it's best to split it this way since more frequent injections avoids a "crash".
I would like to have less frequent injections if I could!
It depends on the exact type of Testosterone being used. Each type has a different half-life and absorption profile.
The most common - Testosterone Cypionate should be best used twice a week to avoid the "crashes" - if you care about keeping your levels relatively stable. Other forms of Testosterone have different half-lives and should be taken at differing schedules.
I never saw the point in subq shots for TRT. They are less effective, and are recommended solely for patient comfort and compliance. If you can manage a twice-weekly deep IM injection, I personally have had great results with that once I learned the locations. Nearly as painless as subq and better more consistent results.
Overall it doesn't matter a whole ton unless you are doing it for specific performance enhancing reasons. Being off "optimal schedule" a few days isn't going to make a meaningful difference for most.
Both graphs are 200mg per week. Green is dosed at once every 7 days, while the blue is broken into 7 smaller doses per week. (I haven't included axis and such, because it's really just the shape I'm trying to highlight)
As you can see, more frequent dosing results in steadier levels.
When administering your testosterone once per week, you will have to make one of a couple trade offs:
1) Dose high enough that you are above the level you want to be by the end of the week. This avoids the "crash" you mention, which will consist of both low-testosterone (low-libido, fatigue, etc) and low-estrogen[1] (joint pain, etc) side effects. Dosing higher means you shift the whole graph up, and you will be at supra-physiological levels of testosterone and estrogen, and the high estrogen side effects are no fun: nipple sensitivity, emotional fluctuations (think crying at the sight of puppy pictures), gynecomastia (development of breast tissue), horrible back acne, etc.
2) Dose on the lower side to avoid avoid high testosterone/estrogen side effects. This shifts the whole graph down, and now you're below where you want to be by the end of the week, and you now feel more like you did before you started TRT.
3) Somewhere between the above two options, and add an aromatase inhibitor (like anastrozole) to minimize high estrogen levels. You'll still have excessively high testosterone though... and you'd really be better off avoiding the high testosterone peaks instead of adding another drug to the mix.
I used to go into a clinic once a week for an intramuscular injection of testosterone cypionate. In order to not feel like shit the last two or three days of the week, I had to up my dose such that my back broke out in a constellation of acne, and probably negatively impacted my health in other more meaningful (but less obvious) ways.
Now I inject testosterone propionate every night. I managed to lower my dose so that I'm always hovering right around where I want to be, instead of bouncing all over the place.
That's another benefit of increased injection frequency: you can lower the total amount of testosterone injected per week while staying within therapeutic range.
1: Your body produces estrogen by aromatising testosterone. More testosterone and/or more aromatase -> higher estrogen. Less testosterone and/or aromatase -> lower estrogen.
This is true generally in pharmacology, but the plasma concentration of the androgen esters (prodrugs) isn't a good measure of "active" testosterone in your system. Thus the graph is a bit of an exaggeration. Basically, as long as the slopes are the same (rate of breakdown ≈ rate of prodrug conversion), you'd get ~same plasma levels.
Ideally they'd break down at a constant rate (they don't, but close enough) leading to steady levels despite levels of the prodrug steadily diminishing. This makes once a week dosing of testosterone cypionate (for example) viable for many, but not all, as you've discovered.
Dosing less but more often helps minimize the uncertainty/variability in breakdown/conversion, thus being more reliable at the cost of convenience.
A lot of these medicines that require patients to inject themselves come in a self administrating auto-injector. There are really simple to use, I mean literally anyone can inject themselves, then throw the one-use auto-injector out.
My doctor’s office handled the insurance approvals once I told them I was interested in switching me off oral PreP. I go to a pretty large practice that specializes in working with LGBTQ folks and one of the big advantages is they tend to be pretty good at figuring stuff like this out quickly.
Agreed, it’s another treatment in a continuum of adherence— pre relations testing, barrier precautions, daily pills, semiannual injections. All running up to the eventual asymptote of cure and eradication.
Oh, as someone from the rainbow community I didn't even know we'd progressed to that yet. I was still taking a big blue pill when I needed to, then sticking to the number of days after as well. If it's every two months I'm so gonna look into it.
I briefly did some work with an HIV research organization in South Africa.
One dynamic I was shocked to hear was the prevalence of marriages where one partner (always the husband in this context) is HIV positive and the other is secretly on prep. In this context infidelity may be a norm and traditional cultural and gender norms may look negatively or skeptically at anti-retrovirals.
While this isn’t the majority of the HIV experience in South Africa, it’s certainly a sizable group.
Further, adherence more generally is a massive problem. The cost of travel to a clinic in both rural and urban settings can be prohibitive for many and cause major adherence drop-off.
Drugs like this, if made affordable, will go a long way to immediately easing pressure on these groups - and that’s exciting.
You’re implying that the prep and HIV are known internally to the marriage but secret externally? That seems unlikely. Taking medication in private does not seem to qualify as a “secret” to me
We are used to a western perspective on marriage, where the playing field is generally level between partners. In Africa, there is often a huge power imbalance between men and women in marriage. A woman particularly might want to keep her prescription status a secret because it suggests that she might be cheating on her husband. Even though it may seem obvious to us in the west that taking medication to avoid contracting HIV from our spouse is an obvious and reasonable thing to do, in Africa, it would be more culturally acceptable for the wife to remain vulnerable to contracting HIV from her husband because that would also infer that she is not sneaking around having sex with other men.
From the perspective of the husband, the woman taking prep implies she is cheating. He either doesn't get tested or doesn't care, it's more important that she not do the thing that implies she could be cheating than that she not get HIV, and that she be sexually available to him.
You're digging for a logical explanation for a fundamentally illogical cultural problem and you aren't going to get it.
No, that doesn’t make sense. And writing it off as an illogical cultural problem is just lazy. I’ll believe these guys are assholes. I don’t believe they’re just consistently idiots. If the men refused to acknowledge that they had HIV and refused to allow their wives to get prep, then the logical consequence is that the wife gets HIV and the men are forced to confront the fact that either the husbands themselves have HIV or the wife is cheating and got it from someone else.
It seems much more likely that the husbands refuse to allow their wives to get prep out of spite. The implication of infidelity angle does not feel plausible.
Otherwise the men are setting themselves up for a lose:lose scenario regardless of what the wife does.
"the men are forced to confront the fact..." No they aren't, they simply never confront it. People go to their graves denying that they have HIV, denying that they ever tested positive, denying that a positive HIV test has anything to do with illness.
"Otherwise the men are setting themselves up for a lose:lose scenario regardless of what the wife does." - Of course.
I mean, the most rational win:win thing to do is to get an HIV test and get treated if positive. They then both don't get sick and die and can't pass along HIV. Many people don't do that either. What's the mindset that explains this behavior? You can't work backwards from the most rational thing to do to what people actually do.
You are the one injecting this narrative about women cheating though. It seems to me you’re just making this up. It doesn’t make sense.
Establishing the narrative that if my wife gets HIV that she must be cheating on me is a losing proposition for the man that only increases the probability that his wife will appear to be cheating. There is no motivation for it.
Simply being a dick and saying women can’t use prep because I don’t want them to is a much simpler narrative.
Your reasoning here is similar to arguing they’re a stupid people ergo they don’t use prep because of aliens. It’s not compelling even if you’re willing to believe they may engage in irrational behavior.
You asked "why would someone hide prep", you got one example. It is by no means an exhaustive list. For example, a big fear is being perceived as having HIV (since prep drugs are also part of HIV treatment).
If you do actually have interest in this topic you could read about it:
"Men were able to initiate PrEP without discussing it with their partners, whereas some women said they needed to get permission. Discussions around starting PrEP could raise questions about trust and infidelity and act as a barrier to PrEP use."
Well, you have an anecdote from someone claiming to be from SA saying that’s culturally the perception. Here’s a summary of research [1] on the topic concluding similar reasons (among others):
> Several participants felt that they could stop taking PrEP when the need, as they saw it, had passed. Often this was to do with the nature of their current relationship, for example with a person regarded as unfaithful: “If I find someone that I will be in a relationship with and if he is not faithful, or I have started being unfaithful, then I will come back and get them.”
And
> On the basis of these findings, the authors suggest that take-up and continued use of PrEP is likely to remain subject to established social norms. These norms often relate to gender and they determine, for example, who decides what HIV prevention methods to use, and the extent to which a woman in a relationship might – or might not – be able to make and implement such choices.
Just because something seems logical to you, doesn’t mean that social norms and pressures don’t superseded it. In fact, we even see it in our own cultural with people believing vaccines cause autism, the whole belief that ivermectin cures COVID-19, or flat earthers. What’s really impressive though is you having such a problem with this idea despite overwhelming objective evidence to the contrary being available online and people telling you their lived experience on this very website and you significantly discount the very real possibility that people can be illogical in their strongly held beliefs even if it seems nonsensical to you. If you know nothing about a subject, you’re likely to believe what all your peers tell you which is how misinformation gets a foothold. This misinformation can even come from nowhere. The point is that if enough people believe it, they can get others to believe it to. That’s literally how human belief systems work where beliefs spring out of nothing.
Your first quote is saying the opposite of what you are trying to defend. It’s about women taking prep because they believe their husbands are cheating, which makes total sense.
Not HIV husbands forbidding their wives from taking prep because it would enable the wives to cheat or imply that they are cheating
The point is that in the scenario being described, where the woman feels she needs "permission", the man's perspective is... if you were taking this, what does that say about ME? What does that say about what you think about ME? The decision would be about him, not her. How could it be about her? Wait, if it's not about ME, who else do you need this for? MY wife would never need such a thing.
It is easy to avoid stigma and shame through denial. The woman would be well aware that he would not approve such a thing and would take it in secret.
I mean you literally have women saying they take it if they are cheating.
> Some of the women were prevented by their male partner from taking or continuing PrEP: “I showed him the pill. He immediately stopped me from saying more before mentioning he had heard about PrEP and that he was strongly against the pill... He ordered me to throw them away or else pack my bags and leave. And that was why I stopped taking them.”
Here’s some more explicit quotes [1]:
> Another concern was that partners would interpret PrEP use as evidence of sexual activity outside the relationship.
> “I didn’t tell him about the pills. I was hesitant because he will say, ‘Why are you preventing HIV? Are you cheating now because we don’t have HIV so why are you taking pills?’ So, I decided to keep quiet. I am going to tell him. But for now, I haven’t told him about it.” PrEP User, Lower adherer, Age 21
It even makes sense that your partner taking PrEP would be seen as evidence of having an affair if you are convinced that neither of you had HIV prior. So not only do you continue on doubling down on a losing position, it’s not even an illogical line of reasoning to have.
I’d say the burden of proof is on you at this point that such an interpretation isn’t a social norm or that it’s even an illogical position to have.
Could you fucking not? I’m asking a question because I don’t understand it. You don’t need to try to shame for not knowing something and trying to learn.
HIV/AIDS dominated my high school years; it was just starting to become known; the first reported US case was in 1981, and in 1983, the disease (AIDS) was traced to the virus (HIV). My biology class had a poster of all the things AIDS could present as (kaposi's sarcoma, etc). At the time HIV was effectively a death sentence and it really affected places like SF heavily.
One of my main motivations in college and grad school was to work in drug discovery, specifically for HIV. At the time (~1995-2000) we were just starting to see positive results from protease inhibitors and reverse transcriptase inhibtors came somewhat later leading to the current "managment of HIV through HART" https://en.wikipedia.org/wiki/Management_of_HIV/AIDS
All of this came slowly - decades between significant new technologies/improvements in treatment. many sources of infection such as blood transfusions are now much less risky (people in the 70s and 80s were getting hep C and HIV from blood taken from HIV-positive donors). And the disease presents very differently in the US vs. other areas such as Sub-Saharan africa. But with extensive effort, prevention has gotten better and treatments have gotten much better. If there are truly usable preventatives for at-risk populations, and those medications are affordable, it will be a huge boon to the recipients.
Some interesting things to note:
- there was a lot of controversy about the source of infection and a lot of people used this to criticize gay people and injected drug users.
- one of the world's most famous virologists, https://en.wikipedia.org/wiki/Peter_Duesberg actively denied that HIV caused AIDS and instead thought it was transmitted by drug use. Note "Duesberg entered a long dispute with John Maddox, then-editor of the scientific journal Nature, demanding the right to rebut articles that HIV caused AIDS." which I think presages the current arguments about what scientists can say regarding the origins of COVID. The impact of his statements in South Africa was significant. From what I can tell he was completely off base and never made any truly convincing arguments for his position.
- Fauci, of COVID fame, played a big role in getting NIH and the various AIDS community organzations working together and making large improvements to HIV/AIDS treatment. Before that, Fauci was heavily criticized by various LBGTQ orgs (see https://www.nytimes.com/2022/12/31/opinion/anthony-fauci-hiv...) "Larry Kramer, one of the group’s founders, wrote an open letter to Dr. Fauci in The Village Voice calling him a murderer and comparing him to the Holocaust organizer Adolf Eichmann." Again, all this presages the later treatment of Fauci by various political groups during COVID. I often think back to Fauci during HIV/AIDS while reflecting on the current situation around COVID and I think we got lucky to find somebody like him, even if he said a few dumb things, and we'll be lucky if any public servants are willing to take up his role in the future.
- modern gene therapy often uses variants on HIV as the vector. That's right: it's so good at getting into cells and modifying the genome, that we use it as the preferred method. it took quite some time before the vectors were made safe enough (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5152689/)
One of my in-laws is a full on Fox news nut, but has a rare condition that he received treatments for as part of an NIH study that did him a world of good and Fauci was one of the doctors that worked on it, as a result the bits of nuttery he didn't buy into were attempts to discredit Fauci or anti-vax stuff. Oddly it didn't pull into question any other beliefs he picked up from that station.
I believe that's referred to as Gell-Mann Amnesia. Common for most educated consumers of tv and print journalism. Indeed, even Fauci has made mistakes he has later had to correct/retract, like his early herd immunity claim.
> even Fauci has made mistakes he has later had to correct/retract, like his early herd immunity claim.
You get new evidence and you update your beliefs. This is literally how science works and progress is made. If you had to put every student of science on the spot for everything wrong they said/did, there wouldn't be as much progress.
Why downvote, that's exactly what I said. I'm glad you agree that even experts make mistakes. It would be truly strange to argue that point, though many have and do. With respect to Gell-Mann amnesia, to be more exlicit since it seems that's needed, it's really just a side effect of our heuristics. Most of the time you can turn your brain off and follow the crowd, widespread consensus is a safe bet, but you have to leave room for occasionsl mistakes, as you acknowledge. Taking mental shortcuts, being lazy conformists is in no way exceptional. Humans are mostly stupid creatures, even experts.
Um I don't really agree. Making mistakes is not the same as changing opinion based on new evidence.
Fauci changed opinions, a lot of experts do. It's only the lay people with no idea how science works who will call it a "mistake".
Actually it's worse than that, people have openly harassed and threatened Fauci and his family for doing what he did. That's unfair and borderline evil.
He also made mistakes, like telling us masks didn't work to save stock, and then changing guidance when there was enough stock. It's ok, as we're saying here anyone is entitled some mistakes along the way, but nobody is perfect, and overall we got through the worst of it, so it wasn't that bad.
Well if you think he didn't make mistakes, or think that any human is error free, then you have an oppinion that is not based on science. Some sort of zealotry or hero worship or something along those lines. Fauci made mistakes. Science makes mistakes. To err is human. You might want to reevaluaute your beliefs and maybe read some of the copious amount of scientific and philosophic literature on the topic. Everyone makes mistakes.
>> one of the world's most famous virologists, https://en.wikipedia.org/wiki/Peter_Duesberg actively denied that HIV caused AIDS and instead thought it was transmitted by drug use.
I'm curious about his claim that retroviruses (retrovirii?) must be harmless to survive and multiply. What is the mainstream consensus on this?
To be clear: I know next to nothing about viruses (virii? I mean I don't even know how to call them) and I have no idea whether it really supports Peter Duesberg's claims about AIDS in general. I'm just wondering whether he's pointed out an interesting peculiarity of HIV that is not further investigated by others for fear of being accused of denialism.
Scientists can get very like that.
>> (...) the current arguments about what scientists can say regarding the origins of COVID.
It reminded me most about John Ioannidi's polemic against the way COVID was dealt with, rather than its origin. Ioannidis is a leading epidemiologist so he had to be taken seriously, although of course his opinion was rejected by most everyone else.
The mainstream consensus is the he was wildly wrong about HIV specifically, that HIV causes AIDS, and that his influence in South Africa to not deploy anti-viral medications killed hundreds of thousands of people before the policy was reversed.
Part of his hypothesis was that viruses in general, not just retroviruses, were not connected to cancers, the consensus view is that this is completely wrong. We have a very large body of evidence on many virus caused cancers now.
So, the two known human retroviruses both cause disease and retroviruses cause diseases in animals. Duesberg held on to and promoted this concept long after it should have been clear to him that there was zero empirical support for his idea.
To me the most convincing bit that weakens his "hypothesis" is that people who received blood transfusions from HIV-contaminated blood. Many of those people showed none of the risk factors.
Influenced the deaths of hundreds of thousands of people?
Yet apparently to this day he draws over 200k/yr in salary from Berkeley. I believe they are not entirely funded by tuition/endowments which means California tax payers support him at least in part.
He also, that I know of, still supports this position. To this day, you will find people getting into this particular conspiracy and rejecting treatment. It doesn't go well for them.
I do think that freedom of speech is important, and that many attempts to squash "misinformation" are misguided, but some speech has consequences. Personally I find Duesberg utterly reprehensible and morally culpable.
Perhaps I found the article clearer because of familiarity with the subject.
On the "retroviruses must be harmless" virology: He's a denier of viral involvement in cancers in general, not just that HIV must be harmless. He is way outside mainstream consensus on all kinds of things.
For instance, he argues that Kaposi sarcoma, a very common AIDS related cancer was caused by drug use and not opportunistic infection. It is now very well established that all KS, which also affects (typically older) HIV- people, is caused by HHV-8 infection.
The core thing he does on all of these topics is just to ignore or deny anything that doesn't agree with him, eg: Hemophiliacs treated with tainted blood get AIDS, HIV viral load directly corresponds to disease progression which is clearly halted by dropping HIV load with treatment, the HPV vaccine demonstrably prevents cervical cancer, etc. He is far off in quack territory.
I think I understand that retroviruses can cause disease, contrary to what Peter Duesberg seems to be claiming. What I'm wondering about is his claim that they should be harmless in order to survive. Is that something commonly accepted? If so, should it cause surprise that they aren't harmless, and still surviving? Is there an interesting scientific question somewhere in there?
That's the question I couldn't answer by reading the wikipedia article. But I think thanks to some of the comments here my question is at least partly answered: at least some retroviruses -including HIV- seem to not kill off their host immediately, which I guess gives them time to reproduce and infect more hosts.
I don't see any particular reason why retroviruses would be different in that regard: they need the cell they infect to live long enough to produce enough viruses, and it is advantageous to them that some cells they infect lay dormant and reactivate later (a trick not limited to retroviruses), but there's not particular reason why they should not overall act much like any other virus: keeping their host cell alive only long enough to produce enough new viruses to continue to propagate. It's an argument which you could extent to any pathogen: why would any disease kill its host?
> It's an argument which you could extent to any pathogen: why would any disease kill its host?
Moreover, why would a disease even 'care' about the host? As long as it can jump hosts quickly, it can afford to kill many of them. If achieving fast transmission is tough on the host, so be it. Other diseases may select for the opposite approach, of course.
Speculating about the shape of the potential energy surface of viral evolution is non-trivial.
I don't know enough (my retrovirus knowledge is out of date), but if you look at authoritative knowledge (IE, textbooks), you will see many non-harmless retroviruses:
- oncoretroviruses: as a side effect of how they integrate, they often cause cancer in patients. There is lots of time between infection and death for the virus to be transmitted.
- lentiviruses (this is also known as a "slow virus"). There is often lots of time between infection and death for the virus to be transmitted.
It's possible that scientists are avoiding directly attempting to argue with Deusberg's observations, but in general, the consensus seems to be that he brought nothing useful to the debate except irrational claims that were inconsistent with the evidence. We don't live in an ultrarational world where every fringe theory can be investigated.
As for Ioannidis... not sure what to say. I think his big mistake was going to the white house and trying to make Trump an ally and not shut down everything because he predicted the virus wouldn't spread and wouldn't be fatal at the rates that were later observed. Diseases like COVID are multidimensional problems with partial information and a high level of politics, corp, and media involvement. I think fauci and others have finally admitted that they may have made some mistakes in the specific details of the shutdowns, in particular, it took people a while to realize that the impact on children (who by and large are not at risk from COVID) was enormous.
If your goal is to affect public health policy, you have to be a truly 4D thinker, and even that's not enough dimensions.
You reminded me hat Ioannidis made very specific predictions that turned out to be false (about the number of deaths we could expect). And that, while measures were adopted that he claimed were useless. I agree Fauci saved lives - and last time I saw him in the news he was being attacked by Republican trolls, I don't have any other word for those people.
> we'll be lucky if any public servants are willing to take up his role in the future
Sadly, there will be plenty of people desperately wanting that job. It is definitely a prime example of the saying those that want the job would not be good at the job and those that would be good at the job do not want it. Especially in today's environments where it will become a bully pulpit to push whatever agenda of whoever is in charge
> I often think back to Fauci during HIV/AIDS while reflecting on the current situation around COVID and I think we got lucky to find somebody like him, even if he said a few dumb things, and we'll be lucky if any public servants are willing to take up his role in the future.
Hopefully, the next administration doesn't come up with Schedule F once again and make all health-related government jobs political.
Don't forget Kary Mullis as another famous scientist thinking HIV does not cause AIDS. I personally don't know what to make of Mullis' and Duesberg's claims. But I found an interesting Mullis article recently in which he presents a hypothesis about how AIDS could develop independently of HIV. Quite interesting, but I am guessing nothing really more than that. https://link.springer.com/article/10.1007/BF01435010 The article is unfortunately paywalled.
Just to be clear, this is not a vaccine. It is an antiviral drug delivered by a long-lasting subdermal delivery implant. It has been known that antiviral drugs effectively prevent HIV infection for some time now (about 20 years). Recent work has been on better-tolerated and longer-lasting formulations.
Treatment of HIV+ people also reduces their infectiousness, and good treatment reduces the risk of passing the infection on nearly to zero. Providing sufficient HIV antivirals and medical care to everyone in the population, both HIV+ and at risk for HIV, in theory, could be enough to halt the pandemic. Some wealthy countries with sensible policies have seen remarkable gains. The UK is reasonably effective at getting drugs to both the HIV+ and to at-risk populations, and the number of new HIV infections there, has been reduced by approximately half in the last decade.
> It is an antiviral drug delivered by a long-lasting subdermal delivery implant.
I don't see anything to indicate it's an implant - the prescribing information [1] says it's a subQ injection, and the trial information [2] seems consistent with that.
You're right. I blithely assumed any drug with such a long half-life must have some sort of delayed dose mechanism. But it seems it's just extraordinarily stable and is very, very slowly absorbed. Remarkable.
It’s not a vaccine, but it’s close to one at twice a year.
Even if we can consider HIV “cured” in the developed world (where PrEP is available to anyone who wants it) there’s no way we eradicate HIV from impoverished countries with limited healthcare access until we either have 1) a vaccine, or 2) a shot (or something) that prevents HIV for a really freaking long time.
Not sure if 6 months will quite cut it, but it’s great to see progress in the right direction. More advancement is needed.
I assume you’re referring to things like the flu vaccine. Many vaccines can last 10, 20 years or more which this doesn’t come close to.
That’s not to say it’s not a great improvement, I happily await the day we can nearly eliminate some of these infectious diseases that plague humanity.
> we will eradicate HIV within the a single generation at this rate
If there is one place socialised medicine makes so much sense that almost any argument against it is invalid, it's around contagious diseases. The prevention and treatment, inasmuch as it reduces transmission, which is true of virtually all HIV treatments, should be as effortless as possible. That starts with making it free.
We had a taste when COVID shots were free, and it was magical. So nice not having to make 16 phone calls and then getting billed $800 "by mistake", followed by 20 more phone calls to fix it, only to find out that the pharmacist's sister's mailman was out of network, so we're sending your bill to collections because it got lost in the mail.
Wouldn't complete eradication mean eradication in all countries? Given HIV policies degradation in Russia, which is significantly affected and has a sizeable population, your assumptions sounds too optimistic, even though I agree that would be a great achievement.
Programs like George Bush's PEPFAR have made great strides in fighting HIV globally through treatment and prevention. Estimated at 25 millions lives saved in 20 years, mostly in Africa.
Unfortunately it's become a target of the right wing culture warriors and certain groups are trying to gut it, after huge strides have been made in reducing global transmission of HIV.
Yeah but the united states is also the main cause of developing countries not having access to cheap medicines through the enforcement of IP laws. You can look up the special case of India and Brazil who managed to negotiate in a much better way and so are entitled to cheaper treatments.
I know someone from a EU country that had to do medical tourism to Brazil to afford hepatitis and HIV treatment as the drugs are so expensive that the doctors at public hospitals (in that country at least) will not prescribed them and instead manage the illness in other ways for the first few years. This is bad because the disease progresses faster.
> we will eradicate HIV within the a single generation at this rate!
In the same way we eradicated COVID? /s
First of all, COVID is still around just less common.
Second, this HIV implant is a twice yearly implant. Not a one-time preventative cure.
Third, User Rlad in these comments calls into question its efficacy suggesting it merely stops replication but not infection. Once a cell is infected with HIV, a cell is permanently infected. This posit’s the concern that once a person stops receiving the implants, the dormant virus will then begin replicating —- fully infecting the individual. That makes this drug sound a lot like Luciferium from the video game Rimworld.
Fourth, the inactive ingredients need to be studied. If they contain heavy metals such as mercuries and aluminums, that a reason for pause and study. Autopsies of brains affected by Alzheimer’s usually find high levels of heavy metals in the brain. Heavy metal poisoning causes all sorts of cognitive issues.
Fifth and last, too large of an immune response is associated with the creation of new allergies. All allergies are a product of an immune response to something that the body shouldn’t have an immune response to. While HIV protection trumps new allergies, it’s worth examining side effects especially if some are mostly permanent. I also don’t know if this drug causes any kind of immune response. It’s all a starting point for someone who wants to study it more to study so you can come to your own conclusions after studying.
The drug, Lenacapavir, is a capsid inhibitor. That means it prevents HIV virus from assembling into infectious particles by interfering with the production of the capsid and packaging of viral RNA into it.
This also means that it actually does not stop infection. Cells still get infected, but this drug prevents more virus from being produced.
My question is, since there are infected cells in these individuals, if they stop taking the drug aren’t they likely to become immediately highly infected, because the drug only interferes with viral replication while it is present in the body? Once infected, a cell is permanently infected.
I think this should be the case, unless infected cells are somehow killed off through some other mechanism: maybe they get lysed through an accumulation of partially formed capsids?
Beautiful news to see. I've often heard that cracking an HIV preventative cure would be the end-all-be-all to creating preventative cures for most viruses within the decade of its discovery; I wonder if this optimism is still there.
Amazing. I guess SARS-CoV-2 is much less stable in comparison to HIV?
Higher mutation rate and other shifts vs broadly neutralizing antibodies? Anyways, it would be nice to fully "solve" COVID-19 as it's still wreaking havoc somewhat silently (?)
I also wonder when or if we'll see therapeutic vaccines against either of these and more sooner than later?
Each time I only briefly start staring into the abyss that is "wetware" I'm gladly returning to our comparatively trivial (self-inflicted) complexity in the world of software / computing.
HIV is notoriously unstable - RNA viruses don't contain any error checking during replication. Which is one reason HIV drugs, including those one, are almost always used in combination.
There are several variant-resistant pan-Covid/pan-Sarbecovirus/etc. vaccines under development [1], including one by the US Army [2].
Vaccines are notoriously slow to develop, perfect, and test for safety and efficacy. The original Covid mRNA vaccines were developed at breakneck speeds as far as vaccines go. Unfortunately, much of the funding has since dried up.
In fact, it's HIV that's much harder to develop a vaccine for. HIV vaccine research has been going on for 40 years and hasn't really had any candidates that went beyond "plausible" until recently.
This is anti-vax misinformation. I don't think actual evidence, studies or data would support this. Let's take a look at real information and refresh our memories.
Uh, no. It's actually extremely effective against the target variant. The original Wuhan strain is extinct as a result. In areas with high vaccine uptake, the population has very high levels of neutralizing antibodies against it, to this day. Even if it somehow broke out again, it would die off within weeks, as most of the population is immune to it.
Evolution has driven the virus away from the neutralizing antibodies. This is called immune escape. Recent variants have very little antigenic overlap with the original strain. The original antibodies are not very effective, so people can actually get sick once again.
The FDA now updates the vaccine formulation every year. This means that every year, there is a time window during which the vaccine formulation and the circulating variant are the same. If you get an updated shot as soon as it becomes available, you're immune for all practical purposes until a new variant emerges.
Right, but most diseases we have vaccines for can’t easily evolve their way out of them like in this case. That’s kind of the point.
And you’re far from immune with the newest formulations. From the CDC: “People who received the updated COVID-19 vaccine were 54% less likely to get COVID-19 during the four-month period from mid-September 2023 to January 2024.”
The updated 2023 vaccine was based on XBB.1.5. In the period you quoted, the variants based on the massive BA.2.86 saltation took over, including JN.1 which was fully dominant by January. XBB.1.5 and BA.2.86 are antigenically very different. I would not be surprised if the case ratio between the two branches during the period was in fact 55:45, i.e. matching the CDC's 54%.
Regrettably, this is one's on the FDA, as XBB.1.5 was already on the way out when the FDA chose it. Part of the problem was their desire to include Novavax in the lineup. It has a much longer update turnaround time than Moderna and Pfizer, and Novavax had already committed to XBB.1.5 by the time the 2023 VRBPAC meeting took place.
As for the original vaccine, the waning measurements were in terms of antibody titers, not in terms of actual effectiveness against the target variant. Delta emerged in the spring of 2021, and it had significant immune escape from WT (Wuhan.) By the time the population was immunized against WT, Delta had already driven WT out.
There have not been many reported cases of non-immunocompromised people getting infected with the exact same variant they had been vaccinated against or previously infected with, particularly with WT. There has been too much evolution in the timeline to even dig out the signal.
The original WT mRNA effectiveness measurements were 92-95% IIRC. For all we know, the missing 5-8% might be attributable to immune deficits, early infections, and/or incomplete B-cell maturation. I haven't noticed any research that measured the likelihood of single-variant breakthrough infection, but if you find some I'd like to look at it.
As for other diseases, they are not in the pandemic phase, so their vaccines can be optimized accordingly.
I would dispute that "easily evolve" notion, though. There have been billions of Covid cases since 2019, including countless immunocompromised patients who are basically walking virus incubators. Yet there have only been a handful of major saltations. It's actually quite likely that Covid will eventually be defeated completely.
This injection isn't a vaccine, it's an anti-viral drug being used as pre-exposure prophylaxis. The first approval of this approach was in 2012, but using an oral pill with a short half-life taken daily.
That drug is still in use and also highly effective, the new improvement is to provide the same approach with a longer acting injected drug. One reason there has been great interest in this, despite the already effective oral PREP, is that there are thought to be socio-behavior advantages for cases like women in Africa as in this study. For example: the woman does not have to keep a supply of daily pills that a partner can find. Also possibly improved adherence with no missed doses.
The drug itself is not thought to be more biologically effective than the oral drugs, which are basically already at close to 100% effective assuming the patient actually takes them as scheduled.
I'm not sure if taking e.g. Paxlovid as pre-exposure prophylaxis has been studied, but my guess is that the side effects from the drug are worse in the long run than the disease itself (especially if the seriousness can be blunted via vaccination).
Since people don't spontaneously recover from HIV infection, and the PrEP drugs have relatively few side-effects, the tradeoff is more favorable.
No clue if this easy trick would induce immune escape if a large number of people started using it. I guess it's a good time to get in on the ground floor.
1. "Prophylactic or therapeutic administration of neomycin provided significant protection against upper respiratory infection and lethal disease in a mouse model of COVID-19."
2. "Furthermore, neomycin treatment protected Mx1 congenic mice from upper and lower respiratory infections with a highly virulent strain of influenza A virus. "
3. "In Syrian hamsters, neomycin treatment potently mitigated contact transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)."
4. "In healthy humans, intranasal application of neomycin-containing Neosporin ointment was well tolerated and effective at inducing ISG expression in the nose in a subset of participants."
The mechanism appears to be that Neosporin triggers an ISG[1] (immune) response? Not a biologist etc, but the results showing that it prevents transmission is only in rodent models, and then showing that a similar biomarker shows up in (some of) the participants and the rodent models. They authors say:
> "These findings suggest that neomycin has the potential to be harnessed as a host-directed antiviral strategy for the prevention and treatment of respiratory viral infections."
Obviously it’s not stimulating the immune system but it works as an antiviral barrier. I’ve been using it since I read that study and I’ve avoid 2 of my daughter’s colds since (and still got 3). That might not sound impressive but I have a terrible immune system and haven’t avoided a cold from someone I’ve had close exposure to in as long as I can remember.
That said, I might need to add some Neosporin to my mixture when she comes home with her nose running.
I make my own. There's at least one product out there but it's something like $20 a bottle and you can make it for pennies. Here's a recipe:
For 150ml of (distilled) water:
1.35g of salt
1.8g of iota carrageenan
A drop of polysorbate 20
Heat up the water to close to boiling, add those things, shake it up, and there you go.
Note: That was supposed to be in line with the product that was tested, but I've found adding more water makes it come out of the nose spray bottle thing better. It's still pretty thick, just not a complete gel. Perhaps there's another type of spray bottle that would be better.
This paper gets ripped into in my favorite podcast, TWiV (This Week in Virology)!
Essentially, yes, neomycin in the nose, if timed perfectly, can activate the innate immune system, but en mass this practice would cause the spread of antibiotic resistance.
If it turned out to work great in practice and people started using it en masse, the benefits would greatly outweigh the costs IMO, particularly if it snuffed out Covid and/or the flu. If it ends up being a niche thing, I doubt it would bite into the resistance numbers.
Besides, we're already spiraling down the resistance chasm with antibacterial soaps, stuffing cattle with antibiotics, overprescribing, and so on.
I tested positive for COVID last weekend, was out of action for three days and spiked a 40.3C/104.5f fever. It was worse than when I got it three years ago.
"
PURPOSE 1, a Phase 3, double-blind, randomized study, is evaluating the safety and efficacy of twice-yearly, subcutaneous lenacapavir for pre-exposure prophylaxis (PrEP) and once-daily oral Descovy® (emtricitabine 200mg and tenofovir alafenamide 25mg; F/TAF) in more than 5,300 cisgender women and adolescent girls aged 16-25 across 25 sites in South Africa and three sites in Uganda. The drugs are being tested in parallel, with one group receiving twice-yearly lenacapavir and one group taking once-daily oral Descovy. Additionally, a third group was assigned once-daily oral Truvada. Study participants were randomized in a 2:2:1 ratio to lenacapavir, Descovy and Truvada, respectively. Because effective PrEP options already exist, there is broad consensus in the PrEP field that a placebo group would be unethical; thus, the trial used bHIV as the primary comparator and Truvada as a secondary comparator.
There were 0 incident cases of HIV infection among 2,134 women in the lenacapavir group (incidence 0.00 per 100 person-years). There were 16 incident cases among 1,068 women in the Truvada group (incidence 1.69 per 100 person-years). The results demonstrated superiority of twice-yearly lenacapavir over bHIV (primary endpoint, incidence 2.41 per 100 person-years) and superiority of twice-yearly lenacapavir over once-daily Truvada (secondary endpoint), with p<0.0001 for both endpoints. In the trial, lenacapavir was generally well-tolerated and no significant or new safety concerns were identified.
[...]
Gilead expects results in late 2024/early 2025 from the program’s other pivotal trial, PURPOSE 2, which is assessing twice-yearly lenacapavir for PrEP among cisgender men who have sex with men, transgender men, transgender women and gender non-binary individuals who have sex with partners assigned male at birth in Argentina, Brazil, Mexico, Peru, South Africa, Thailand and the United States.
"
This is a legitimately amazing result and a huge win against HIV. I hope it replicates in PURPOSE 2. Zero incident cases in an at-risk population is, frankly, fantastic, in a country where prevalence of HIV ranges from 12-27% depending on the province.
I read that as cisgendered && (women || adolescent girls) && (16 <= age <= 25). Basically 'cisgendered' and the age range are describing all study participants which which are all either women or adolescent girls which makes sense to me based on how I believe these trials are generally constructed.
Very often "women" and "men" in medicine refers to adults, i.e., 18+.
Likewise, we use the term "girl's/boy's" tennis in high school but "women's/men's tennis" in college because most people in high school are under 18 even though they are "women" and "men" in many relevant senses.
The term matters to the study, because they were interested in a comparable group of women. I don't expect HRT is realistically available in that area, so they're just reporting that they didn't need to deal with that complication.
This prevalence is true in the US (and most Western countries I think, though not as certain), is definitely not true in Sub-Saharan Africa (where 75% of the world's HIV+ population lives). Women and girls are more likely to have it in Sub-Saharan Africa. See https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10126805/ estimates that over 60% of all new infections in SSA are in women. Parts of that region the HIV+ prevalence rate is above 5%. That is why they are focused on testing that population in that region, they are the most at risk.
For the existing HIV-preventing medications we have, such as PrEP, the treatments are much more effective in men than women. It can easily take a month for PrEP to be effective in Assigned Female At Birth folks, but I saw studies during the COVID era that a few days were plenty for Assigned Male At Birth folks. There's some logic to focusing on the cohort that usually has the lowest success rate with these kinds of medication.
The difference in efficacy has to do with the way the body is designed to absorb fluids, and its one of the few areas where hormones and surgery don't make a difference. (A trans guy on HRT with a full set of surgeries generally has male chances of cardiovascular issues, male levels of calorie consumption/muscle-building, etc.)
I see, so you're saying that "cisgender female" means Female As Identified at Birth, but includes both trans and not trans groups regardless? Thus, "cisgender female" includes both homosexuals and non-homosexuals (and non-binary etc), but actually some from this group may presently identify as male? I did not know this.
A bit simpler: cisgender means same/matching gender, basically the opposite of trans-gender. If the gender you identify as is the one matching your birth sex default, you're cisgender.
But it's completely separate from your attraction to other people, so straight, gay, anything is fine in either category.
The paradox of living in this day and age is witnessing astonishing advances in science, while enduring the increasing levels of anti-intellectualism that pervades society like a cancer.
Ok, but please don't post generic tangents to HN. They make the threads less interesting, more tedious, and (possibly as a result) tend to turn them nasty.
I think all the really obvious and influential products of science and technology happened in the 20th century and now we're so comfortable because of those that we take it for granted. Then people find reasons to hate it because they forget how bad things were without it (previous generations). Same goes for political stability.
Another aspect is that a lot of intellectualism is really activism with "intellectuals" trying to impede other people's lives for the sake of some arrogant moral purpose.
> now we're so comfortable because of those that we take it for granted. Then people find reasons to hate it because they forget how bad things were without it (previous generations). Same goes for political stability.
I'm not sure that most people are really all that comfortable. They're a lot more distracted though certainly.
I think there are a lot of different reasons people today have a problem with science and technology. Some are scared of it. Some just don't trust it, which can be entirely fair depending on the degree/situation. Some see that the regulations, oversight, and accountability we expect and depend on to keep us safe aren't working like they used to or like we thought they would.
Mostly I think people see not only what we've gained, but also what we've lost and could/should have again. Reliable and repairable products that weren't designed to exploit and work against the interests of the person who paid for them for just one example. We've had many trade offs, where they've improved things in some areas while making them worse in others. It hasn't always worked out in our favor. It's also frustrating when you see that amazing things are now possible, but we can't have them because of politics, or greed, or fear of change.
Personally, I hope people never stop wanting and expecting better from science and technology. Especially in those cases where what previous generations had was better than what we're expected to accept today or where we've created problems previous generations never had to put up with.
> I think there are a lot of different reasons people today have a problem with science and technology. Some are scared of it. Some just don't trust it, which can be entirely fair depending on the degree/situation. Some see that the regulations, oversight, and accountability we expect and depend on to keep us safe aren't working like they used to or like we thought they would.
We often forget that many people have been genuinely negatively affected by technology or science or know someone who has. Let's not forget that many technological and medical advances have come at a real human cost. People have been poisoned by harmful chemicals either during their occupation or because an entire community has been exposed. Entire communities have been devastated by the opioid epidemic which the medical community is directly responsible for. Not to mention the countless people who have lost their jobs or will lose them soon to automation.
There are people with genuine concerns about the way science and technology are heading and pretending anyone skeptical of modern science is simply uneducated or stupid is extremely counter-productive.
I think things like the opioid crisis where doctors were getting outright bribes from pharmaceutical companies who knew they were killing people has done a massive amount of harm to the trust people had in medical science. It's been a problem for a long time, even going back to the tobacco industry hiring researchers to lie about the dangers of smoking. Those researchers didn't lose their jobs and become unhireable in their fields. They just went on to work for the oil companies to lie about how climate change isn't real and are now working for companies currently trying to convince the FDA about the safety of food additives.
Between corporations being able to buy whatever research they think will get them a favorable headline, peer reviewed journals accepting any paper if you pay them to publish it (this one being a personal favorite https://www.sciencealert.com/a-neuroscientist-just-tricked-4...), the reproducibility crisis more generally, the total lack of any meaningful consequences when companies are caught outright knowingly poisoning people or selling dangerous drugs, it's really getting harder to explain to people at the fringes like antivaxxers why they should have more faith in the data we have and on the systems put in place to protect them.
If the people aren't held accountable for causing harm and scientists don't do a much better job self-policing I think the situation is only going to get much worse. Even if things do change it will likely take generations to undo the damage already done.
> I'm not sure that most people are really all that comfortable. They're a lot more distracted though certainly.
I think people in wealthy countries like the USA are very physically comfortable, but also quite unhappy- possibly much more unhappy day to day than they were historically when there was a lot more disease and discomfort- and a lot of that is directly a result of excess comfort combined with a life without any real difficulty, challenge, or sense of meaningful purpose. We feel like we want comfort, but it's mostly harmful to us. Humans just aren't built to be "house pets." People need a sense of purpose, of overcoming difficult challenge, and an ability to directly see positive results from their efforts. The challenges need to be both mental, and physical.
What we have now is lots of empty entertainment, stupor inducing comfort, and lots of sedentary careers that feel pointless, where nobody even notices the difference if you work hard or not. More and more people are burned out at work, and socially isolated.
I don't think the answer is to go "backwards" and lose all of our progress in treating disease, making labor easier, etc. but in a cultural and personal change where we find some new meaning and challenges, to grow even more. Personally, I've found this through being a scientist where I can work on hard problems, as well as doing physically demanding and uncomfortable hobbies like weight training, fasting, and cold water swimming.
I've noticed that the more intentional physical discomfort I experience, e.g. from cold, the more content I feel, and the less I crave comfort, or other addictive things like social media and overeating.
People don't _feel_ comfortable but they objectively are much more comfortable that 120 years ago or more. Unfortunately being objectively more comfortable doesn't make you feel more comfortable and ultimately it matters how you feel and want to fix whatever is causing them to feel like shit.
We're physically more comfortable and that's mainly what technologies promised and delivered. Maybe a new wave of technology improving how we feel emotionally will come with just as much enthusiasm as the old physical technology, but so far it seems we're only going backwards. Maybe that emotional technology was invented thousands of years ago in religion and social norms but we never bothered to adapt it to our modern environment so we lost it.
> Another aspect is that a lot of intellectualism is really activism with "intellectuals" trying to impede other people's lives for the sake of some arrogant moral purpose.
In Germany, unlike every other European country (maybe except the Polish, not sure if they're doing the same with Auschwitz?), we have every generation of school children visit a Nazi Konzentrationslager once - precisely to avoid forgetting how bad it was, by showing the actual, undeniable evidence. And on top of that the Nazi dictatorship is usually an entire year's worth of history lessons in schools.
Despite the far-right being on the rise as well as everywhere in Europe, they still have a harder time here, which I think is mostly due to these two education policies.
I do not think it's working. The AfD was the second most voted party for the European parliament, despite their candidate literally defending the SS a few weeks prior.
European elections are usually used to deliver a "Denkzettel" to the currently governing party, it's the same across Europe as these elections are (wrongly) seen as consequenceless.
Federally, the AfD is around 15-18% [1], which is still way too high in my opinion, but they're far from any chance to gain relevant influence on politics. Statewide is a different beast, sadly in Eastern Germany (the equivalent of the "flyover states" in the US) they're almost at the 33% required to block major legislation [2]. I'm honestly not sure how to combat that any more, outside of a (well deserved, given e.g Höcke directly using banned NS slogans) ban on the party.
I'm honestly not sure how to combat that any more, outside of a ban on the party.
Perhaps by getting rid of these haughty, and one simply has to say: typisch-Wessi notions of the new Länder as being "flyover territory". Which is part of what drives people to vote for AfD in the first place. As if the former West Germany doesn't have its own stereotypically maligned areas as well.
Excuse me, are you saying that teaching kids about past horrors including onsite visits to places where those horrors took place, with pictures and film and everything is "brainwashing"?
He’s making the point that poor governance delivering poor outcomes will eventually by replaced by its ideological opposition, no matter how distasteful.
No, he isn't saying that. The context was "children are taught why Nazis are bad but now people are voting for Nazis" and his response was to say people were brainwashed to defend going against their interests.
He may not be saying this to imply that the Nazis would have been acting in the interests of the voters but that's what the notion that teaching children Nazis are bad is brainwashing (to allow the government parties to go against the interests of their voters) strongly suggests. Couple this with a comment history of being vocal against "economic refugees" and a German political context of the AfD heavily using migrant scares in their rhetoric and it's entirely legitimate to challenge this statement.
It's also worth mentioning that AfD politicians have not only defended the SS but also loudly complained about Holocaust remembrance and downplayed the extent and significance of the Holocaust.
Your reply completely ignores that he deliberately used the word "brainwashing" which the comment you replied to called out. Intentionally or not, your reply demonstrates a motte-and-bailey (the bailey being that teaching about the Third Reich is brainwashing, the motte being the content of your reply).
Technically, I think teaching in general is basically brainwashing/propaganda. The primary difference is that what we're teaching us socially/culturally acceptable, if not actively _wanted_. Much like the thing about paranoia only being related to what you're thinking/feeling, regardless if you're correct.
I wonder, how it is usually spinned? I'm asking as Russian and I see direct evidence of how people who grew up in the constant narrative "fascism is awful, that war was important, our grandparents are heroes" also, it seems, consumed it in easy/stupid form of "fascism is something that those weird germans do, they attacked us, and we won, so we can't be fascists ever".
I'm pretty sure there are places in Europe where the AfD equivalent doesn't get 15%.
Trip to a holocaust museum is nice and all, but it probably fails at making people understand the problem. They'll kind of nod that yeah, Nazis were bad but then happily go and blame others for their bad decisions and vote for populists with easy solutions.
Somehow half of Germany thinks Russia is OK, because they "saved Europe", hammer and sickle symbols are still not treated the same as swastikas and, of course, the main outcome of the kind of education you mention is that Germany is basically freeloading wrt defense and very unwilling to do the only reasonable thing, i.e. help prevent another genocide as it unfolds in Europe.
Hopefully something has changed in the last 2 years, but the preceding decade, spending over 100 million euros daily on Russian natural gas is hard to undo. And that's with pre-war historical minimum prices. Since you all didn't get the memo that you need to stop buying Russian stuff until NS2 got blown up, the flow of money for natural gas from Germany to Russia in 2022 and 2023 is likely several times the pre-war annual number.
And then you have people saying shit like "we have spent enough on Ukraine" or "Ukrainian refugees are coming because of our social safety net", not even from AfD politicians (I think some CDU idiot, lol). Yeah sure, but you gave 100x the money to Russia, who of course spent it on weapons because they don't give two fucks about their own people.
Being sorry about things from the last century, while failing completely to judge the situation in the present doesn't really help. Not to mention Poland still didn't get the war reparations for WW2 last I checked. They probably don't want to shake the boat too much and just hope Germany will at least stop being useless.
Do you really think there is no intellectual work to be done on moral subjects? That morality is entirely in the realm of folk intuition? If you thought very hard about some moral question and came to another conclusion than most of society, what would you do about it?
Would you have called intellectual abolitionists people trying to impede other people's lives for some arrogant moral purpose?
Like, I get it, nobody likes a woke-scold, but it is still weird to complain about the idea that an intellectual who comes to a moral understanding might want to act on that new understanding/change the world/convince others.
I don't really know the state of moral understanding, but I do know people, even intellectuals, can't separate their personal ideologies from their work, so they're not really capable of objectively figuring this stuff out.
I'm sure we can at least make some judgements about whether a set of morals is better or worse than another, but all the obvious cases are already solved and people strongly disagree on the ambiguous ones where they really have no idea.
One big moral concept is individual freedom vs long term survival of the system of social order they belong to. You can't have individual freedom without a society to protect it but you can't sustain that society without restricting people's freedoms (eg. military conscription). It's popular today in the west to value the individual over the future of their society, but a lot of history and the rest of the world is the opposite. People from these two camps seem to be blind to the weaknesses of these underlying assumptions, so they end up with moral ideas that seem totally immoral to each other.
I don't understand how anyone could separate their personal ideology from their work unless they happened to mostly align already. I might disagree with a person's ideology, but I can only agree with a person who believes their ideology ought to inform everything about their life, including their work. What other use is an ideology if it doesn't compel you to change the world or, at the very least, yourself, despite resistance from the world?
In the US you also have situations where all that science means that effective treatments exist but they are entirely out of your reach because of insane healthcare costs.
I can't imagine having to watch a loved one slowly die knowing that you are surrounded by doctors who could save them if you only had the tens to hundreds of thousands of dollars they demand or if you'd been living in basically any other developed nation on Earth.
I’m certain that the US is in no way unique in that. Countries with universal public healthcare care systems do cost-benefit analysis all the time and access to the newest effective treatment options outside of the richest/most developed countries (or even in them) is far from guaranteed. e.g good luck buying latest cancer drugs from the US on an East European salary after your local healthcare system bureaucrats have rejected them because they are too expensive and/or are taking a year or two to decide of they are worth buying.
> or if you'd been living in basically any other developed nation on Earth.
That’s just beyond absurd, unless you think that only Switzerland and a handful of other rich countries are “developed”. Yes getting some minimum/acceptable level of care when you’re not rich might generally be easier. Getting access to latest or even experimental drugs (most of which are developed in the US)? Not so much..
This is partially true but for many things the price is different. In the US drugs are priced assuming that there are some number of rich people who can afford them. This often results in higher margin pricing which is more profitable even if the volume is lower and puts them out of reach of many. In countries with public health care, setting the price that high will typically result in near-zero sales, so the price gets set closet to the cost-benefit point to make profit in lower margins but higher volumes.
It doesn't always work like this. Some drugs are just too expensive to manufacture and the minimum profitable price is too high for the benefit in public health care. But often the bargaining and purchasing power of a public health care system can achieve lower prices for drugs and other tools.
That's because we subsidize the world by investing in a massive portion of the science and tech for producing medicines. Then when those costs are recouped via sales to our consumers the whole world laughs at us while ironically many of them would be up shits creek without the advancements they get to piggy back off of.
Healthcare and medicine needs overhauling but it's maddening watching these downstream foreign benefactors damn the golden goose they'd be fucked without.
I don't think it's necessarily true that we need to keep letting Americans needlessly die due to unaffordable healthcare in order to maintain our nation's lead in innovation. We should be able to continue to invest in medical science without continuing to fall behind other developed nations in actual health outcomes for patients. There are certainly many opportunities to drastically reduce the costs of healthcare without impacting the budgets for research.
Does the US actually fall behind other nations in health outcomes? The US has two big factors working against them: much more widespread obesity (and the level of morbid obesity) and the insurance bureaucracy. These two factors should negatively impact health statistics without the treatments being worse.
> Does the US actually fall behind other nations in health outcomes?
For the world's richest people you couldn't do better than to be a patient in America. For most Americans though, the US healthcare system is failing them. America does worse compared to other nations in some very basic measures like having a lower average life expectancy, a higher infant morality rate, more obesity and congestive heart failure and more hospital/pharmacy screw ups. A child or teenager in the US is less likely to live to adulthood compared to those in other developed countries. It's not any better when it comes to mental health either. The US is one of the worst nations when it comes to mental health outcomes and suicide and drug related deaths are higher in the US. Over thirty percent of the US population has been forced to put off getting the care they need due to the cost and preventative care is usually the first thing that people cut back on leading to bigger problems that could have been avoided entirely.
If you adjust by factors like obesity, state and drug use US is quite close or more or less on the same level as Western European countries.
Even if you don’t do that there is a higher variance in life expectancy between different US states than inside the EU. e.g. California is about on par with the Netherlands, Germany, Britain while Mississippi and West Virginia are slightly below Bulgaria (of course mainly because of drugs..). IMHO that kinds of makes generalized comparisons semi-meaningless.
"Yeah, but just unimportant people from flyover states. We have to divide our analysis of the United States: Over here in California - you now were the people we care about live - life is just as good as in these other fancy European countries we don't look down upon."
People who can't do basic math and skip prevention are responsible for their own shit outcome.
People in Portugal, where healthcare is "free", i.e. the government pays for it, frequently wait for years before being able to see a specialist due to long waitlists. The obvious outcome is that only poor people use the system and if you can you use private healthcare.
People in Czechia with single payer healthcare system with e.g. average wage of 2000 USD pay from 100 euros a month for health insurance (unemployed) to e.g. 500 euros (with 4000 USD salary) or more if you make more. You get the same shitty service (something like 20 years behid the US), you just pay a lot more if you make anything resembling a US salary.
There's no such thing as free healthcare. Can you make a single payer healthcare system that works better? Sure, it's just hard and even if everything is ideal you get maybe 50% discount. The main way to make healthcare cheaper is to drop coverage for diseases that are expensive to treat.
- 90% of Americans have health insurance - I would say it works for more than half (most) of Americans. Granted, not all health insurance is created equally.
- The obesity and congestive heart failure issues is a function of poor dietary choices most Americans make (choosing fast/process food over cooking/making healthy foods), and not a function of healthcare access
Clearly having health insurance isn't enough to make healthcare affordable or prevent patient outcomes from being worse for Americans than patients in other nations.
> The obesity and congestive heart failure issues is a function of poor dietary choices
I also suspect that obesity and congestive heart failure issues are heavily influenced by diet, although I think that "choices" might be misleading here and that being unable to afford basic and preventative healthcare likely does have a major impact in healthcare outcomes even when the problems come from obesity and heart failure.
It's certainly not as if people in other nations don't also enjoy ultra-processed foods or are any less fond of sugar, fat, and salt. They just often have better access to healthier foods, and more stringent regulations concerning what companies are and aren't allowed to put in foods, what they are allowed to advertise, and how they are sold.
There is a huge difference between the number of people in the US who have little to no access to healthy foods when compared to those in other developed nations. Sometimes it's physical access (food deserts) and sometimes it's a matter of costs, but I don't think there's anything inherent to Americans that forces them to make bad choices. I'm guessing that instead Americans tend to have less choice and fewer opportunities for healthy foods in the first place, while having unhealthy ultra-processed foods that would be banned in other countries readily available, easily affordable, and heavily advertised to them.
I call bs on the second part. It's not unhealthy food that makes you gain weight, it's how much food you have.
On top of that, the healthiest foods are among the cheapest foods you can buy. Milk, oatmeal, potatoes, rice, macaroni, chicken are all cheap compared to most foods you can get. This stuff is available almost everywhere.
>but I don't think there's anything inherent to Americans that forces them to make bad choices.
It's partly cultural. But this isn't a uniquely American problem. It's just worse in the US. 72% of Americans are obese or overweight.
On top of that there was a recent study that found that BMR has decreased in the last ~30 years. Among men it was even up to 7%. That's a big enough difference to take someone from barely overweight to obese over a lifetime. But this is only a single study so far.
> On top of that, the healthiest foods are among the cheapest foods you can buy.
The usual argument here calls out "bulk beans and rice" instead of potatoes and chicken, but in both cases you aren't going to find that in a gas station or convince store which for many Americans (some 40+ million) is the only place they can get groceries. If they're getting chicken it's not going to be whole and uncooked. It'll be sold in a plastic bag leaching PFAS into the food and be coated in high fructose corn syrup (most packaged lunch meats have sugar or HFCS added). Those kinds of places tend to have very little fresh fruit and veg as well.
If you're looking at cost per calorie unhealthy food will often win out as less costly, not just in terms of money but also time and effort. Someone who works two jobs and spends hours sitting on or walking to/from the bus isn't always going to have the energy or time to roast a chicken. It's easy to see why they'd choose what's fastest, highly satisfying, requires less preparation and clean up, and is inexpensive.
Not that I'm suggesting that the 72% of Americans who are obese/overweight have those kinds of problems... just that you'll find more Americans who are in that position than you'll find somewhere like the UK.
I found the study on the decrease in BMR. That's pretty wild and if true, I wouldn't be surprised if it was a factor in the obesity problem.
>If you're looking at cost per calorie unhealthy food will often win out as less costly
What you should be looking for is cost per gram of protein. That's the only macro nutrient you need large amounts of. Calories per gram of protein are important too - oatmeal and dried pasta are the cheapest protein/$, but their protein/kcal is too low.
I think it comes down to 'not caring enough' to try to get it under control. All the obfuscation and noise around nutrition ("healthy food") doesn't help either, but it's doable.
>I found the study on the decrease in BMR. That's pretty wild and if true, I wouldn't be surprised if it was a factor in the obesity problem.
It might even be the main part, at least for men. If your normal TDEE is 2136 kcal and you eat at maintenance, but then your BMR drops by 7.7% (165 kcal) then you'll gain weight until your TDEE is at 2136 kcal again. During this you would go from ~80 kg to ~95 kg taking you from 24.7 BMI to 29.3.
An argument against the study is that it could be due to different measuring techniques. On the other hand, we have found that the average temperature of humans is slowly decreasing, so maybe it's true.
It's not all roses. I'm sure that even the wealthy who get healthcare in the US do have to deal with things like over-treatment, a lack of regulations, excessive costs, etc. It doesn't seem to hurt their outcomes enough to offset the fact that they'll have far more options, greater access to the best avilable technology/treatments, and that they'll be treated like absolute royalty.
No. If you get something like cancer, at best you can expect Medicaid to be comparable to basic private health insurance, which can easily leave people with out of pocket costs they can't possibly afford.
Medicaid has a ton of other problems starting with eligibility, but even if you are eligible and you successfully jump through all the hoops to keep it (which are sometimes totally insane: https://youtube.com/watch?v=bVIsnOfNfCo), you still may not be able to get the services you need. Many doctors won't accept it and you can die just waiting for an appointment. Studies have shown there was effectively one psychiatrist for every 8,834 Medicaid beneficiaries and just one cardiologist for every 4,543 Medicaid beneficiaries. These doctors can't possibly see, let alone adequately treat and manage the care of, everyone who needs them.
The closest we get to free healthcare in the US is care in the emergency room which is only required to "stabilize" you. They'll try their best to keep you alive if you're actively dying, but then they push you out the door and send you a massive bill. They won't give you chemo or radiation to keep your cancer from spreading
> That's because we subsidize the world by investing in a massive portion of the science and tech for producing medicines.
Even if we assume that's the case - as in, normal margins would be insufficient to finance the research - that does not account for the medical treatments themselves.
This is such a rotten take. America, saviours of the world. It entirely discounts the contributions that other countries globally make. Countries in the European Union, Australasia, etc.
The US cost of healthcare is about 17% of GDP. In other first world nations it's about 11%. This isn't service delivery or value, it's underlying cost. Per capita healthcare costs over twice of what it does in the UK. Similar for Australia. Both those are socialised and have very active R&D communities.
The average life expectancy in the US is about 78. In other first world nations it's almost unilaterally closer to 84.
The US is ranked 69th globally in terms.of health system performance. The US is also ranked worse than the OECD38 average for death by preventable causes.
The biggest difference between those places I mention and the above is that the US views healthcare as a capitalist endeavour and tries to claim that competition will lower prices. Quite the opposite has occurred, and the system has become perverted. Intellectual property laws applied in this fashion ensure that you cannot have competition for health care since drugs are limited to a single supplier. You also don't get a choice in hospital care or doctors in most cases when you really look at how medical competition works.
In other places, the costs are socialised through taxation. Drugs are purchased through nationalised efforts where suppliers must either come to the table and negotiate prices properly or lose access to entire markets. It's funny how they can still be quite profitable even under this scenario, and yet the prices still be so significantly less by orders of magnitude than US pricing per patient/dose.
American exceptionalism ceases to be felt when you go spend time in other first world nations for any meaningful length of time. You realise it's reassurance of self rather than truth on basically all but defence technology spending.
> The average life expectancy in the US is about 78. In other first world nations it's almost unilaterally closer to 84.
It doesn’t help that (at least when it comes to healthcare) US is a dozen of different countries in a trench coat.
Life expectancy in richer states like California or New York is very close to that in Germany, the Netherlands, Britain etc. (and if adjusted for the massive disparity in drug related deaths they’d probably be closer to Italy, France or even Switzerland) while the poorest states are about on par with Eastern European countries where it’s barely above 75 years or so. So any average figure is semi meaningless.
> That's because we subsidize the world by investing in a massive portion of the science and tech for producing medicines.
How much of the money that flows into the US healthcare system really goes towards medical R&D, and how much is effectively wasted due to the inefficient bureaucracy and out-of-control litigation?
> How much of the money that flows into the US healthcare system really goes towards medical R&D, and how much is effectively wasted due to the inefficient bureaucracy and out-of-control litigation?
Literally tens of billions are wasted annually on advertising. The cost is pushed to the sick and hurting while doctors are bribed to overprescribe whatever drug people are being trained to "ask their doctor about". I'd worry about that way before I gave a thought to "out-of-control litigation". Especially considering how companies like Purdue Pharma and Philips Respironics can knowingly kill people with their drugs and medical devices, try to hide the fact they were doing it, yet face no meaningful consequences and not one person is put behind bars. If anything, I'd say America should be demanding more justice from the legal system not less.
if US government is paying for research, advancement and what not, why should the end result not be free for citizens? let them spend a trillion dollars on a new drug developed by bayer or whoever, why should the company then charge anything more than say a generic paracetemol?
All research done using any amount of money from the US government should be open and easily accessible to every American (with exceptions for national security), but that doesn't mean we should get the products resulting from it without cost.
If the government funded research that resulted in a more eco-friendly car I wouldn't expect to see one delivered to my driveway or that the car with the fancy new tech (which might be a lot more involved in terms of costs) should be priced the same as the old tech.
Healthcare should just be made accessible and affordable to everyone. It looks like the best way to do that is with publicly funded health systems.
>I wouldn't expect to see one delivered to my driveway or that the car with the fancy new tech (which might be a lot more involved in terms of costs) should be priced the same as the old tech.
we often pay a new user tax, or monopoly tax like the epipen thing. that should not be possible.
Well, if the US decided to not offer medicine on a realistic price point, other nations would do what the US did with Germany's Bayer, back when Anthrax was a concern: Cancel the patent on the only Anthrax medicine available due to "national security".
Don't blame the world for your Pharma executives needing a third private jet for their mistresses.
It's a tragedy of the commons. US lawmakers need to ban pharmaceutical companies from selling their drugs in the US at substantially higher prices than the drugs are sold elsewhere.
I'm not so sure about rising levels of anti-intellectualism overall if you look globally. I looked at some stats over my lifetime and globally from Our World in Data 67m people had post secondary education in 1965 vs about 1.07bn now so up 16x. (https://ourworldindata.org/grapher/world-population-level-ed...)
Also in the 1970s the Cambodians were searching out their intellectuals and executing them and the Chinese did a slightly less extreme version in the cultural revolution whereas now you get none of that and China is becoming a science superpower.
Admittedly some in the US seem to be pushing antivax and climate denial but it's not like the past events. Also it seems a bit local. I'm a Brit for example and see almost no climate denial here. A bit of antivax maybe.
Some of the anti-vax movement during covid (I presume that's what you have in mind) is anti-intellectualism but some of it is not.
You can hold both opinions that an mRNA vaccine is an incredible new technology that has enormous potential, while a new technology that had never been tested on humans shouldn't be forced on people for whom the benefit was marginal at best (kids, healthy population under 50, people who already had covid).
And you can hold both opinions that health authorities clearly misbehaved or acted in a moronic way (lying about masks, origin of the virus, forcing vaccines on people who had already been infected, telling you you can't go outside, except if it's to protest for BLM, etc) while acknowledging that coming up with a vaccine against a new virus in only weeks is a technological wonder.
It's absurd to be systematically anti-intellectual, but also some healthy skepticism is well warranted.
It's like poker. You can have this lucky draw on the river, but most often you don't. You cannot built your strategy on lucky draws and those people weren't, even when not everything worked out. You and I are still alive, so I think they did a good job.
Right, a lot of the problem with anti-intellectualism is actually the people who define their viewpoint as The Science and try to shut down those who disagree as being "against the science".
its only been a small gap in time where anti-intellectualism was segregated from society. you could always just be in your tiny circles of elite higher education.
only thing thats changed this time is anti-intellectualism is given a microphone.
I think you'll find certain parties on both sides secretly want things to be framed as controversial to drum up the useful idiots to their cause or open their checkbook.
Fighting the symptoms instead of the cause isn't really pragmatic, in my view. But well, that's not really the website to have a real talk about the subject.
“For most people, experts say, the two tenofovir-based drugs — the first known as T.D.F., the second called T.A.F. — offer roughly equal risks and benefits.”
The Republic of Gilead is named for the biblical name "Gilead" for a region in Jordan[0]; the shot is presumably named for the Balm of Gilead[1], also named for biblical Gilead.
Descovy and Truvada are already more commonly referred to by their marketing names than with Gilead’s. Hard to see how this new shot would be different.
South Africa has one of (if not the) highest incidence of HIV in the population, so it makes sense to test it there. If you test it in a country where the incidence is 0.01 of the population, it's very hard to see statistical significance.
Edit: to add to my comment, it's also a phase 3 trial, so the safety has already been proven before.
They probably will, since they've extensively shared patents for their previous HIV drugs through the Medicines Patent Pool. It seems like you've fallen victim to some misinformation on Gilead or the pharmaceutical industry more generally.
Drugs in general are not tested on people in africa ("african people" is probably not the right term). More likely drugs are tested less in africa vs other places.
If you are talking about drugs for diseases that are a much more serious problem in africa than in the rest of the world - well doesnt that make sense? You dont test a new malaria drug in canada where there is no malaria. You test them where there is the biggest problem.
Globally, women and adolescent girls bear the highest burden of HIV, highlighting the critical need for effective HIV prevention options. In Sub-Saharan Africa, women and adolescent girls make up almost 60% of all new HIV infections. Stigma, marginalization, poverty, gender-based violence, and social inequities are some of the factors that have made women and adolescent girls especially vulnerable to HIV. PURPOSE 1, which enrolled cisgender women, will evaluate an investigational drug, lenacapavir, and an FDA-approved PrEP drug for people assigned male at birth, emtricitabine/ tenofovir alafenamide, also known as F/TAF or DESCOVY®, for PrEP. This trial is taking place in South Africa and Uganda and has completed enrollment.
I wonder what the existing breakdown is. If, hypothetically, all males had HIV already, then the new HIV infections would be 100% female. Obviously that isn't the case, just directionally this stat in isolation doesn't really show whether HIV is disproportionately affecting women.
Subsaharan Africa has the largest epidemic of HIV, that is why. Because you need a control group and compare the frequency of new infections.
It would make no sense to study HIV drugs in, say, Egypt, where the sexual mores are rather strict due to the conservative Islamic character of the society, and thus infection rates remain very low.
(Note that Egypt is also Africa, but probably the "wrong kind of"... at least as far as the fashionable racial classifications go.)
That's a legit question: drugs are now day tested in Europe on a relatively small and strictly controlled cohort and in China/India/Africa on much larger cohorts with much different rules.
It's easier and cheaper to test new drugs outside the us/eu because laxer regulations.
> It's easier and cheaper to test new drugs outside the us/eu because laxer regulations.
Given your comments elsewhere I suspect you're claiming this with no evidence.
For other readers, this isn't true / it's drug dependent. Amongst other things: difficulty sourcing the correct patients; difficulty importing drugs, particularly because they're not yet approved; difficulty getting high quality or reliable labs; etc. As any ctm could have told you.
As for this drug: the US/EU don't have rampant hiv, esp with the use of PrEP.
Or rather (due to obvious reasons) you just couldn't get a meaningful sample and would just be wasting resources/money if you conducted this test in US/EU.
Not really. When performing clinical trials, if you'd like to use the results of the studies in chinese/indian populations you'll need to prove bioequivalence in many cases, so you're going to need to collect a meaningful sample in the first place.
The reality is that most clinical trials aren't successes. If you can get a huge cohort of people for relatively cheap elsewhere, you can screen a lot of promising but doomed tests at a cheaper price point, then only re-create similar testing on the most promising candidates in your lucrative markets.
What the grandparent post was referring to as "obvious reasons" must be the high prevalence of HIV in the study countries[0]. Why wouldn't they test in countries with the highest infection risk?
There may be common reasons to trial there like it being cheaper or less regulated. But there is a good reason for this specific medication to be tested in those specific countries. Criticizing the study authors for being "cheap" is uncalled for in this case.
I'm not sure developed countries are the most lucrative market for HIV vaccines. How many people would even get them and why? This is a product almost entirely developed for Sub-Saharan Africa so it only makes sense that they focus on testing it there?
Hard to say, maybe it's not inconceivable that ~1% of potential patients in the US/EU/etc. might end up paying more than > 50%-90% of the people living Sub-Saharan Africa for whom getting the vaccine would make a lot of sense.
I'll try really hard to assume you're not trolling here.
I think it should be obvious that your suggestion doesn't work, because that's already an option right now... and it doesn't work. People's lives aren't neat and tidy, and people don't always do the safest things in the heat of the moment. Even if they want to, this kind of testing likely isn't available everywhere, or easily, or cheaply.
A twice-a-year shot is much more likely to be effective and actually used than ad-hoc, on-demand testing.
> ... unless you are extremely active.
Some people are. Are you suggesting that if someone is "extremely" sexually active, they don't deserve a reasonable, affordable way to avoid getting HIV?
> it's better to address the root cause—being hyperactive
If people want to be "hyperactive" when it comes to sex, that's their business, and there's nothing wrong with that. Measures that can make that safer are good things, not bad things.
Reading between the lines, I'm guessing you have some pretty puritanical views toward sex, and some misconceptions about the availability of healthcare and health-related testing in different places in the world. Maybe dial down the level of judgment, and learn a bit more about how people different from you live.
Given how much of a hot mess mass COVID testing was, and that was just a nasal swab, it is hard to imagine systematic blood draws for STI screening getting anywhere near feasible.
> there's nothing wrong with [a hyperactive sex live]
Well, clearly nothing except for the increased risk of STD exposure. I'm not GP and I wouldn't call myself puritanical, but let's not pretend like choices don't have consequences, and activities don't have risks. Yes, maybe the risk is more palatable for some, but when they knowingly take on that risk, they don't get to cry in conginitive dissonance about how their situation (STD) is not somehow a consequence of their choices (lots of different partners who are untested). In my opinion they knew what they were getting themselves into.
Now, yes, people are stupid, so it's good that backup options exist and are being developed. Still, let's just call it what it is: stupid.
I think the modern trend of acting like nothing is ever anybody's fault and consequences don't exist is very harmful. People need to take personal responsibility. And if they can't or won't, we need to recognize that for the bad thing that it is.
It's just this incessant infantilisation of people who are perfectly capable of reasoning and agency, where we pretend like nothing is every anybody's fault and therefore don't feel bad about it nor change anything about your ways.
And all of that is completely orthogonal to being either a puritan or sex positive.
Or maybe it's stupid to refrain from enjoying your sex life when the technology exists to enjoy it safely. All a question of perspective.
One thing's clear: there's nothing in your comment that's actually actionable. Sourpusses have been droning on about personal responsibility for centuries – and everyone else has been happily ignoring them. Making PrEP and other such treatments available will actually make a positive difference to people's health.
Yeah, giving in to our low level desires without doing some high level reflection on it is the easier thing to do. And statistically it is inevitable that at least some people some of the time act on it, so indeed maybe we should throw out the baby with the bathwater and all act that way so we don't get labeled a "sourpuss" when we talk about responsibility.
Look, I'm not arguing against backup options here. I'm just saying people should be as responsible as reasonably possible.
Edit: it's good that this exists. However, anecdotally: I know some promiscuous people and none of them are on prep. Some don't use protection at all because they are gay and there is no risk of pregnancy for them. When one person acts this way, it's their problem. When many people act this way, having sex at all becomes riskier for everyone. Recently, STDs have been on the rise. People just want to have fun and not feel bad about anything. They think they're the exception or something. And if you dare say something about it, you get called names like "sourpuss" or worse.
You mostly seem to be complaining about people who aren’t on PrEP. So you should be happy that there may now be an easier option for these people. It’s because you instead choose to complain about (literally!) people who have fun and don’t feel bad about it that you come across as a sourpuss. If you actually have some kind of concrete alternative proposal to making PrEP more widely available then I’m all ears, but you seem just to want to complain about people who have more than some arbitrarily-determined quantity of sex.
What I'm really complaining about is people with poor risk assessment and self control skills causing a tragedy of the commons for carefree sex, because people don't want to hear that they need to behave responsibly. In modern society it's pretty much a taboo to tell someone that they are too sexual, even when it's true and they are at highly increased risk for getting and subsequently spreading an STD.
I think you and I are in agreement about how awesome sex is. It's not about that. It's about people acting stupidly. I don't want a dating pool full of STDs but we're getting there. There's pros and cons to everyone leading a short-term-pleasure hedonistic lifestyle.
And yes, I'm happy about this PrEP development. Because when treatments and cures get better, it changes the risk calculus, and makes behavior which is today risky, no longer as risky or maybe even not risky at all.
I empathize with people who simply love to fuck a new body every week. They have their reasons for not picking a person and sticking with them. But I can't realistically say "well that's their business" because it's not just their business, it's the business of our whole society.
Food for thought: why is short-term greed looked down upon when it's about finances or business, but it's looked up to when it's sexual in nature?
You can wait for every human to change their behavior to fit your preferences (and disparage them until they do). In the meantime we can produce drugs that save lives until then. We can do both at the same time, so what's the problem?
> You can wait for every human to change their behavior to fit your preferences
No one has said or claimed that... and it isn't about "my" preference or yours; it's about the scientific approach to resolving an issue by addressing its root cause, or at least adhering to the 80/20 rule.
The issue here is exploitation. All I see is a greedy company trying to profit from a demographic instead of resolving the root cause, offering a "subscription-based" medicine. It's strange how all these new "breakthrough" medicines are supposed to be taken for life, like Ozempic. Meanwhile, the best prevention is to get tested in advance. It takes a few minutes and it's reliable, safe, and obviously cheaper than paying for pills/shots for life for the chance of getting that disease/virus.
If that medicine were a "treatment," on the other hand, then it would definitely be a breakthrough, especially if it's taken once, like some treatments for other STDs. Obviously, it isn't, and there's an entire business model built around that.
You seem to think the root cause is either "people have too much sex" and/or "people should have the foresight to always get tested at the appropriate time".
Both of those things are not root causes. The first is your value judgment (which others do not share, and there's nothing wrong with that; your moralizing around this is unwelcome), and the second is just a fundamental understanding about the availability of healthcare and people's ability to access it when they need to.
If there is any kind of "root cause" here, it's the existence of HIV itself. We should do our best to eradicate it, and taking every measure possible to help prevent people from contracting it in the first place is a good way to do that. Sure, some of that will be through education, teaching people to avoid risky behaviors, and get tested regularly if they're in a high-risk group. But creating vaccines and other prophylactics is also a good way of doing that, arguably even better, because it doesn't require that you educate everyone and change everyone's behavior. That never works all that well.
there is a lot of spontaneity in the act of sex that you're taking for granted; it's not that easy to throw that away and get the same thing out of the event.
rigor and standards are often the enemies of passion, so it's a hard sell. Your base logic is right, prevention is the best cure, but humans just don't work that way.
This is amazing, but surely I'm not the only one who is struck by the irony of a company called 'Gilead' who is trying to save the human race? (Handmaid's tale reference)
But maybe this company can incorporate all that in their market to targeted ad the nation’s schizophrenics, the ones that will draw a connection where there is none
Excellent news. HIV is nasty stuff. It acts sort of like an acquired genetic disorder.
It's a retrovirus, so it makes two copies of itself and replaces cellular DNA. Two RNA welded together make up DNA, so it more or less gives you the equivalent of a genetic disorder.
"Here's a shot, go have sex with people with HIV"? I hope the young women conducting the trials were compensated sufficiently for the risk taken, especially those who contracted HIV during the period.
Normally, some percentage of the population will get HIV in any given year. So what you do is give a bunch of people the shot and track them long term. You count how many got HIV after N years, compared to what would be expected in a normal population.
Nobody is exposed to HIV as part of the study, that exposure would come through the participants living their ordinary lives.
Close, but it's actually run with two large groups: one that gets the real shot, and one that gets a fake shot. You then compare the two groups, rather than comparing with the population.
That would be extremely unethical, exposing the control group to needless risk. There is already another drug that helps prevent hiv, it's called truvada. They tested this new one against truvada, and basically learned it's a lot more effective.
Who would sign up for your study? The diligent person already on truvada - would they risk getting placebo? No. Or the person too careless to take truvada? Would they go to the trouble of participating in a study for a 50% chance of protection? No.
Ethics and managing relationships with the public overlap.
But I don't think the particular aspect of "making sure you have enough participants" interacts very much with ethics. Especially when the failure state in question is an honest failure to attract them.
I think it would unethical if the participants in the study were asked not to take any other antivirals.
In that case, someone at high risk for HIV infection could be prevented from getting treatment because of the study protocol. The ethical solution, which the authors of the study chose, was to provide the highest standard of care as the placebo - in this case it was Truvada.
Since the treatment was actually even more effective than the existing standard of care, it was a home run success. Their conclusion is even stronger than it would be if they used a non pharmaceutical placebo, so in retrospect their decision was clearly correct.
In this case the study cites that as being unethical due to the high prevalence of HIV in the target population. So the actual trial gave some people the shot, and some other people the known-working daily pills as a control.
Here's the study page. https://www.purposestudies.com/purpose1/ and extensive details on clinicaltrials.gov https://clinicaltrials.gov/study/NCT04994509
It's double-blind so the patients do not know if they received the drug or an alternative. The investigators inform the patients of the risk and tell them to do what they would usually do. The participants must meet certain criteria including already being sexually active. The investigators would not tell the participants to be more sexually active, or active with more risky people than they normally would. The prevalence of HIV infection in the area is already fairly high so people are actively at risk already. I believe there was only very limited compensation.
I didn't think the question was unreasonable as some suggest and couldn't find an answer in any of the replies to you.
Poking around, it's my understanding that double blind procedure only covers treatment allocation--that is, who gets the placebo or not--and does not exclude general experiment communication to patients. I imagine trial communication is something generic along the lines of "We're running a novel drug trial, help us gather more data for $50/shot."
I don’t think the question is inherently unreasonable, but they asked it in a really flip and disrespectful way, and weirdly went with a very negative assumption. There’s also a whole field of medical research ethics and, I guess, it is hard to believe that somebody could be not aware of that (then again, I guess everyone has to learn it at some point).
Yeah, I asked it in a negative way, probably because I hold the view that Africa is the dumping ground for unethical behaviour/products. Just 2 months ago we were outraged at Nestle putting sugar in baby foods [0] in Africa. We have 2 kids, the eldest of which is addicted to sugar.
As a South African, I appreciate that we're also the most unequal country in the world (by Gini coef). So, some of what was going on in my mind as I read the Bloomberg piece, was:
* did they choose people at random, because the high HIV rate is obviously skewed towards vulnerable groups (think a young woman who's financially dependent on her boyfriend, who has multiple partners)
* just because the HIV rate is prevalent, doesn't mean that young sexually active people would have multiple partners, so how do they account for situations where we were sexually active, but with 1 or safe partners
* condoms are freely available in clinics and often public toilets, and we've generally gone past the fear of asking for them. So how does safe sex affect their study
> So, some of what was going on in my mind as I read the Bloomberg piece, was: did they choose people at random
They chose around 5000 people; they randomized them to either try the new shot, or one of two existing PREP drugs.
Of the 2000 people in the lenacapavir group, 0 got HIV, while dozens got HIV in the existing PREP groups.
When you have that many people and shuffle them, the groups end up pretty similar. You'd have to be really unlucky to get all the promiscuous people in the PREP groups.
PREP is already pretty effective; to have such a crushing result over PREP is a breakthrough.
i'm gunna bury this here, but pfizer said their tests in africa were 100% effective for the sars-ncov-2 vaccines.
It is in their interest to ... fudge the truth a little.
Now pfizer did this a different time by removing 2/3rds of the treatment group, and only counting "infections" if they occurred after all doses/boosters were administered. If you compare actual results to what pfizer published and claimed, you see that it was 7 infections in the placebo group and over 100 in the test group. they claimed <7 in the treatment group (i don't think it was 0, but it was like 2), and 7 in the placebo, saying "see, reduced infections by 80%!" Well, yeah, if you don't count infections and remove 2/3rds of the people who would have counted as infections possibly.
which means, and you don't even have to squint very hard, that the vaccine was actually increasing the chances of infection.
A lot of us are completely burned out and therefore wary on multinationals, regardless of their vertical. Pharma has a lot to answer for. Nestle has a lot to answer for. Chevron (et al) have a lot to answer for.
Instead, the vaccine and control groups were about the same until roughly day 10-12 after the first dose, and then dramatically diverged (though not as decisively as after dose 2).
unfortunately the source eludes me for my paragraph, but this https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10810638/ is some light reading although it has been retracted. however, it mentions a bit about it (such as moving people from placebo to treatment cohort and using those people in the data for the treatment cohort.)
I never made the statement that this was their South Africa (or africa) study. It isn't difficult to find the CEO of Pfizer saying their vaccine was "100% effective" in africa on twitter (there was a video, as well). that was my first claim.
Then i said "Now pfizer did this a different time ..."
edit: the source eludes me because i originally saw it on my cellphone in a video (the paper) and the bullet points were being read by an asian female. I failed to bookmark/save the video, and i have a hard time chasing down research that is this controversial without a DOI or PMC due to the ... tens of thousands of papers containing the same keywords.
I'm not claiming it's "buried" or "being kept from us" or anything conspiratorial, but it never got any play on mainstream media and would obviously get shadowbanned on any large site with funding from pfizer (et al) because of the "fact checkers want you to know that the vaccine has been proven safe and effective!" modal.
but i am done for today, i have to crack some hydrogeology textbooks so i hope this stays up so i have my own reference for the next time i mention this
> The trial involved about 5,300 women and female adolescents ages 16 to 25 in South Africa and Uganda, some of whom who received Gilead lenacapavir, and others who received older once-daily drugs from Gilead, including Truvada or Descovy.
Not to mention a superficial understanding of how drug trials are conducted would exclude that method.
They don't ask people to live their lives any differently than they would, nor do they expose anyone to HIV on purpose; they just track them assuming that x% of people get HIV in any given year. So they compare what X is for people who got the shot, vs those who did not.
As I skim TFA, they say nobody who got the shot ended up getting HIV, which would be statistical anomaly for the population they tested.
Twice a year, but yes. That's a huge benefit -- not only is it easier for patients to stay on the treatment, but it's likely to be a lot cheaper as well.
I wonder how much variation there might be in terms of margin of error. Like, how close do they have to get to keeping people on a rigid 6-month schedule? Would 7 be fine? For what percentage of people? I'm assuming they have reason to believe once a year isn't enough, so that's an upper bound, but what's the lower one?
> I wonder how much variation there might be in terms of margin of error.
Probably quite a bit. The trial used the same dose of lenacapavir as what's used for maintenance in HIV patients; it's quite possible that less is needed to prevent infection in a healthy patient. Unfortunately, there's really no safe/ethical way for them to test lower doses.
the short answer is no one knows (yet). if/once it gets approval, there likely would be a followup study on how much you can stretch the timing (possibly with dosage variation)
People are sexually active at different rates over different times, I also assume that a 100 people having sex with each other, where none of them have HIV, would not contract it.
It's like giving police officers new buller-proof vests, and then none of them getting in the firing line. You can't say that your vests are more efficient than other vests if they technically didn't get tested.
So, my thinking was how they ensure that all test groups are sexually exposed to other people with HIV, for the trial to be effective.
They don't need to ensure that all test groups are exposed to people with HIV. There is already a known risk factor for the specific population. All they need to do is see if the people who received the medication had more/fewer/similar infection rates as those who didn't.
Think about it like studies on which cars perform better in crashes. They don't need to have people drive more wrecklessly to determine if the car is safer. They just need to look at the expected risk compared to the outcomes of the people who drive that car. They are already doing the risky thing.
South Africa (study was in SA and Uganda) has an adult HIV prevalence of 18.3% and 210k new infections per year. It is easy to select a high risk group in which you would expect to see new HIV infections during the course of the study without intervention.
> So, my thinking was how they ensure that all test groups are sexually exposed to other people with HIV, for the trial to be effective.
They don't. Some people will organically have sex with people with HIV, and some will not. Your study just needs to recruit enough participants that it is likely some will. Your study absolutely does not tell people to deliberately have sex with HIV+ partners.
A while ago I watched this highly disturbing documentary produced by Vice about the prevalence of rape in the DRC as a weapon of war and terror against women. [1]. I have to imagine that this is involved, somehow.
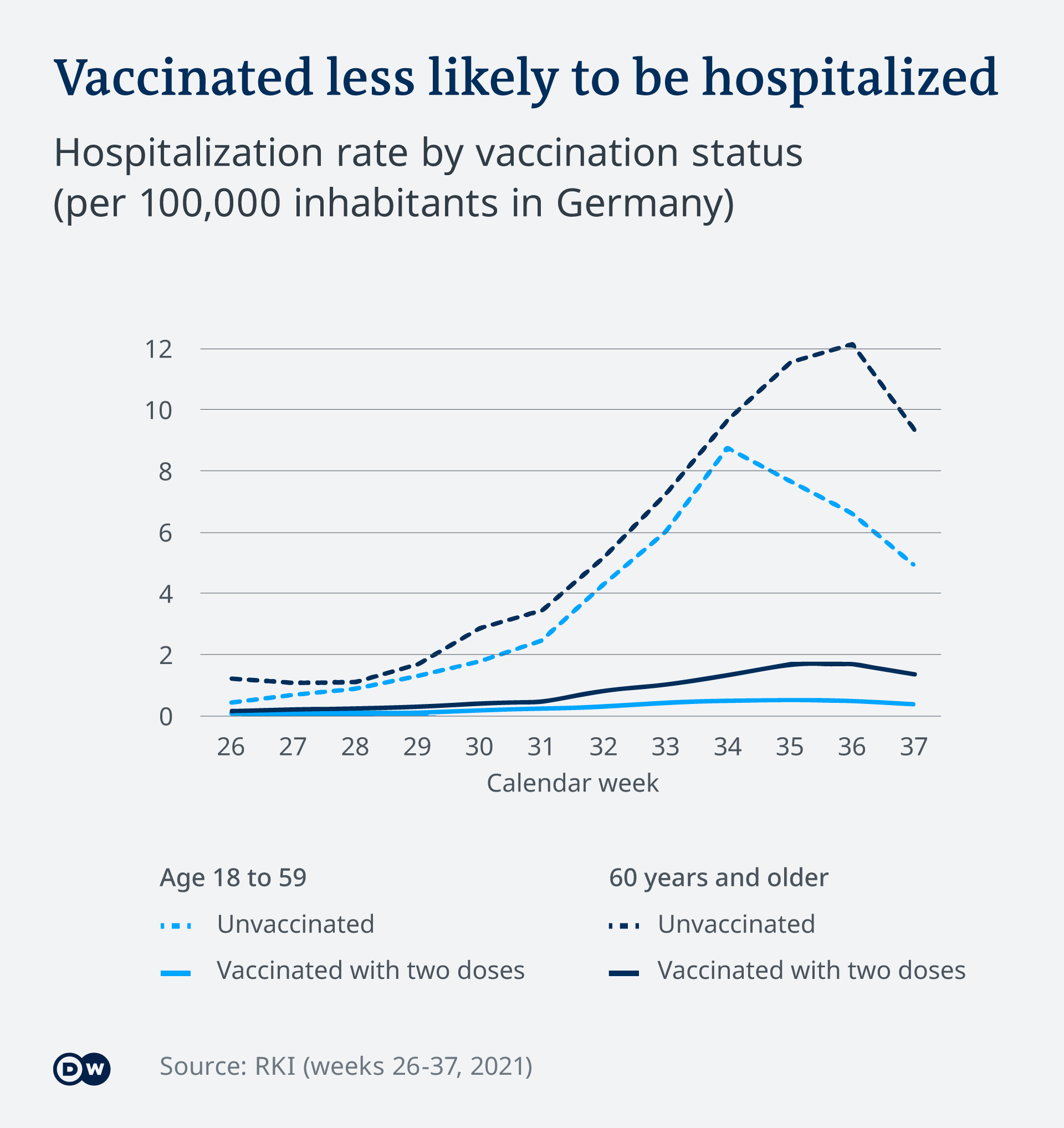{kind=link}
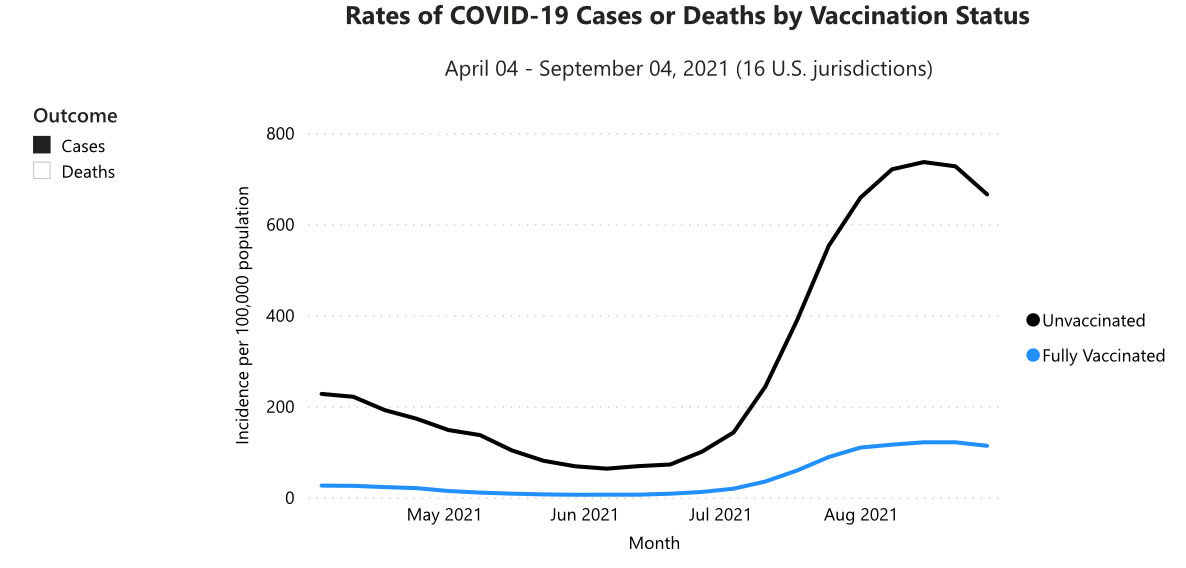{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Press release: https://www.gilead.com/news-and-press/press-room/press-relea...