I never understood how people bought into the whole "we assure you it's safe*" narrative. Unless, there's a secret time machine, there's no data (read: no science) to support such hyperbole. And yet, such statements were quickly followed by "...trust the science..." as well as attemps to marginalize those who asked to see that data from the future.
Such shenanigans doesn't build trust. It undermines it. As if gov and science need less trust at this point.
*effectively an untested type of vax technology is somehow miraculously free of any/all possible short and long term side effects? The comparisons to say the Polio vax were embarrassingly naive, at best. I don't get it.
I always said that the public health official must be absolutely certain they that all of the vaccines they were pushing are as safe and effective as they claimed before even considering mandating them. We now know they were wrong about at least one of them: the J&J vaccine is no longer being offered in my health system both because it's questionable safety profile and the fact that it is not as effective. Once we start preventing children from entering schools and removing people from their jobs (some with decades of experience) for not wanting to take a vaccine, the burden of proof is on the health officials to prove they are right. We also must remember that these measures have second order effects. I fear by abusing the trust the public had in physicians, public health officials have cause possibly permanent damage to the trust the average citizen has for the health community (this is especially pronounced among the underserved community).
a fast spreading pandemic vs. this or that public health measure.
the damage to the public health community is done not because of things like operation warpspeed, but because of the realpolitik of WHO, China, Trump, etc.
responsible participants have to take the time and effort to communicate with the correct framing: as new data comes in the best course of action can change, the current best is X, based on data D1, D2, ...
of course what ended up happening was random factoids sprinkled all over various media channels linked to local/state/federal/global decisions/recommendations.
government agencies are absolutely not up to the task of doing responsible communication to the public in this day and age.
Well, none delivered as promised. We went from "this will do it..." to "...get your booster boosted...and boosted..."
I get it. It's difficult to say. That's the true nature of science. The problem is, that level of honesty and transparency was completely abandoned. Instead we got "it's a pandemic of the unvaccinated" which was yet another hyperbolic lie. Instead we got Fauci suggesting "wear two masks" instead of coming clean (i.e., those disposable masks didn't have any science to support their effectiveness. That is, they're useless*).
These are not opinions. These are facts. Yet we're in collective mass denial??
*Why didn't we already know this? And why isn't anyone asking why that was?
The anti-vaccination / bashing of anti-vaxx people was a pretty big and one sided internet niche pre-2020. In a way that you did have some tinfoil hat people, you had some whistleblowers, and you had an army of people bashing them left and right. And we're not even talking polio, but with stuff like chicken pox, where there was a vaccine introduced, but the folk solution (locking up the sick kids with the healthy kids so everybody gets over it) were at conflict that turned super, super vicious.
In a sense it was an already ongoing battle with every argument already deployed and pre-determined, but all of a sudden everybody and their grandma were involved in the conversation against their will. The perma-online people predictably took up the positions they did, while a plethora of other opinions / skepticism emerged but were all summarily heaped in the tinfoil hat. Now it seems to be unwinding, and it feels just as surreal as the last few hours of a rave where everybody is kind of sobering up and looking at a very bothersome way home.
> Is a terrifying admission about the gamble that was taken.
Right, but according to Reddit, the Australian/New Zealand governments and other places people who didn't want to expose themselves to this stuff where all ignorant selfish assholes.
I think you might have been browsing an alternate-reality Reddit. The one I read was constantly bemoaning that no one in America was taking it seriously, "why aren't we locking down like China and New Zealand", etc.
It's strange to me how so often you will see people bemoaning Reddit for some opinion that goes against the grain, when in reality Reddit is composed of a sampling of millions of humans and therefore is fully aligned with mainstream thought. Some people see a few comments or threads that disagree with them and they use that to say "All of Reddit has lost its mind", always forgetting the vast numbers of comments and threads where people generally agree with them. Funny how people do that..
Reddit is a sampling of roughly 20% of 18-29 year old men who use the Internet. That’s not exactly “mainstream thought”, it’s a self selected demographic and what is popular on Reddit reflects that.
> and therefore is fully aligned with mainstream thought
It's obviously not fully aligned with 'mainstream thought', when the expression of many widely help positions will get individuals and whole subreddits banned
Almost every single biomedical paper includes a line that says "more research is needed" because one of the main goals of research is to figure out what research to do next.
Why is everyone voluntarily practicing amnesia? We had a lot of trial data showing safety and efficacy before the vaccines were rolled out.
It is standard practice with influenza to update the stains. 0 reason to think that updating the mRNA for COVID vaccines from one strain to another is dangerous. None. Zap. Zero. Zilch.
Vaccines for influenza have been around for decades. The first covid shot was the first ever mRNA technology ever approved for human use.
Now the booster doesn’t simply swap out strains. It moves from a monovalent to a bivalent (original formula plus the Omicron Ba4/Ba5 formula) and we shouldn’t test it? The first ever bivalent mRNA vaccine. Deployed to everyone on the planet. With absolutely no human testing done.
If you’re okay with it, that’s great… that’s your personal choice to trust corrupt health authorities and for-profit vaccine manufacturers. Let me know how it goes.
The ba.4/ba.5 is not the first bivalent mRNA vaccine. The ba.1 bivalent vaccine was the first, which has been studied in a larger population than the ba.4/5 bivalent vaccine.
The FDA instructed Pfizer and moderna to reformulate based on the changing variant landscape as ba.4/5 overtook ba.1
The ba.4/5 bivalent vaccine was an extremely incremental change from the ba.1 booster
I can't recall seeing any human studies on mRNA vaccines before the Pfizer one, which was unblinded and the control group vaccinated after six months. I also don't understand why this was done, since there will never exist any long term high quality data because of this.
> It is standard practice with influenza to update the stains.
A questionable one. Depending on the year, getting the influenza shot has been shown to give you negative efficacy. How nice would that be if we saw a -50% efficacy this year, wouldn't that be problematic for our strapped healthcare systems.
> In the 2014-15 season (when, as mentioned, the vaccine was unchanged from the year before and a drifted H3N2 strain was circulating), "negative effects of prior vaccination were pronounced and statistically significant," the researchers found. VE in those who received only the 2014-15 vaccine was estimated at 65% (95% CI, 25% to 83%), whereas VE for patients vaccinated two seasons in a row was -33% (95% CI, –78% to 1%).
How am I spreading conspiracy theories? You suggest to grandfather the covid shots on the coattails of the flu shots but are not concerned about the combined potential for negative effectiveness on future variants as seen happens some years with the flu shot and the increased infectiousness of sars-cov2 as compared to flu?
Are you thinking that the 2014 flu vaccines were released with the understanding that they would have negative efficacy for those who'd had the prior years vaccines? Why would they have done that?
This is an incredibly common expectation, and the only reason people took exception to it is because they dislike the government telling them what to do. Interesting I never heard from grandpa rail against the military for the vaccinations he was forced to get in the military...
You are comparing the volunteer military, an organization where the government controls its enlistees every move / food / clothing literally all parts of their life... to the life of an every day citizen?
I had COVID twice before I had the chance to get vaccinated. I then thought I’d wait for the new vaccine for my busy wedding season that’s starting now.
Too bad it’s just a booster and I’m not eligible to get or because I haven’t gotten the probably essentially useless (for me) original vaccine. As far as I’m aware they didn’t announce the details of this until sometime in August. At this point by the time I got the booster that might provide me some protection the virus will probably have mutated again.
> no evidence of long-term immunity after an infection
Define immunity, but there is absolutely evidence of long term effectiveness against hospitilization and death if you care to look for it.
"No evidence" doesn't mean we looked for it and it doesn't exist, it means we didn't look for it yet or have chosen not to look into it. In this case you seem to be citing ancient talking points from before it was possible to tell how long lasting the immunity from covid would be, AKA in early 2021 they couldn't state for fact that immunity against severe death would last longer than a year because the disease itself was too new, (although sar-cov1 was known to have long lasting immunity 10 years later, but lets pretend we didn't know that it would work the same). Now we know because the disease has been around long enough to gather those types of statistics.
> Virus-specific B cells increased over time. People had more memory B cells six months after symptom onset than at one month afterwards. Although the number of these cells appeared to reach a plateau after a few months, levels didn’t decline over the period studied.
Take the above snippet for example. From this you could make the statement "we don't have evidence for natural immunity lasting beyond 8 months" But that is explicitly a limit coming from the length of study.
I fear you've avoided mine. There are verifiable reinfections. Covid-19 is probably going to celebrate it's 3rd birthday in a few weeks maybe even a few days from now and Omicron has reinfecting for the entire year those that have had other Covid variants before.
I'm going to demonize the person that thinks they don't need a vaccine.
Like I said, define immunity, I presumed protection from severe disease or death, for which prior infection hold quite well. Mild symptomatic infection is not generally avoidable vaccinated or otherwise.
> I'm going to demonize the person that thinks they don't need a vaccine.
We're pretty much done with the culture war side of the COVID vaccine debate, so perhaps we can now discuss whether there were unknowns that warranted investigation without the vitriol. I myself had no hesitation taking the vaccine, but had the same response as OP to this study. I don't regret getting vaccinated, but in hindsight, I should have been a bit more charitable towards those expressing concern.
Are you new to the Internet? Arguments over putting pineapple on pizza cause vitriol.
Jokes aside, the summary admits more studies need to be necessary. From what I understand of it, it made mice stronger against flu, but may have made them weaker to other infections. This is big if true, but it requires more study.
It was aspirational not an expectation. Alas, the downvotes show me that I'm doomed to yet another disappointment :p
> This is big if true, but it requires more study.
That's basically my point. I am saying that I would have (apparently incorrectly) assured people that more study was not required - at all. I and many others probably overcorrected for the skepticism of "the other side". It doesn't change my opinion that the vaccine program was the right call.
I live just down the street from a 'memory care' center for seniors with dementia, etc. There are about 120 'guests'. In two weeks they lost 45 elderly patients, and one nurse due to COVID. And today people are still arguing about the vaccinese. there are literally more than a billion people vaccinated for right near 2 years now. Still no serious data about problems, but people feel like it was dangerous to encourage their use. I wonder what their threshold is for when its finally okay?
It's confirmation bias in its purest form. They welcome any small piece of evidence suggesting that vaccines carry risk, while rejecting any evidence to the contrary or that the benefit outweighs the risk. They're not having an honest discussion.
> But yeah lets talk about how maybe possibly 10+ years from now there is some repercussion...
And will any of these repercussions be significantly worse than having gotten a mild case of COVID the natural way? We do not know what COVID will do to us in 10+ years even after a mild case. Anything from nothing at all to organ failure to whatever else...
Or maybe like measles in 10 years time loads of people who caught it "naturally" will drop head from an incurable encephalitis that kills them.
We just don't know, so we make reasonable guesses. Consider the harm we see happening weight then more against the unlimited possibilities of harm we can imagine.
People were by and large happy to have a new vaccine today and risk some unpredictable future risk than die of a disease they saw killing people.
I think some people just can't wrap their heads around balancing these kind of risks.
> The vaccine was 95% effective in preventing COVID-19 disease among these clinical trial participants with eight COVID-19 cases in the vaccine group and 162 in the placebo group. Of these 170 COVID-19 cases, one in the vaccine group and three in the placebo group were classified as severe. At this time, data are not available to make a determination about how long the vaccine will provide protection, nor is there evidence that the vaccine prevents transmission of SARS-CoV-2 from person to person.
> “Obviously, with a 90-plus percent effective vaccine, you could feel much more confident” about not getting the virus, Fauci told Tapper. “But I would recommend to people to not abandon all public health measures just because you have been vaccinated.” Those fundamentals include: universal wearing of masks, maintaining physical distance, avoiding large crowds, doing more outdoor activities and washing hands frequently.
> Because “even though, for the general population, it might be 90[%] to 95% effective,” said Fauci, “you don’t necessarily know, for you, how effective it is.” Even at those success rates, about 5% to 10% of people immunized may still get the virus.
It's absolutely wild that people complain about 95% efficacy against Delta, or about the gradual rate of decay that successfully kept a lid on COVID until the later, gentler variants dominated.
Yeah. I don’t get the parents point either. The vaccine doesn’t prevent catching COVID like the measles shot does, it only reduces symptoms.
Almost everyone who’s been vaccinated has ALSO caught COVID. So those of us with the vaccine have to worry about the long-term risks of both the mRNA vaccine, in addition to the long-term risks of the disease. Those who skipped the vaccine only have the theoretical long term risk from COVID to worry about.
If there are repercussions to the immune systems of vaccinated people 10 years from now then we have a big problem. The "maybe" and "possibly" qualifiers don't diminish the scenario where there are actually problems.
> mRNA was in studies prior to COVID, its not like we made it up in 3 weeks.
Part of the reason it was in studies for so long is because it kept failing. But in two weeks (seriously! That's straight from Moderna) they were able to button everything up and make it work for Covid.
The only reason it wasn't developed before COVID was because it wasn't a profitable improvement over other styles of vaccines. It was literally a business decision to not develop it more.
No, mRNA tech wasn't being used before COVID. They were trying to bring it to market and failing. That's why so many people refer to it as experimental.
Just because 10 million kids lost their caregivers doesn’t mean masks work, or making toddlers wear kn95 masks at preschool works, or any of our NPI’s work. It also just mean that even if they did work they’d be worth the cost.
Yes Covid is a tragedy. I think most people recognize that. That doesn’t mean what we did worked or should have been done.
Nothing in that study says what to expect prognostically. Sorry, but there's little reason to think that staying at home rather than school has forever harmed children.
The pandemic was hard on everyone. Blaming school closures just reveals your personal vendetta.
>The COVID-19 pandemic has produced high morbidity and mortality rates within the global population,39 as well as risk factors for healthy growth and development among children. The increase in parental stress, the suspension of classroom activities, social isolation measures, nutritional risks, children’s exposure to toxic stress, especially in previously unstructured homes, and a lack of physical activities are some of the factors found in the literature.
Yup, this seems pretty obvious anecdotally so its good to see it being backed up in the literature.
Was it worth it to save the lives of 100's of 1000's to millions of elderly people? Probably.
Did it negatively impact the younger generation, who had no say at all in the decision? Absolutely.
I think the 'was it worth it' has to be answered by the our community over the next 10-20 years.
We made a choice, right or wrong, to sacrifice some of our children to save our elders. Culturally, this is not something we do. I wonder how this will be interpreted as more of these studies come to light and the children start to age and we can see the damage.
Society constantly trades off the well being of kids vs people that are older than kids. This is totally something we do. Funding for education vs funding for something else. Streets that are safe for kids vs ones that are convenient for driving fast. We're happily screwing over entire generations with our carbon based economy.
We already know we made the right choice because the alternative was 20 million more dead. This "time will tell" bullshit is ridiculous. We swerved the car to avoid crashing it head on into a wall, and yes you might have whiplash but there is no honest room for second guessing the decision not to drive the car into the wall at full speed.
I'm sorry but that is not how science works. We will be studying this for years and changing healthcare policies as a result of this. Its not "second guessing bullshit" its looking at what happened, the results of it, and changing our future actions accordingly.
There is an entire branch of study - one which I work in - whose entire job is to run either observational studies or post-hoc studies using real world data to find out if something had an impact, a positive impact, negative impact, and what the likelyhood of your own study being correct is.
If you think this is 'done' and we shouldn't revisit this to see what we did well / did poorly then that is as anti-science as they come.
With all due respect, further tests, research, and outcome analysis on the people impacted by our choices will be how we understand our response and what we should have done differently.
You are lumping every response to the pandemic together and appear to be saying "you can't judge this, would you rather millions have died??" - well no, but thats not the question either. Instead "We did things to respond to the pandemic, some good some bad. What was good and what was bad."
This will happen. Saying "NO NO NO" is not going to stop that or help it.
We didn’t “sacrifice our children”. At worse they may have a harder time catching up at the price of having older relatives around longer - who if nothing else often provides free health care so parents can go to work.
This is such a privileged take. We stole proms, graduations, first dates, first days of school, friendships, relationships, social interaction, you name it… we stole it from our kids.
Maybe rich tech workers had it easier or are living in denial but the fact is what we did to the young is completely disgusting and it is shameful how quick some people are to dismiss it. What we did to kids was state sponsored child abuse. We absolutely fucked over their one and only childhood for a disease whose median age of death is higher than the average life expectancy for a normal person. The number of young ones who got seriously ill from Covid is a drop in the bucket.
So it’s a “privileged take” that it’s mostly poorer families who wouldn’t be able to afford child care and would depend on childcare from their now dead older relatives?
Yes it’s more concerning that poor little Timmy couldn’t have his first kiss than granny actually ending up dead.
If you haven’t prepared your children to handle a little inconvenience like not going to a prom, he’s certainly not going to be prepared for real life.
'Millions of dead' vs 'no prom'. As if prom means anything. As if it's some essential thing that was always a critical part of human life and children are considered "sacrificed" if they have to go without. Ridiculous. Talk about privilege!
Sadly, things during the deadly global pandemic have been less than ideal. Nobody asked for the pandemic and nothing we did or could have done differently would have changed the fact that it was going to have an impact on children just as it has had an impact on all of us. You just can't have a deadly global pandemic and not disrupt people's lives somewhat.
Ask any kid who lost a parent to covid if they'd rather have prom, a 'first days of school' immediately instead of later, or their loved one back. Imagine how many more parents (and children) would have been killed or suffer long term problems due to the virus if we'd done absolutely nothing like many seem to have wanted.
I wonder which kids are going to grow up and think back to this time and feel more abused, the ones whose parents did everything they could to protect them in the middle of a pandemic or the ones whose parents told them not to wear a mask and wouldn't get them vaccinated and wanted to shove them back into schools no matter how many children and adults got sick.
Our preschool is composed of 3 year old kids who never played with anybody outside their family. Many haven’t seen a single strangers face for years. Many have serious behavioral issues and speech issues. Saying “kids are gonna be okay” is such a line of bull.
Even if all that crap we subjected them to worked, that still doesn’t make what we did to them okay. We stole significant chunks of their one and only childhood away from them for a disease that they aren’t even close to being at risk from.
We absolutely fucked our kids and it is perhaps one of the saddest most shameful outcomes of societies myopic fixation on Covid.
Is it really ridiculous to consider the impact that massive societal changes we made might negatively impact our young? Zoom school, or even being in school masked and socially distant seems objectively worse for young children than being in-person and able to watch facial expressions and read lips. Why is it hyperventilation to consider the aggregate impact this will have on the generation of children that effectively lost 1-2 years of in-person social development time?
You can’t prove that what we did to children saved millions and millions of lives.
Frame your argument in terms of quality adjusted life years and the whole thing falls apart. The median age of somebody dying of Covid was higher than the average human lifespan. What kind of sick demented society steals two or more years of little kids childhood for that?
Oh can you prove that keeping schools open would NOT have resulted in even more mass death than we have already experienced? What about the millions of children who lost parents?
I never thought I would see “think about the children!” used like this. No worries, little Timmy will be fine. But what do you think will happen to the children when their caregiver dies since grandparents and other older relatives are one of the primary source of free childcare?
My 80 year old parents are not in the nursing home. My 80 year old dad still spends all day doing yard work and he still does karate katas to keep limber.
Most older adults are not living in nursing homes.
>The reality is, way more people would have died without the vaccine
You can't and couldn't possibly know that. Nobody could. What we do know today is that the un-vaccinated aren't dying like was originally claimed they would, in fact they seem to be faring better for those under 60 or so.
> You can't and couldn't possibly know that. Nobody could
Not with that attitude... Yes you can, there are plenty of ways of comparing regions or countries with high and low vaccination rates, or vaccination uptake. (Of course only while demographically adjusting, but the people who do these studies surprisingly often do think about the basic gotchas.)
I am going to leave age out of it as I don't participate in the "fuck-em they're over the age of 55" mentality.
The incident of death does increase substantially past 55, however people died at all ages during covid, so we know more infections = more deaths across the board.
Given that the vaccine available at the time resulted in around a 85% reduction in likelyhood of infection, we can for sure declare it saved many more lives than without, unless it directly killed more people than it helped...
>un-vaccinated aren't dying like was originally claimed they would
Oh man what a gotcha! If only there was some sort of change in circumstances that could impact how many people will die from a new disease, like I don't know, new less damaging variants and significantly better care in facilities that are no longer buckling under the burden of thousands of cases a week.
Probably one of those tabloid pieces saying something like "80% of the deaths are now among the vaccinated" - which ignore that the population vax rate in that country is higher than that.
People in the western societies will do anything to avoid wearing masks. That includes pushing and taking vaccines that weren’t fully tested. Unlike the latest flavor of mRNA vaccine, masks do not lose efficacy against new variants within a few months. If you wear an n95 rated mask or higher, you will have 95% efficacy or higher
masks work, but their end-to-end efficacy is very low, because people would have to wear them perfectly.
there's no point to wearing masks if you go to places where you take it off. people did exactly that and everyone was pikachu surprised that the pandemic was still alive and well.
That’s not true. Even an imperfectly worn N95 is more effective than a cloth mask or nothing at all. The n95 mask is high intuitive unless you have a large beard (ie. you just have to ensure it fits your nose bridge area and chin area properly). I would wager that it still has better efficacy than an mRNA vaccine even when improperly worn
2. People use garbage cloth or surgical masks that have poor efficacy. Those masks at best are only effective in partially protecting others if you’re sick, but not vice versa.
3. For the reasons stated above, these studies don’t disprove the efficacy of n95 or higher rated masks
Unlike cloth masks, n95s and higher rated masks have much better efficacy and I have yet to see a study that either focuses on them or differentiates them from near useless masks. A better study would focus on hospitals and their workers’ use of different types of masks. The current studies just help prove my point. Hating masks is something people on both sides of the political spectrum can agree on in the West
I had masks at home well before COVID stuck, mostly for protection against dust and whatnot. Saw how HongKong took desinfection quite seriously, saw how SARS went down.
And still, as long as we don't magically come up with a way to educate millions of people effectively about masks, mask mandates are a wash. (Their best benefit is that anyone who gives a shit does not look like an outlier.)
For the record, I’m not pushing for mandates. They will fail.
I’m just saying that n95 masks are highly effective at preventing the transmission of airborne illnesses such as COVID regardless of whether anyone else wears a mask, along with my observation that the West detests masks ie. I’m not recommending a solution. I’m lamenting the stupid and illogical behavior of people, even educated ones
However, I hope that lessons about human nature have been learned, now that we have all lived through the pandemic. Whenever we look at history and ask "how could people buy such a flimsy story, and abandon all that they previously held dear?", the answer is "willingly, enthusiastically, and they will turn in previously good friends and family to further the supposed moral ends".
> On the other hand, we report that after pre-exposure to mRNA-LNPs, the resistance of mice to heterologous infections with influenza virus increased while resistance to Candida albicans decreased.
It sounds to me as though the tradeoff being made here is: a slightly decreased immune response generally, but a better immune response to the thing you've been immunized against. That seems to be a reasonable tradeoff if there's something really bad going around.
But as they say in the paper summary: more research is needed.
Also: this is purely in mice. They have zero data on whether this is true for humans.
I donno. Seems like white blood cells are kinda important.
We have a huge number of interactions with bacteria and viruses and all sorts of microorganisms. Hundreds? Thousands times a day? Scratches in the kitchen while preparing food, for example, floods our body with stuff that white blood cells are required to deal with.
Giving up some of the ability to deal with those for a small reduction in the symptoms associated with a specific disease doesn't seem like a useful trade off.
Dishonesty can never satisfy intellectual curiosity. It’s not an insinuation, it’s a scientific possibility that warrants further investigation, especially when boosters are being rushed to market with similarly abbreviated clinical trials. There are some reasons for suspicion. One is the rapid fading of the vaccine’s effectiveness. Why is it so much faster than expected? What’s the mechanism? Another is that every other coronavirus vaccine tested has resulted in decreased immune function due to Antibody dependent engancement. Do we know the current vaccines cause ADE? Not so far as I’m aware. Is it something that should be researched? I’d say so.
Not being aware of any research about ADE doesn’t mean it hasn’t happened… There has been a ton of it and it tends to be something that shows up pretty evidently in clinical trials.
If you do a Google Scholar search for COVID vaccines and all-cause mortality, you'll see that in most studies, people who got vaccinated die less in general (i.e. counting deaths from all causes).
Population level or absolute increases in deaths do not tell you the marginal impact of getting vaccinated. For example, there's no contradiction between both vaccinated and unvaccinated dying more and vaccines being protective.
If you select for careful, risk-averse populations, you'll see correlary effects of your selection and theirs, irrellevant to the measure you're taking.
People are dying at rates well outside historical norms. Things have causes. What is the cause of people dying more?
One would think after a pandemic with an outsized effect on those already in a moribund state that overall deaths would be down, but they aren’t, they are up. Why is that?
Why are excess deaths higher after rollout of the mRNA injections than before?
Nothing about it adds up, other than one sacred cow elephant in the room.
If people are dying more, there is a cause for that, people have tried everything they can that doesn’t involve going down sacred cow avenue, and they’ve come up empty.
Can be seen in the European data. Excess mortality should be back to normal levels, but it's barely changed between 2020, 2021 and 2022. Worse, older people do seem to be doing better but younger age groups worse.
> People are dying at rates well outside historical norms. Things have causes. What is the cause of people dying more?
I suspect it's your preexisting bias that makes you assume it's vaccines vs any vast number of other possible explanations. The point is, that we don't know what is driving these deaths. Research should be done, and if evidence turns up which suggests it's more likely vaccines than most other possibilities then sure it'd make sense to say vaccines may be the cause. Do you really think we have enough evidence pointing to vaccines being the cause right now? If so, where is it?
Until we have more answers it's impossible to say what the cause is, but what we do know and have evidence for is that Covid has become extremely (and unnecessarily) politicized, that data on the number of cases and deaths have been being interfered with by government officials, that there is a very strong economic incentive to get people to act in ways that could cause them to get infected, and that people who have been careful are growing tired of the restrictions being safe puts on them as well. We absolutely should expect uncertainty in the number of cases and deaths we see reported, and that could result in some amount of increase in excess deaths. So could complications not directly attributed to the virus, but caused by it still.
We've also got a whole lot of people these days drinking poisoned water and people who don't even have drinkable water. I can't even keep track of the all the cities that are under boil water orders. We've got people without power. We've got areas of the country flooding, other areas that on fire, people living in extreme poverty (including those who lost their job due to lockdowns or their ability to work because of long covid or their household income due to illness or deaths).
It seems like if there's one thing we're going to have to start getting used to it's increasing amounts of death. With so many causes throwing their contributions into the mix it's going to take time to sort it all out and we'll have to do it in an environment where at least some of the data is being manipulated and many people have their egos wrapped up in "taking sides".
Personally, I accepted the possibility that the vaccines could have terrible effects down the road (it was clear enough that there were no major issues in the short term) and I came to terms with that ages ago. If it does start to look like the vaccines have done some great harm then at least I can say that the choice to get vaccinated was easily the best that could be made with the information I had at the time. Sometimes you can make the right choice and still end up screwed when new information is discovered. I'm still hoping that doesn't turn out to be the case here, but if it is there's no point in denying it. Pretending it isn't true if it is would only make it harder to try to fix it (if that's even possible).
There are three things that have changed since the number of deaths went up in 2020.
Covid, lockdowns and the associated harms and the vaccine. Now apparently covid deaths are down, yet excess deaths remain elevated. So the two obvious changes are a rushed "vaccine" with what appears to be fraudulent trials and lockdowns causing delayed diagnosis, treatment or suicide.
It should be easy to compare vaccinated to unvaccinated groups to find out if the vaccine is causing problems. But rather then do that, the authorities have done their best to destroy the control group and coerce everyone to take the failed "vaccine".
Excess deaths are widely considered to be “from Covid” right now. It is possible there’s something else going on, but as the parent said, the numbers you should care about when making a vaccine decision are the mortality rate of the vaccinated vs the unvaccinated.
Unvaccinated people are dying at a much higher rate. If your biggest concern is not dying, you should be vaccinated.
I was going through serious medical issues when I lost access to my doctors from Covid.
I got lucky in that the 20th medication they tried just before lockdown ended up working. Would most likely probably be dead if things had shut down a month earlier.
Tons of people in support forums were in a panic over lost access. Needed testing / procedure.
Not fun when brain is swelling and doctors say they can’t see you.
I have loved ones that suffered similarly. I do not doubt there were excess morbidity/mortality from restrictions. I'm not doubting, but there is a ton of nuance in epidemiological data like this and I'm wondering about things like demographic cuts and magnitudes of numbers which are necessary to understand the statement.
And, likewise, you cannot NOT attribute them to the vaccine.
Inconclusive data is not to be either used as a calibrated measure nor to be simply ignored.
The excess deaths are quite possibly attributable to both the virus and the vaccines if, as one plausible but very unproven example, they're due to inflammation and/or micro-clotting caused by the spike protein. But in an environment where everyone will be exposed to the actual virus eventually, with uncontrolled initial exposures, it comes down to whether the benefit of getting vaccinated is worth the risk. The data I've seen says that it is.
There are large crowds that took 2 doses in pandemic period (getting vaccinated properly back at the time) but not receiving boosters.
It would be easy to track:
- 2 dose, no other booster
- all boosters
- no vaccine
and readjust results considering age and other bias etc.
If all booster people have excess deaths, than "not from Covid" ?
If 2 dose people excess deaths < all boosted people, than something about vaccine?
No vaccine could be control.
The unvaccinated have been receiving lower quality of care. The symptomatic have Been diagnosed without PCR accuracy. The data being collected is bad. Let's not treat it as good data, and see assumptions such as this for what they are, which falls in the "not good data" category.
> Excess deaths are widely considered to be “from Covid”
Considered by whom? The funny thing is that there was no non-covid excess mortality in 2020, that stated on 2021, which is the same time the v{censored} started.
> Unvaccinated people are dying at a much higher rate.
Insurance companies have already begun publishing reports indicating that excess mortality rates are inversely related to vaccine adoption (i.e. higher excess mortality in states with lower vaccination rates).
Thanks. Very noisy data, so I'd say far from conclusive, particularly given the confounding variables that differ between states. Still, the best attempt I've seen to actually look into this issue.
Countries like the UK have national vaccination databases. They could easily put this issue to rest with a study of excess deaths by vaccination status, controlling for age/health/etc., except they conspicuously have chosen not to.
Starts on page 33, for any one else curious at looking. Quite interesting to see what appears to be their hazard ratio relative to the state population: their members have a much higher excess death rate, and their members show minimal correlation to the vaccine rate of the state they are in—presumably reflecting that older, sicker, or more health-conscious people opt in more often to buying health care plans?
Do you mean “Weekly number of deaths (from all causes)?” If so that is such a junk chart I don’t see how it supports either claim. The X axis label is absolute garbage. It’s completely unclear where the new year begins. A naive reading (counting back from 2022) has the excess deaths starting in 2019!
1. That wasn't a controlled experiment. Observational data < RCTs.
2. You are mixing up mortality and mortality attributed to COVID. It's a common error. For overall mortality the picture is far less clear. For example in the Pfizer trials there were more deaths overall in the vaccinated arm than the unvaccinated arm i.e. RCT evidence = no mortality benefit.
Also, we now have excess deaths above the expected baseline for long periods in 2022, which is unprecedented. Governments are highly reluctant to split these deaths out by vaccine status, but the increase seems mostly attributed to heart and blood clotting related deaths. So the data from the "experiment" is not obviously positive.
>You are mixing up mortality and mortality attributed to COVID.
There's also the problem of governments playing funny games around deaths and "vaccinated". Someone who died from an adverse reaction immediately following their shot would not count as a vaccinated death, because the _definition_ of "vaccinated" meant you completed the vaccine schedule which was multiple shots over time.
In trials the vaccines were tested in tens of thousands of people where adverse reactions were meticulously recorded and there just isn’t any evidence that the vaccines caused immediate death in anybody.
Then beyond that there isn’t any evidence that there also is a government conspiracy following the first dubious claim.
> For example in the Pfizer trials there were more deaths overall in the vaccinated arm than the unvaccinated arm i.e. RCT evidence = no mortality benefit.
> Governments are highly reluctant to split these deaths out by vaccine status, but the increase seems mostly attributed to heart and blood clotting related deaths.
There were approximately 40k people in the vaccinated and the placebo groups. One group had 17 deaths, and the other one had 21. If you are not aware of this information, how can you consider yourself informed on the topic?
There is a pretty good reason that the Pfizer RCT doesn't show excess mortality benefit. It wasn't designed to study that. The recruited population is mostly healthy as individuals with multiple risk factors were excluded. For example the proportion of the study group over 65 and the proportion with at least 1 comorbidity is much smaller than the population as a whole. The studied group was very unlikely to experience mortality in the first place so a much larger study would be needed to show any evidence of an effect on mortality. The difference between 17 and 21 is not statistically significant.
In the absence of a large enough RCT we're left with observational studies and there are a ton of these now. The observational data shows a large mortality benefit in the vaccinated population and I'm not aware of a single observational study that shows the opposite, but I suppose there could be one out there that I have missed.
The preponderance of the evidence is pretty strongly in favor of the vaccinated population experiencing lower mortality than the unvaccinated population.
And yet, this is the "science" that was used to push the vaccines on the entire population. It just so happens that the group with the larger number of deaths was the vaccinated group, but we aren't allowed to talk about that. A question: why was this not discussed?
> And yet, this is the "science" that was used to push the vaccines on the entire population.
Yes. It's sound science. What problem do you have?
> It just so happens that the group with the larger number of deaths was the vaccinated group, but we aren't allowed to talk about that. A question: why was this not discussed?
It wasn't discussed because 17 vs 21 in a sample size of 40K is not a statistically significant difference. I don't know how to make that more clear without going into a lesson in high school-level statistics.
So, really, it was discussed, as indicated since you and they heard of the discussion. It is indeed quite simple to discuss even, since the conversation should end with learning that this is covered in high-school stats class.
What is more ironic to me is that this is the total deaths number, without any regards to cause. And in a large population of 40k healthy individuals, is is expected for a few to unexpectedly die over 6 months. This is ironic, since skeptics also often seem to claim that 10-50% excess all-causes death in the population was just random noise.
Lack of statistical significance does not mean you get to assume the outcome you want, it means you can't say for sure if the effect exists or not. Therefore if you see more people who take the vaccine die than those who didn't, you need more data. End of story.
This should be obvious, indeed, obvious from high school statistics classes. If the effect does in fact exist and you roll out the vaccine on a global scale, you will end up creating a truly enormous number of deaths that should have never happened. Therefore you must be sure that the number of deaths will reduce. Their data couldn't prove this so it should never have been approved. But of course the whole thing was on rails from the start. The idea that governments would have rejected the vaccine trials when they were telling people vaccines were the only way out of lockdowns and buying up millions of doses before the trials even completed, is naive in the extreme.
The core problem for COVID vaccines is of course that COVID just isn't very deadly and many of the so-called COVID deaths were in people dying anyway of other reasons where the cause of death was spuriously mis-assigned, i.e. not people who will join trials. That's why they struggled to show any impact on death.
"To examine the possible non-specific effects (NSEs) of the novel COVID-19 vaccines, we reviewed the randomised control trials (RCTs) of mRNA and adenovirus-vector COVID-19 vaccines ... For overall mortality, with 74,193 participants and 61 deaths (mRNA:31; placebo:30), the relative risk (RR) for the two mRNA vaccines compared with placebo was 1.03 (95% CI=0.63-1.71)"
Excess deaths in the UK. Useful because (a) it's all in English and (b) the UK authorities do split out deaths by vaccine status unlike most places:
"For 14 of the past 15 weeks, England and Wales have averaged around 1,000 extra deaths each week, none of which are due to Covid. If the current trajectory continues, the number of non-Covid excess deaths will soon outstrip deaths from the virus this year – and be even more deadly than the omicron wave. The Government has admitted that the majority of the excess deaths appear to be from circulatory issues and diabetes – long-term, chronic conditions that can be fatal without adequate care."
UK data at first appears to show that the unvaccinated die at a higher rate. However, this is only because they're using incorrect population figures. Although it may seem absurd the government population figures in the UK are officially labelled "experimental" because they are universally acknowledged to be far too low. In some age groups the official population is lower than the number of people who came forward for immunization, so these figures cannot be used and indeed the UK HSA didn't use the official population stats when computing their own effectiveness rates, but rather estimates from NIMS (National Immunization Service). If the same methodology is used then you can calculate chart 4 on this page from officially released data:
"The ONS data is interesting because it also includes data on non-Covid deaths by vaccination status ... Using this alternative estimate of the population of England [from NIMS] now suggests that the vaccines substantially increase the risk of death for reasons other than Covid."
Unfortunately and worryingly, even the NIMS estimates are likely to be seriously off. According to NIMS about 9% of the British population refused vaccination but a few months ago the BBC commissioned a professional survey from a polling firm, to ask people questions about their vaccine status and if they didn't take it, why not. They were surprised to discover that 25% of people said they were unvaccinated.
> To examine the possible non-specific effects (NSEs) of the novel COVID-19 vaccines, we reviewed the randomised control trials (RCTs) of mRNA and adenovirus-vector COVID-19 vaccines
Did you bother to click on that first link? It's broken because the authors retracted the paper. This kind of stuff is the reason it's hard to take vaccine skeptics seriously.
Yes, that's how I quoted from it. The link had a number deleted from the end, a mistake whilst editing the post. I fixed it. The authors haven't retracted the paper.
> For overall mortality, with 74,193 participants and 61 deaths (mRNA:31; placebo:30)
31 deaths with mRNA and 30 deaths with placebo with over 74K people in the trial to me means that mRNA carries zero risk. In a sample size that large, 1 additional death means essentially zero correlation.
"This article is very painfully committing the Base Rate Fallacy."
You didn't read past the first sentence, did you? Embarrassing, because the article starts by explaining the base rate fallacy and pointing out that the social media meme it starts by highlighting is wrong. Then it goes on to do correct analysis, which shows the conclusions I gave. You'd have known this if you read my post properly too, because I have a whole paragraph about the stats involved in correctly calculating base rates. If you think there are mistakes in the rest of the article please explain them, but you do need to actually read it first.
"I'm not going to accept "Daily Sceptic" as a source."
Again you didn't even click the link and look, did you? The image is a table of data from official government statistics, they simply happen to host the screenshot. But I knew I'd get a response like that from someone. Lack of intellectual curiosity around this topic is extreme - for obvious and understandable reasons of course. But still.
Re: PowerBI
Where do you see that? There are virtually no COVID deaths (a.k.a. "had a positive test a month before death") since the end of the winter in the UK. Look at the data for the various kinds of heart failure, for example. You see clear excess where COVID isn't implicated starting around the end of April.
"1 additional death means essentially zero correlation."
After incorrectly snarking about not understanding statistics, you're now demonstrating a mis-understanding yourself (albeit a very common one).
You can't simply look at a small difference and say "not statistically significant therefore there is no risk". That's not how statistics works. Firstly, the overall sample size was very large, it was an RCT. So we can say with great certainty that the vaccines have no effect on mortality, yet, that was the entire purpose of developing them. I see up thread some people are now trying to deny this, claiming that the vaccine trials were never meant to even study death rates! Truly Orwellian stuff. Death is the endpoint that motivated everything.
What we can't say with great certainty is if the vaccines are truly more deadly than the placebo. But statistical significance is not the same thing as significance. This is a really common logic error you see even amongst scientists themselves (when badly motivated). This result means the vaccines might be more deadly than the placebo or might not, and therefore the correct response is to gather more data. The incorrect answer is to say "eh, yolo, let's assume the optimistic result", especially if you're about to force people to take it on a massive scale.
But of course they didn't gather this data. The people who created and run the COVID vaccine programmes think that any expression of doubt about vaccine safety is immoral anti-science anti-vaxx insanity, which in turn means they can't neutrally measure or act on data. Their conclusions are chosen before they even do a single experiment, so they just went ahead and did it.
At any rate, the placebo in these trials was incorrect. They gave the placebo arm vaccines too, just different ones, so this is actually not comparing against reality (=no vaccine) and therefore overly generous to the vaccine under test.
As you see in the article, this is a mathematical model which indicates vaccines saved 20,000,000 lives. It is completely unprovable and only serves as a nice sounding talking point.
I also could claim 20,000,000 lives were saved by natural immunity. Or vitamin D from sunshine. Or the placebo effect.
Prove it then... not even the 20 million but just a single death saved because of the vaccine. You cannot. It's not a rip on you, nobody can. Hence it's not provable.
If anyone could, they would have already and wouldn't have to resort to nonsense theoretical computer models.
VERY interested in your attempt though gets out popcorn
Really, you think that?
There are excess deaths and dropping fertility. What is the cause? People have tried every explanation they can think of and nothing adds up except for one thing few people want to talk or think about, why is that?
We’re not talking about speculation, we’re talking about clear thinking and rigorous deduction of potential causal pathways. The drop in fertility is, horribly so, blindingly obvious. In country after country, 9 months after mRNA injections rollout for young people we are seeing a striking drop in births. We know there is an effect on women’s reproductive system and men’s. Men’s sperm counts drop a study from Israel has shown. Many, many reports from women of their periods having been effected.
Unfortunately, there is nothing speculative about this. Nobody wants this to be the case. That this was pushed the way it was on young people is criminal and insane.
In terms of death or injury there are definitely cases where it is entirely clear cut just hours or days after an injection somebody is dead or severely debilitated in a way clearly linked to the shot.
Those are deaths or injuries that had no business occurring and yet they did, why?
In the aggregate/macro overview we’re seeing it in data where it can’t be hidden and in the day to day. Just do a search for something like “unexpectedly died”
Again, who wants this thing so many went fanatical about a year ago to have caused this?
Something did cause it though, and at this point the most likely and parsimonious explanation is the shots. And not for lack of trying alternative explanations. Why stick your head in the sand if that leads to more death and destruction. We’ve found ourselves in a hole in terms of societal health, let’s stop digging.
This is the first I’ve heard of the invisible space alien theory. What is the evidence for it?
> The drop in fertility is, horribly so, blindingly obvious. In country after country, 9 months after mRNA injections rollout for young people we are seeing a striking drop in births.
The US birth rate continues to climb after the introduction of vaccines, for the first time in decades.
I have yet to see a chart that shows a decline that wasn’t painfully manipulate to hide the fact it declined much less after vaccinations than it had in the decade leading up to it. Though I have only seen articles for a handful of countries.
Common internet debate confirmation bias to grab the first thing you think supports your point after a quick scan, link to it like it is a slam dunk, and read no further.
You sounded like you were genuinely interested in learning more, saying you hadn’t seen most of the data so I posted some links to get you started. There is a lot more there than the link you posted.
I don’t think Chudov would say “unfounded,” even if it is temporary that is still a scandal almost beyond words.
“Take this shot you don’t need, that we’ve either
terrorized or coerced you into taking and it may permanently or temporarily impinge on your ability to reproduce or cause a host of other maladies “
No part of that is acceptable.
And even if it is temporary after one shot, how temporary is it going to be if the shots continue to be pushed and mandated, and each additional shot increases the effect?
The University of California system has just announced they are mandating yet another shot!
It is madness and criminal.
Ok, I should have read further and posted a full reply. I had seen his data before, and it looked a bit scary, so I am interested, but I also quickly noticed that it lacked statistical error bars and was excluding any data that contradicted his hypothesis.
Would it change your perspective if you learned that the still birth rate in 2022 was still lower than every previous year, except for the years 2019 and 2020 that he uses as comparison?
Does it change your perspective if you learned that the birth rate has been dropping about 2-3% per year, except for the year in comparison (2021) when it was 2% higher than the previous year?
Does it change your perspective if you learned that vaccinated mothers appear to have been slightly more likely to have a healthy, normal birth over this same time period (fig 3-9), though the difference was not statistically large?
All of these links are directly from his blog post, so I know he also had access to this data, which shows it was safe and even beneficial to you to get vaccinated, and he apparently chose to ignore it.
> even if it is temporary after one shot
If it doesn't reoccur though, it is temporary, regardless of what else happens. But the data would already have included the effect of boosters by now. In some ways, the blog post also suffers from a lesser known problem of being too-big of an effect. It was >8% decrease when <20% of the population had a vaccine, so now that >60% has had a vaccine, we should see a >25% drop in births. That is too big an estimated effect he's observing in one specific area for it to be invisible to other statistical measures and countries. So that hints something else is wrong with his analysis, failing to account for something, or taking small numbers as divisors to make them look bigger.
I had heard a fun podcast on excess effect size being a possible yellow-flag for statistics, but cannot locate the exact one for you. If I recall right though, it was related to Andreas Glöckner's discussion of the size of the mental depletion effect linked from
https://freakonomics.com/podcast/in-a-job-interview-how-much.... In that article he shows how the correlation was too strong between "mental depletion" and outcome, that it likely points to there not being a causal-link.
I didn't know I was going to look more, but I decided to look at his Hungary data. He mentions in conclusion that his R^2 of 0.22 is "relatively low", but does not seem to understand that is means his theory fails to explain more than 75% of the variation between counties. And thus his result is that he is highly confident (97%) that less than 25% of the difference might be correlated to vaccinations.
Thus, to come back to belltaco's point, his post shows there is far more evidence for invisible space aliens (75% unexplained correlation) who only target Hungarians than for vaccines (25% possible correlation).
Over a million people, in the U.S. alone, died in under two years after being infected with this virus.
Even granting the unlikely possibility that this mouse model is reflective of the immune response in humans, whatever other microorganisms people were encountering were demonstrably less dangerous than SARS-CoV-2.
Unless you know of some other highly infectious microorganism that rapidly spread to hundreds of millions of people and killed 1-2% of those it infected?
> Even granting the genuinely unlikely possibility that this mouse model is reflective of the immune response in humans, whatever other microorganisms people were encountering were demonstrably less dangerous than SARS-CoV-2.
The mouse model is apparently enough for the new booster.
So they ran the phase 2/3 trial in >1000 humans for fun?
The problem with anti-vaxxers is you just imagine a world in which everything is underhanded and a conspiracy when all the science and data is out there in the open, just ignored.
Anti-vax? You have no clue what my beliefs are on this, I'm not anti-vaccine. I remember just last year the Biden administration forced through the booster shots (after a propaganda campaign predicated one & done, that then extended into mandates, which Biden, Pelosi & others said were never on the table or illegal, later to be proven unconstitutional by the supreme court).
Senior officials at the FDA resigned over the insufficient evidence of efficacy. Not only was it unclear that they should be approved for seniors, they just opened it up to everyone. It's only gotten worse now. It's not even remotely clear to me that the average healthy person (not on the standard American diet, chronically ill with the typical stuff like diabetes & obesity) needs upwards of 4 vaccines, and counting, for a virus that's much more attenuated & practically everyone has some form of immunity at this point.
Also: to answer your question, from what I can tell the studies haven't shown efficacy. They only show that antibodies rose, which we know isn't absolute proof of efficacy with regards to infection or disease.
I never said the trials showed efficacy, though there are multiple high quality trials which do show serious benefits of 3rd/4th shots in various age groups. I just say they ran human trials, which your comment implied they didn’t.
Also:
- no good evidence the virus is attenuated (lower hospitalizations/mortality likely driven by increased population immunity)
- a lot of FDA/CDC officials agreed with the decision too, and I think on the whole were proved right to offer to the booster to older populations before all the studies were completed.
- nobody is forcing you to get the 3rd/4th shots, why do you want to prevent other people from getting them if they want them? You are sooo sure they are bad?
Sure let people get them voluntarily. My point is that all this irrational exuberance is very clearly precipitously eroding trust in public health authority & science generally.
> My point is that all this irrational exuberance is very clearly precipitously eroding trust in public health authority & science generally.
Nobody needs vaccines for this. We have actual evidence of doctors who got kickbacks for giving patients addictive drugs they didn't need, of pharmaceutical companies lying about known risks, of scientific papers that are nonsense being published, of the CDC lying to the public because they didn't trust us to act like adults and not stockpile masks. There is a US doctor telling her patients that their illnesses are caused by alien DNA and demon sperm, and she's still allowed to keep her medical license. These are hurting trust in science and public health.
I don't blame people for being skeptical of what's going on, but far too often what people are doing is just putting their trust into whatever backs up what they've already decided must be true. People who thought the vaccines were bad before they had any evidence at all to support that have total faith in every study and doctor they can find which might support their position while insisting that the mountain of evidence that contradicts them is a lie cooked up by a conspiracy.
Everyone should be distrustful of research papers, doctors, and public health agencies right now. They earned that, but that just makes it more important that people do a better job of avoiding their own biases and evaluating the imperfect information we have. For all the problems that exist in science, when the vast majority of scientists are telling us something it's best that we listen. We should be most cautious when listening to people who are telling us what we want to hear.
If you're going to unveil a new vaccine it should be proven to be effective. Anything else at this point (when practically everyone has developed an immune response through infection or previous vaccination) is unethical.
The mouse models were challenge studies, i.e. how do vaccinated mice respond to exposure to the omicron variant? That's what matters. Versus what you are demagoguing. Conflating with "tested", that since the new booster was given to humans and no abnormal AEs were observed & antibody levels rose, that automatically means it must be effective.
This is precisely the scenario that degrades public trust in institutions when this fast-and-loose science is being rolled-out live on large populations.
However this exact issue you are talking about was debated at the public FDA hearing on whether or not to approve the updated boosters. Most, but not all, of the people on the committee believed that it was worth the risk with incomplete information.
It isn’t ethical or possible to run the studies you want given the existing prevalence in the virus, so you do the best you can. It isn’t fast-and-loose to make decisions with imperfect data when all you have is imperfect data.
Also there were even more interesting and nuanced arguments against the updated booster but evidently you didn’t read the FDA meeting notes and see the arguments from the couple people who voted against it. Oh well.
> Most, but not all, of the people on the committee believed that it was worth the risk with incomplete information
This is hardly surprising considering two of the people most likely to disagree resigned from the FDA after the last booster approval, due to their disagreement with the process. [0]
The people who resigned were FDA Office of Vaccines Research and Review Director Marion Gruber, Ph.D. and Deputy Director Phillip Krause, M.D.
After resigning, they also published a critique in the Lancet of the policy of boosters for everyone. [1]
What? I’m not arguing a decision a year ago. I’m arguing it’s unsurprising there was no disagreement the second time they asked everyone if they want to approve the boosters, since the people who said “no” the first time are the same people who resigned in protest when nobody listened to them.
and the reasons why it should be clear to you are what, precisely?
Do you have some particular expertise in public health? Or are just another person who believes that applying their own intelligence and internet sleuthing skills are sufficient to allow them to question the decisions made by people who make this sort of thing their life's work?
Science requires participation to work. If these “experts” cannot explain their data and people can’t reproduce their results… something is badly wrong.
Neither "experts" nor anybody else have any obligation to convince every skeptic of their position, even if it is preferable for them to explain the data they get from reproducable studies.
I'm sure the Army would love to have the draft and would make it their life's work to get every American to be all they can be. Every American has to sleuth their way through the rat race or you will be taken for a sucker.
It doesn’t require a conspiracy to think something is majorly wrong with how the last 2.5 years were handled. Everybody played to their incentives and thought they were doing the right thing. The outcome was a complete disaster and a horrific overreaction. But people thought they were doing the right thing.
It’s kind of like a modern engineering failure. It takes multiple failures to bring down complex, redundant systems. That is what happened here.
> when all the science and data is out there in the open, just ignored.
I lost count of the number of times somebody yelled or called me “dangerous” for showing this data. Most of the public data goes directly against the narrative people like to push. It gets tossed right into the “conspiracy” bin. Virtually nothing about our response was based on science or data.
> Virtually nothing about our response was based on science or data.
Virtually nothing?
So the thousands and thousands of studies on vaccines, treatments, mask policies, vaccine policies, school policies, air filtration techniques, etc, etc… those were just done for no reason?
To say we live in an imperfect society with imperfect leaders and imperfect citizens is a fair point. Incorrect decisions were and continue to be made for political reasons or religious reasons or whatever else. That’s what happens in an imperfect society. To say “virtually nothing” about the response is based on data is just ridiculous.
Again, anti-vaxxers and conspiracy theorists make up a world where decisions are made in secret for suspicious reasons when generally all the data and arguments are out in the open and are just ignored.
Are all the highly esteemed professors, scientists, politicians, healthcare workers, and researchers who signed the great barrington declaration anti-vaxx conspiracy theorists?
Do you have any idea how many people in real life yelled at me and called me incredibly nasty things for suggesting that maybe, just maybe this myopic fixation on Covid was going to have some serious long term effects and maybe, just maybe we are overreacting?
You can’t speak against the narrative. Speaking out against what we did was and still is career suicide if you are in healthcare, science or research.
There has been a continual incredibly strong push to label anything that goes against “the narrative” as misinformation, “anti-whatever”. Speaking out as a member of the medical/science community gets you blacklisted. Beware of any research that got published in the heat of this mess—there were strong incentives to only publish research that supported “the narrative”.
There is a huge difference between saying we made a lot of mistakes in the response to covid and saying “virtually nothing” was based on data.
I don’t support people being shut down as you talk about, however you should also appreciate that a ton of people speaking out against the “narrative” were just grifters spreading misinformation for whatever random reason. A lot of the blame for legitimate dissent being ignored is due to the fact that most dissenting views were actively in bad faith.
Why not plural microorganismS?
Although a neglible increase of mortality across countless events where broad-acting immunity protects us may be outside your ability to calculate, it's still readily applicable to recognize that a lot of straw exists on a camel's back without simply studying just the one which broke it. An overall increase in mortality from all causes is congruent with valid scientific theory and is a hypothesis worth evaluating without eschewing existing data.
Your question is unneccessarily leading with false premises by which you define the answer without accepting the known truth.
If you're looking for just one organism which would need to spread, then you're looking in the wrong place for how, i.e., people were killed by myocarditis, or inability to stay nourished while suffering vaccine-induced side effects, including inability to defend with the same metabolic fervor from the flu.
As another commented pointed out, we have hundreds of millions of data points in people now post-vaccination and post-boosters, which haven’t detected a problem, and only 12 here in mice, that the authors suggest warrants further study. Which hypothesis are you saying has “no data”?
It is hard to see a problem if you are not looking for it or if the cause is distant from the reaction.
An Example: My friend had undiagnosed alpha gal for months because the anaphylactic reaction happened to him more than 12 hours after eating red meat so they did not know the connection.
Is Long Covid actually not from COVID but from this weekend immune system having to fight off old latent viruses it once had not problem with?
You’d be amazed at the number of unexpected effects I could find studying just a single mouse!
Having a small number data points means that a single outlier can impact your results. And since “no results” typically doesn’t get published, the rare events end up disproportionately represented in journals.
The smaller the sample size, the more likely the “effect” you’re seeing is just random chance.
You're welcome to post the other pandemics that occurred in 2020 through 2022.
Flu was practically wiped out for example. COVID19 was more fit, and many people were taking precautions (ie: masks) that also hampered the spread of Flu.
If mRNA vaccines really inhibited general immune response to other viruses / bacteria, it should be demonstrable. Just line up the number of people who died / got sick of non-COVID19 diseases in 2020 through 2022 and compare them to the COVID19 vaccine patients, stratified for age/sex/race.
Okay. Take any COVID-19 test kit and see if someone sick with the flu tests positive with them.
There is a simple thing called science. COVID-19 test kits are literally free. It wouldn't even be a hard test to do. EDIT: In fact, most COVID19 test kits come with their documentation, showing how well they test vs the Flu (guess what? Most of them don't detect the flu at all)
You should probably investigate how sensitive PCR tests can be. We cranked those things up to 11 so anybody with a spec of the virus got labeled as a Covid case.
Be specific. Because each test kit has documentation on how well it has cross-reactivity to other virus strains. I know its complicated with lots of competition here in the USA and lots of different manufacturers.
So I need to know exactly which test kits you were using, and which virus (Influenza type A? H1N1? Adenovirus? Influenza Type C?)
EDIT: For example, Abbot's test kit has the following documentation: https://www.fda.gov/media/136258/download . We can see page 10 how much it cross-reacts with other viruses: which is not at all.
It doesn’t even matter honestly. The data used to justify all our incredibly costly mitigations is a toxic dumpster fire. You could take that data and twist it to justify anything you wanted.
And even then the actual science and data never mattered from a public policy (or even public health) standpoint. It’s been politics, fear-mongering and straight appeals to authority all the way down.
> You could take that data and twist it to justify anything you wanted.
No. My question is if your side has any data at all on the assertions you're making.
Because in my experience, with regards to this debate, one side seems to just be flaunting falsehoods, while the other side has actually done tests and demonstrated their results.
I'm trying to figure out which side you're on. The side with data, or the side without. If you think the data was poor, fine, whatever. Where's your data that supports your viewpoints? Even if you break someone else's argument, it doesn't matter unless you yourself have data that supports your own side.
It’s not my job to prove masks work, lockdowns work, or vaccines work. That isn’t how science works. You can’t prove shit doesn’t work. The hypothesis is these mitigations work and are worth their respective costs. The burden of proof is on the people making these claims and pushing to enact them.
Outside of vaccines I’ve yet to see any convincing evidence that any of our NPI’s worked in a way that justified their incredible costs on society. The fact that we did them without any understanding of their efficacy is astounding to me.
> It’s not my job to prove masks work, lockdowns work, or vaccines work.
Can you stay on topic? This subthread is about a simple discussion. Do COVID19 tests detect the flu?
The answer is no.
Now if you wish to move your goalposts. Feel free to do so. But don't expect me to condone or accept your obvious fallacy. If you're changing the subject so intensely, I more or less take it as a discussion win in my favor at this point.
I think I've readily proven that your earlier discussion point has no data behind it. And I have no reason to believe you have data behind any of the other discussion points you're bringing up.
EDIT: Now if you start posting some data, maybe I'll start to listen again. But I'm not going to take or respect just wanton assertions in this subthread.
>There is a much simpler explanation which is: people with the flu were testing positive for COVID and health authorities were counting flu cases as COVID.
That is if the authorities were stupid. I can't say for the US but where I live there was no reduction in flu tests and there were still barely any cases found.
If enough people in the population take certain precautions, and those precautions limit the spread of disease, then there is some sweet spot between the virus’ contagiousness and number of people who take precautions that will cause the virus to not spread.
Some people wore masks some of the time, varying by seasonality, weighted regionally by the dominant political ideology of the area. My understanding is that masks were more effective against the flu than covid because Covid can spread in finer particles than the flu, which makes masks more effective in fighting the flu.
> people with the flu were testing positive for COVID and health authorities were counting flu cases as COVID.
We know this happens, the critical missing part of your argument is your estimate of frequency. If your theory were true, the precipitous drop in flu cases indicates that almost everyone with the flu also had Covid. That doesn't pass the smell test to me - I feel confident we would have heard if there were that high a correlation, given all the research going on at the time.
That only makes sense if people were wearing masks to combat the flu before covid started and then Republicans stopped wearing them to spite covid mitigation efforts but that's not the case.
From my understanding the flu is less contagious than covid so any efforts we were taking to stamp out covid that were holding covid in check would have stamped out the flu.
>Just line up the number of people who died / got sick of non-COVID19 diseases in 2020
This is _extremely_ difficult to do, as a mix of both incentive structures and poor policy lead to any death with a positive PCR test being counted as a COVID death.
It's practically impossible now to go back and figure out how many were _actually_ "killed by COVID" vs "died _with_ COVID".
COVID19 doesn't even play a role until 2 or 3 lines later. Doctors write down "Killed by X" which was caused by "Y" which was caused by "Z". COVID19 is never "X", its always Y, Z, or later.
---------
Because we have these statistics, we can correlate "X" causes. If "X" is "blunt force trauma to the head", it is unlikely that "Y" or "Z" will be COVID19.
But don't take my word for it. There's plenty of death certificates, and such data has been coallated together.
See Table 2 in this list, as an example. You can see that the immediate cause of death for most COVID19 patients is Pneumonia, unspecified (J18.9), followed by Acute respiratory failure (J96.0).
Which of these ICD codes do you think is being misclassified as a COVID19 death? Please be specific. Any such large scale misclassification would be obviously in the data here.
You're right. At one point I read it was as high as 10 years that the average person who died of covid could have otherwise lived on for. I suspect that number has changed a few times over the pandemic, but even a few years more years with a loved one is priceless, losing anything close to a decade would be a massive loss.
I’m sure George Floyd would have lived a little longer if he wasn’t Covid positive when he died.
It doesn’t matter anyway. The data required to support our mitigations stopped mattering a long long time ago. ..Sometime back when the “4% kill rate” predicted by the imperial college paper turned out to be very very wrong and when all those temporary military hospital things got closed because they weren’t being used. That might have been a good time to reevaluate what the fuck we were doing but instead of celebrating the fact that Covid wasn’t nearly as bad as predicted we just doubled down for a year and a half more instead.
Honestly it’s best to just take the numbers at face value and assume any overcount is balanced by undercounts.
If 95% of people died from covid, and 5% died with covid, then basically for all intents and purposes and how we use this data, the distinction is irrelevant.
I agree. I just take the numbers at face value. Trying to suggest they are under or over counted is a fools errand. It will take decades of distance from this event for cooler heads to tally up what really happened.
Had those mice been immunized against influenza? That's not what I read, but I might have miss it. What I read is that they used the vector without any payload, and it turned out that influenza is an example of something nominally unrelated where resistance was slightly increased while candida albicans (no idea what that is, not a native speaker) are an example for slightly lessened resistance.
Lines up well with my mental model of how the immune system deals with the unknown: a million monkeys not on typewriters but on text editors with copy/paste. Who fire new code, aimlessly mashed up from their library of previous experience, at a test fixture. Any change to unrelated previous experience can increase or decrease their chance of finding something that sticks.
No, they then followed up with an influenza vaccine delivered by mRNA. This study assessed the relative quality of immune response in those that had previously received a sham vaccine delivered by LNP, or no prior vaccine (or LNP).
> Two weeks later, the mice were injected in the same area with 2.5 μg of mRNA-LNP coding for PR8 influenza hemagglutinin (HA)
Well, the paper quotes unexpected changes in your adaptive immune response. What's observed is a slight decrease of immune response in mice for a highly specific condition. We don't know how the overall immune response changes. For all you know, small decreases in immune response to diseases might bubble up to be a significant decrease.
I agree with you. Also, a problem with the vaccinations is inflammation. A well planned and implemented diet can reduce inflammation. Indeed, my wife and I always tune up our diets to decrease inflammatory foods while eating as many anti-inflammatory foods as possible, and we have been doing this since long before Covid-19.
> It sounds to me as though the tradeoff being made here is: a slightly decreased immune response generally, but a better immune response to the thing you've been immunized against.
No compromise was posited, it is a consequence not a trade off. Not remotely the same
> Also: this is purely in mice. They have zero data on whether this is true for humans.
Out of curiosity, how do you feel about the new bivalent BA4/BA5 booster? It's only been tested on... eight mice [0]:
> So what data specific to the BA.4/BA.5 boosters, did the FDA use to expand the EUAs to include the BA.4/BA.5 boosters? Well, the answer is at least in part very “mice.” Apparently, both Moderna and Pfizer-BioNTech have provided non-human animal data on the BA.4/BA.5 boosters to the FDA to state their case for the EUA. But they haven’t yet shown this data to the rest of the scientific community or the public. This data have reportedly included some preliminary findings from eight mice.
Hey, if that's good enough for emergency use authorization, why aren't the findings in this paper up to snuff?
It's highly unlikely the booster trials were on eight mice.
edit: Found the source of the eight mouse thing; it's a misreading of https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-..., page 21. It's not the safety trial, it's the immunogenicity comparison on a small population of older mice previously given the primary vaccine. (The previous slide, #20, has a heading of "Pre-Clinical Studies"; #21 is describing the early studies before the human trials.)
Page six debunks the idea it's only been tested on mice entirely; it cites a trial of 512 human adults for the Moderna BA.4/BA.5 Omicron booster.
A month is more than enough to demonstrate safety; vaccine reactions to the original shot (and in general) were all rapid.
As that article notes, flu shots have a similar regulatory regime:
> And some scientists say health officials know enough about how vaccines work to start handling the COVID-19 vaccines like the flu vaccines, which are changed every year to try to match whatever strains are likely to be circulating but aren't routinely tested again every year.
and that the new vaccine still expresses the original proteins the already-approved vaccinations were expressing; in the worst-case scenario that mice and humans react similarly to Alpha/Delta but wildly differently to Omicron/BA.4/BA.5, we're still likely generating the at least the original immune response:
> The new booster will be identical to the original vaccines except it will contain genetic coding for two versions of the protein the virus uses to infect cells — the protein from the original vaccine and proteins from the BA.4 and BA.5 omicron subvariants.
A rapid approval process is going to be important for boosters, for the same reasons it is in flu shots. It's very clear the claim that it was only tested on eight mice is false.
This is because the ba.4/ba.5 vaccine is so incredibly close to the ba.1 bivalent vaccine, which did see more human trials and showed a similar safety profile as the original vaccine.
Kinda like how we get a new flu vaccine every year that doesn't go through a years long clinical study
Sounds like conjecture to me. But that’s fine, I understand the argument for printing new mRNA vaccines. But please don’t force me to take it to keep my job or travel internationally, and don’t call me an anti-vaxxer for refusing to inject myself with an experimental vaccine that’s been tested in eight mice and a small group of humans for two weeks.
I'm not saying you have to get it. I'd like everyone to get the vaccine, because it is showing greatly improved outcomes over pre vaccine COVID.
You are anti this vaccine, and your posture is largely fear based rather than scientifically consistent given your not-an-anti-vaxxer self probably gets every year
No; vaccines continue to be monitored. We still keep track of safety events on vaccines that have been around for decades.
Many years of experience with vaccination gives us useful info on how bodies react to them, which allows us to approve vaccines based on logical criteria.
You're (intentionally?) missing the point, which is that long-term effects could not have been sufficiently monitored at the time they were thrust upon the general population.
It is possible to believe the vaccines are safe, and to support their use, while still conceding this point.
> which is that long-term effects could not have been sufficiently monitored at the time they were thrust upon the general population
Sure, that'd require a time machine. Thus, we're left going "hey, what happened with every other vaccination we've ever done?" and making decisions based on that wealth of information.
People attempting to make this point like to pretend the same isn't true for not getting the vaccine. What's the long-term effect of unvaccinated people getting COVID? Do we have a 20 year safety study on going unvaccinated in this pandemic?
>Thus, we're left going "hey, what happened with every other vaccination we've ever done?" and making decisions based on that wealth of information.
Now you're being disingenuous. There is another approach, and it is the one traditionally endorsed by the medical profession: prudence.
Put plainly: the deontologically correct way of proceeding would have been to say "we don't know enough to assert the vaccines are safe", and not thrust them onto an unwilling public.
>Do we have a 20 year safety study on going unvaccinated in this pandemic?
No. This is why I am not arguing against vaccines. I am arguing against mandates.
Well they have tested bivalent COVID-19 vaccines in large human trials. These boosters are functionally the same they just target different strains of COVID. I'm not an expert, but that's how flu vaccines are done. They don't have to seek re-approval for every new strain every season, and that seems fine. Maybe that's a bad practice. I don't know, but I'm comfortable deferring to experts in the field on it.
What are you talking about? It's right there in the Forbes article. Did you bother to read it?
> "Well, theory is one thing. Concrete scientific evidence is another. The FDA announcement did mention studies that compared the use of bivalent boosters and monovalent boosters that included approximately 600 and 800 individuals 18 years of age and older for the Moderna ones and 600 participants greater than 55 years of age for the Pfizer-BioNTech ones. These studies reportedly found those who gotten the bivalent boosters had “better” immune response than those who had of those who had received the monovalent boosters. The studies also didn’t show any significant safety concerns with the bivalent boosters, mentioning the usual side effect stuff like pain, redness and swelling at the injection site, fatigue, headache, muscle pain, joint pain, chills, swelling of the lymph nodes in the same arm of the injection, nausea, vomiting, and fever."
Or maybe I wasn't clear in what I said. They have tested bivalent vaccines. Just not for the specific strain of COVID mentioned. I'm saying that seems fine to me since that's what they do for flu, but I'm not an expert. Maybe COVID is different in some fundamental way that means we need to retest for every strain.
Last time I've posted something about mRNA on Hackernews, it reached page 1 in about 2h and then got flagged immediately. HN is not a good place for mRNA discussions.
Yes! Exactly this behavior. There seems to be some hidden rules, what is allowed and what isn't. Very sad. This is suppressing good discussion and forming of own opinions.
It's not some hidden rule, it's just a story that gets flagged by a lot of people. And I can understand that. This discussion is boring and predictable. We've been talking in circles for almost two years.
To be clear, it wasn't flagged by the people. It got flagged and removed by a mod, after it hit the front page. And how do you know about the story, when you couldn't read what I've submitted?
How do you know it got flagged by a mod? Users with 500+ karma can flag posts, and if enough of them do that, then it automatically drops off the page. No moderator action is required.
Maybe you're right and it was "down flagged". It's just because it was so quickly flagged, it could barely last 2 minutes on the front page. In contrast it was constantly upvoted before from other users, before it reached the front page. Why reached it the front page then, just to be immediately flagged?
I'm being sarcastic but I don't think downvoting because of "source" is a good habit for HNers to have - there are far more diverse views and interesting points being made outside of the mainstream narrative, and if the goal is to have discussion with an intelligent community, "source" is a pretty weak reason to not have that discussion.
>LNP alone led to long-term inhibition of the adaptive immune response
So it's the lipid capsule, not mRNA, that has an unknown effect on the immune system. Make sense as many pathogens have lipid proteins on their surface.
> the resistance of mice to heterologous infections with influenza virus increased while resistance to Candida albicans decreased.
Better in some, worse in others
>mice pre-exposed to the mRNA-LNP platform can pass down the acquired immune traits to their offspring, providing better protection against influenza.
> So it's the lipid capsule, not mRNA, that has an unknown effect on the immune system. Make sense as many pathogens have lipid proteins on their surface.
They were too toxic to use as a delivery mechanism as recently as 2018. IIRC it somehow damaged cell walls. Around 2018/2019 there was some sort of breakthrough that eliminated most of the problem, but the article I read last year didn't even try to call them perfectly safe, just safe enough as far as we could tell.
I think this was also the main reason that even though mRNA was being researched for decades, using it in a vaccine was a no-go until recently: We didn't have a working delivery mechanism.
I suppose. Obviously if these findings hold for humans we could all be impacted.
I just think it's important to differentiate what is caused by the nanoparticle delivery mechanism and what is caused by the mRNA. For example it's not super clear (based on a quick scan) which part they are talking about with the notes on heritability.
You can get dysautonomia from either the covid virus or the covid vaccine. The vast majority of people don't yet know what dysautonomia is let alone how to diagnose it or treat it. And from my experience most doctors as well. It's easily observed and the fact that doctors and medical researchers can't get that right diminishes my trust for them being able to get less easily observed phenomena right as well. Everyone should learn about dysautonomia as we're entering an epidemic of it and we're all going to encounter it one way or another over the next few years.
Unfortunately this seems to be a "catch-all" desperation-diagnosis with a huge range of mental and physical symptoms. Diagnostic procedures for it seem to range between esoteric over so very specific, that it would be extremely hard to find a doctor who does them to plain dangerous (lumbar puncture).
How do you propose private individuals that suspect they suffer from it and GPs deal with it?
Very serious, it’s a core component to long covid. It’s a lifetime affliction for the majority who get it (up to 10% of the general population of which less than 50% will go into remission without treatment). People who get it often lose their jobs, their health, and their relationships all while being gaslit by doctors. It is a thoroughly life destroying condition. Suicides are very common. It can be treated but not very effectively for most people. This has been known since the beginning of medicine but the modern (mis)understanding of it is 75 years old (ME/CFS). Before that it was known as neurasthenia and has had lots of names throughout history. Lots of viruses cause it; EBV is the main one. Society will manage ok, people die and others move on, but an already bad problem is going to be made substantially worse, and we’ll all be poorer for it.
As for many mystery syndromes with broad symptoms it's easily connected to covid infection, long covid and the covid vaccines. A clear and satisfying picture seems to be missing, hence me naming it mystery syndrome.
Many of the mystery syndromes are different manifestations of the same condition for which dysautonomia is most often a core underlying part.
By way of analogy; hEDS is clearly autosomal dominant genetic condition and has been known about since Hippocrates yet because it presents in slightly different ways it largely escapes diagnosis. hEDS is also not rare, it’s only considered rare because it’s rarely diagnosed. The fact that medical researchers and doctors can’t get something so simple right after so long means I don’t trust them with anything that is even slightly complex.
It’s hard to say as it’s very hard to collect data on. Lots of viruses can cause it but covid is especially bad for it, worse than EBV which was the main trigger before covid. The mRNA covid vaccine is the only vaccine that I know of that can trigger it.
You have a high level of certainty. what drives it if it's hard to collect data on?
Why do you know the mRNA covid vaccine can trigger it?
Both BioNTech and Moderna's trigger it equally? Do mRNA technologies against other antigens trigger it?
Anything on the penetrance of the disease as a percentage of vaccinated people?
Suggesting that EBV is a trigger requires a very robust analysis as it is nearly 100% prevalent virus in adults. The study that linked EBV and MS was an unprecedented tour de force
I do not mean to interrogate, but I'm fascinated and looking for details or sources so I can better understand.
I have a ML/Data Science background. It's hard to collect data on because doctors are bad at diagnosing and are highly inconsistent. Additionally there is political pressure to skew the data as well as social pressure to suppress data. We know because many people have gotten sick from the mRNA covid vaccine, myself included. In these groups there are sensible people who will tell you privately and with no ulterior motives that they can trace down the onset of symptoms to shortly after the vaccine. It's strongly and reasonably suspected to do with the spike protein and the ACE-2 AAbs created by the immune system in response. This protein is the same in mRNA viruses as in the covid virus. We know EBV is a trigger again due to timing of onset of symptoms, most people are doomed to catch it but usually only catch it once. It's not like MS where there is a long delay before onset of symptoms that would muddy the waters. There is plenty of literature around this point.
> In these groups there are sensible people who will tell you privately and with no ulterior motives that they can trace down the onset of symptoms to shortly after the vaccine.
To argue the inverse you'd have to suggest that a substantially large number of people who do not know each other are lying in the exact same way. Such a conspiracy would be highly improbable. These are not partisan hacks or virtue signalers, they are everyday people providing their first hand account in a private manner in the hope that a treatment can be found for their own benefit and that of others.
There is a spectrum of quality to evidence and the quantity of anecdotal evidence is a quality of its own. Especially when steps can be made to distill and enrich the data.
By anecdotal evidence I mean that “providing their first hand account in a private manner” seems to be your personal experience (otherwise it would be either not private or not first-hand), and I assume that not a large number of people confide to you privately in that way.
To put in another way, the claims you put forward here only amount to hearsay. It’s not clear how you think one should take those claims seriously.
yes
on one hand, "a substantially large number of people who do not know each other are lying in the exact same way. Such a conspiracy would be highly improbable."
and yet: "doctors are bad at diagnosing and are highly inconsistent. Additionally there is political pressure to skew the data as well as social pressure to suppress data" to me this seems like a highly improbably conspiracy without evidence to support.
The linkage of covid vaccines ti this phenomenon relies entirely on two 'conspiracy' like trains of logic. From what I can tell this disorder is complex, and the diagnosis is likely difficult. linkage to EBV is an endeavor. EBV and CoV2 have very little in common. As far as I know EBV has no link to ACE-2 antibodies is stated as the driver for COVID vaccine linked disesae. The link to EBV sounds at a best tenuous as the 'timing of infection' of a virus that is in >95% of people is very difficult to study. A quick search process studies that link to many other conditions and vaccines (HPV, DTAP, others) which are not mRNA vaccines and not corona viruses, and have no obvious linkage to ACE-2 Abs.
There very well may be something here, but rigorous logic is the way to find it, especially in a world where "Nothing is true and everything is possible" due to the proliferation of misinformation.
We actually don't need to run these experiments in mice anymore, we should have adequate data from the real-time studies in humans with multiple doses for 2 years now
/r/science is notorious for their stringent moderation. I went on unddit.com to see what was removed and it was mostly comments with only anecdotal evidence, which is not allowed on /r/science.
There is a very common elitist sentiment here that HN good; reddit bad. Certain subreddits like /r/Science have VERY strict moderation that lead to a high quality discussion and community. /r/Science is a much better place to have this discussion than somewhere else where "I saw the vaccine is bad on Substack" comments get voted to the top.
I'm actually a long time redditor and used to agree with you. However it has actually become entirely impossible to have conversations on reddit at this point even in the non-standard niche subreddits and the random banning by admin has become insane.
Reddit : Digg :: <waiting> : Reddit
Reddit used to be a place where you could discuss things candidly. It feels like a form of high tea nowadays. It's boring and bland and full of increasingly bizarre litmus tests leading to bans.
I don't really care whether HN is better or not. What I'm saying is that Reddit is not even anywhere in my list of places to have discussions. I wouldn't even bother add "reddit" to a google search anymore.
> Oh joy, another paper for the antivaxxers to misinterpret. Some red flags though.
> The tone of this paper, particularly the last sentence ("potentially harmful effects") seems suspect...almost as if they were intentionally riling up the anti-vax crowd.
> They appear to have misinterpreted the outcome of this study, claiming "higher risk of infection than unvaccinated individuals 9 months post-vaccination". The study makes no such claim that I can find. The tables in the supplement show the only subcohorts with a slightly higher incidence rate for vaccinated individuals at 9 months is age >80 (1.3 per 100,000 person days in vaxxed vs. 1.1 unvaxxed, supplemental table 5) and those requiring in-home care (1.6 vs. 1.5). Also notable is that the only vaccine that shows less effectiveness against infection is the non-MRNA vaccine (supplemental table 6) and that vaccinated individuals in all subcohorts were still substantially protected against hospitalization or death compared to unvaxxed.
> The primary source for the claim that mRNA-LNP is inflammatory is a paper authored by three of the four authors of this paper.
> Also notable is that at least one of the primary authors - the one credited with writing and editing - is a GBD-adjacent, anti-MRNA, HCQ truther (Don’t Look Up” Your Science—Herd Immunity or Herd Mentality? - "The virus fatality rate did not support lockdowns, blanket restrictive measures, and non-selective mass vaccinations. There was no solid scientific rationale to adopt the untested mRNA-LNP platform over other well-established vaccine formulations to fight COVID.").
> None of this means the science in the paper is wrong, but I'd be hesitant to take anything at face value.
Dear reader, please keep in mind that this isn't just about the most political virus of all times, but many other diseases.
mRNA vaccines against many diseases are researched as we speak, including the elusive HIV vaccine, which could lead to the eradication of the most stigmatizing virus in the world.
If all of those required LNP and we find out that LNP are very, very unhealthy, that would be very, very disappointing.
TL;DR > We found that pre-exposure to mRNA-LNPs or LNP alone led to long-term inhibition of the adaptive immune response, which could be overcome using standard adjuvants. On the other hand, we report that after pre-exposure to mRNA-LNPs, the resistance of mice to heterologous infections with influenza virus increased while resistance to Candida albicans decreased.
My layman question: how is this different from exposure to SARS-CoV-2 itself?
Getting SARS-Cov-2 without getting an mRNA shot allows the body to develop durable immunity; how many people do you know who got the shot have gotten SARS-Cov-2 once or more after getting the shots and boosters?
I'm not trying to be controversial but it seems if just get SARS-Cov-2 and survive you're better off than if you didn't get the shots and boosters.
>how many people do you know who got the shot have gotten SARS-Cov-2 once or more after getting the shots and boosters?
I have. Got the first shot in August 2021, then got covid in December 2021. Got the second shot in January 2022 because my new job forced me to get it in order to stay employed, and then I got covid again in August 2022.
> how many people do you know who got the shot have gotten SARS-Cov-2 once or more after getting the shots and boosters?
Me, my wife, her parents, my mom, my grandma, and my brother's entire family.
That said, all of us had very mild systems. For my wife and I, it played out like a cold. A minor fever for one day, a cough for two days, and a runny nose for three. Honestly, if it wasn't for the fact that my wife's work gave everyone 10 at-home COVID tests, we probably would have assumed it was a cold and not tested.
My mom and grandma (who live together) both got COVID about 4 weeks after their second booster. My mom is immune compromised and my grandma is 83 and has poorly managed diabetes. COVID should have been a death sentence to both of them. Instead, they just laid in bed for a couple days and were fine.
The vaccines won't necessarily prevent you from getting it, but they'll greatly reduce the symptoms, hospitalizations, and deaths.
> how many people do you know who got the shot have gotten SARS-Cov-2 once or more after getting the shots and boosters?
Yes, most of them? At least in my area the first peaks of Covid were small, vaccines were available relatively early and most of the people I know were part of the early-vaccinated subpopulation when the big waves hit - so most of people I know got Covid after the vaccination and just a few did before the vaccination. And even less have never gotten it - anecdotally, the people I personally know who "didn't have Covid" are those who didn't test for it when they got sick.
Anecdotally the vaccination status didn't seem to have an impact on the likelihood of catching the disease (e.g. vaccinated kids brought it home from school about just as likely as unvaccinated kids did) but rather on the severity of the disease.
So in my view there is no really a choice of SARS-Cov-2 versus shots+boosters, it's effectively SARS-Cov-2 (likely multiple times as well) versus shots+boosters+SARS-Cov-2.
I know people who got it without the vaccine and have since gotten it multiple times (one up to 4 times!).
Rather than use anecdotes and spread misinformation, we can Google (multiple sources!) and find some studies comparing the outcomes of vaccinated and unvaccinated people.
It has been known for some time that there is slightly weaker long term immunity for 2 shots when compared to getting it without. This gets better 3 shots, and getting 3 shots and having gotten covid is actually the most durable response of all 'options'.
This is silly. Getting two shots was the "most durable" until it wasn't. There's literally no reason to believe that three shots is the holy grail, especially since we're up to four. Or is it five now?
I have had, approximately, 15 flu shots in my life.
Sure, you say, the flu changes constantly.
I think I've had something like 7 or 8 Tdap shots. The vaccine schedule on that is 3 shots two months apart, another shot a year later, then 2-3 years later, then every ~ten years after that.
Why is "You need more than one shot" such a silver bullet argument?
This is antidotal but my wife mother is a anti-vaxxer and has gotten covid at least twice that we know of, once during the initial surge here in the US and now just a few weeks ago.
I know a number of people who got COVID twice before the shots became an option as well. There never was any reason to think COVID would result in durable immunity, but some anti-vaccine have spread that as part of their general war on science. Lets me clear though, it was always propaganda with no basis in science (both anti-vaccine and political propaganda for different reason said things like that), nobody with any knowledge of infectious disease said something like that.
We have no information going back millions of years. Modern science is only a few hundred years old most progress is closer to 50 years. Coronavirus has mostly been a minor cold, and so I'm not aware of any study suggesting durable immunity.
> There never was any reason to think COVID would result in durable immunity
Huh? Where does this come from? Where was the underlying data or mechanism (before the pandemic hit) that getting COVID (unlike most any other virus we've seen) would not result in durable immunity?
The person you asked is probably going to reply with a comment about the frequency of mutations being so high that no two variants are the same and so there would be no immunity between them, in the same way you can get the flu twice.
The problem with this argument is that it applies equally to a vaccine that targets a single variant of the disease (never mind one that isn't even circulating anymore).
This is a good question. It also highlights the danger of a lay-interpretation of these results.
It is certainly already known that exposure to one viral strain can weaken response to others. But this fact has to be taken as part of a body of knowledge on how these effects balance each other to come to any kind of cost-benefit conclusions.
Yes, is was already confirmed in a Swedish study that mRNA from these preparations can be reverse transcribed into DNA [1]. Now this study shows that the reverse transcribed DNA is active as well. The first thing that should be clear is that this was not an intended effect, the mRNA was supposed to be acted upon and discarded. As far as I'm concerned this is not a positive development either since it implies that new cell lines will have been created which can produce SARS2 spike proteins. Long after SARS2 is gone or mutated so that these spike proteins are no longer analogous to the ones on the virus these cell lines will still produce inflammation-causing spike proteins. If those cells happen to be in the wall of a blood vessel, in an ovary or testes they're likely to cause problems. As the study says there is a need for more research to determine this platform's true impact on human health.
These preparations were offered to and in many cases forced upon a large part of the population without knowing what long-term effects they had. This was the largest medical experiment ever conducted and the jury is out on both the efficacy as well as the safety of the preparations.
Explain, please, why? Preferably with some evidence like that study I linked to and the one which started this thread. Explain why:
- it is abject nonsense to state that cell lines will be created which carry DNA originating from mRNA reverse transcription as is shown in the Swedish study
- it is abject nonsense to state that this DNA is expressed as is implied in the study to which this thread is linked
- it is abject nonsense that cells which express DNA to produce spike proteins will be around even when SARS2 has disappeared or mutated so that its version of the spike protein no longer is analogous to the one produced by cells which carry DNA from reverse transcribed mRNA
- it is abject nonsense for such cells to be found outside of the shoulder muscle mass into which the vaccines were meant to be delivered but from where it has been proven they escape into the bloodstream
- it is abject nonsense for such cells to cause inflammatory reactions when it is known the spike protein does just that
If you sit on knowledge we do not have I suggest you share it.
> If you sit on knowledge we do not have I suggest you share it.
There's a reason that Swedish study is unknown outside of antivaxxer circles and it's largely to do with it being scientifically incompetent and published in a journal with zero standards. Best of luck to you in whatever it is you think you're doing though!
That term 'antivaxxer' does not mean what you imply it to mean. Those who are cautious about using largely untested preparations while being open to using well-known vaccines - against Polio, Measles, Diphtheria, Whooping Cough, Tetanus and others - are not 'antivaxxers', they are 'rational individuals'. There is a wide gap between this group and 'traditional antivaxxers' who worry about 5G-transponders in vaccines (etc) so using a term which most people assume to identify the latter to accuse the former is not just erroneous but also disingenuous, just the type of word game which has become so prevalent in the last decade.
Yes, yes, all just a word game. You're just asking intelligent rational questions, unlike those antivaxxers of lore with their bad faith.
Meanwhile the top thread on Reddit discussing that specific article is in the subreddit "NurembergTwo" and titled:
"Shocking study finds covid vaccines REWRITE your DNA… criminal CDC proven to have repeatedly LIED about this very issue to deceive and harm the public"
If you're basing your theory of harm from vaccines on bad articles from non-experts in fringe journals, there might be less distance between you and the 5G nutters than you wish to acknowledge
Do you have anything else to say apart from trying to paint others with your broad brush? I did ask for some constructive arguments after all, not baseless character attacks. As it stands now I can only assume you don't have rational arguments (other than 'my experts are better/more virtuous than your experts' but that is not much of an argument).
> Interestingly, mice pre-exposed to the mRNA-LNP platform can pass down the acquired immune traits to their offspring, providing better protection against influenza.
Who knows what other interesting discoveries will be stumbled upon in the future!
In the future can we agree not to demonize anybody who has any questions or hesitancy about mandating a brand new type of vaccine like this?
I’ll admit: I was hard in on the vaccine. Got it as early as possible, worked to get my friend and family access as soon as possible (by helping them find volunteer shifts at the injection sites).
I’m not saying I regret these decisions, but I certainly acknowledge that the skeptics were right to be skeptical.
I think that I made the right decision at the time, given the information we had available, but I’m not sure I would make the same decision set today.
Many years ago I suffered from a severe reaction from Cipro. No one believed me. It caused tendonitis and nerve issues. I went to Mayo clinic and they did not believe me. Today, the medication has a black box label and mentions nervous system damage and tendonitis. I still encounter physicians who DO NOT believe it and refuse to accept it. The issue is still widely under the radar and individuals suffering from side effects receive nearly 0 help from western medicine.
I know now that physicians mindset hasn't changed very much over the decades.
In 1800s a doctor named Ignaz Semmelweis, discovered that "childbed fever" was being caused by the lack of washing hands and instruments. It took the medical community 20 years to accept it as a truth and he was fired from his job at the hospital.
Skepticism is fine, but anytime I saw skeptics questioning the impacts of vaccines, they always conveniently left out the similar unknowns about long-term effects of Covid, as well as the very well-known short-term effects, including possible death, which were obviously orders of magnitude worse than short-term effects of the vaccine.
It seems to me like a lot of the skeptics were skeptical of everything involving COVID - of masks, of lockdowns, of vaccines, etc. Which tells me they weren't actually interested in the science or long-term risks or anything like that - they just didn't like anything that was out of the ordinary.
I chose to get vaccinated and I continue to believe it was the right decision. More data may prove me wrong. We'll see, I suppose.
But research like this underscores the point that we should not be forcing or coercing vaccination. We also should not have subjected children to years of isolating and alienating lockdowns.
My In laws coerced me into getting vaccinated and honestly I regret it. We ended up with COVID more than my unvaxxed family. It's hard to forgive them or the government.
Why don't you expand on this vitriol? This guy regrets his choice and feels he was pressured to make that choice. That a valid human emotion that doesn't make them Q related at all.
I disagree, statistics demonstrated that the death number largely decreased among vaccinated.
As such to me "forcing" vaccination is legit if it saves more people than it harms, it's for the greater good.
Personally I don't want to risk my life because my neighbour is not vaccinated, but on the other hand no one is preventing my neighbour from relocating to an isolated hut on the top of a mountain and avoid any contact with anyone if he/she does not want to get vaccinated. But as long as my neighbour wants to live in a city then he must comply with the decisions of the majority of people, who, at least in my country, rushed to get vaccinated as soon as possible.
It's the same with politics: sometimes politicians are elected which I don't like, so I can either accept the decision of majority of electors and live with that, or I can move to another place. What I can't do is decide that I refuse to comply with a law because it was enacted by a government that I don't like or didn't vote.
I don't really understand this level of risk aversion. I'm probably old for hacker news, early 40s and my infection fatality rate is somewhere around 5 to 12 in 100k. I've got many hobbies and lifestyle choices that expose me to greater risk.
Even at 80 years old the risk of covid at worst is basically no different than wingsuit base jumping hard for a season. Yes of course if you can lower your 5% risk of death by all means the vaccine is worth it. Somewhere between 50 and 80 is a gray area.
I wasn't so much worried about death as I was about being crippled with long covid and having to deal with the medical system, that would probably not believe me for help.
This is true only in hindsight. The only reason you say that is because we actually kind of lucked out that COVID didn't turn out to be any deadlier, especially to younger folks. But when those decisions were made, that was not known clearly.
> What I do know is that the certainty was not at the threshold which justified mandatory vaccination
Why do you feel confident in saying that? Because I still don't.
I feel like it's still unknown to me how many lives or hours off work, or side-effects were avoided by the mandated vaccines, or were not.
And similarly, I feel it is still unknown how many lives, or hours off work, or side-effects were caused by the mandated vaccines, or were not.
Personally, I can't say if the threshold for mandatory vaccination was met or not until I know these things unequivocally.
What I could get behind, is an unrelated moral argument that would simply claim that free personal choice always trumps collectivism. But this would hold even if say COVID was super deadly to everyone and the vaccine prevented it, it would still hold that in the end it is each person's choice to get vaccinated or not, even if not doing so can contribute to the spread to others or their own death from the virus.
If instead we say there is a threshold at which indivualism has to yield to collectivism, I'm not sure I know where to put that threshold, or if the one that was decided for vaccination was wrong.
"It appears that it was indeed suboptimal for people younger and healthier than myself to take it."
Maybe it was suboptimal for them, but isn't the point that when you vaccine yourself, you're not just protecting yourself, but other people? Isn't limiting the active population that's infected a way of protecting both those who are immunocompromised, but in general, lowering the probability of everyone of exposure? Even if you're protected by vaccine as an old/obese person, would you feel safe walking around in a large population of young people with raging infections?
"What I do know is that the certainty was not at the threshold which justified mandatory vaccination."
2 million people are dead. That's more than the Spanish Flu of 1918, Polio, and Smallpox outbreaks in the US combined. It's equal to the total number of flu deaths over the last 40 years combined.
And you don't think public health officials had reason to want mandatory vaccination? I thank the gods those that came before my generation had the wherewithal to ignore this kind of logic and use widespread vaccination to eradicate Smallpox from the earth.
I was born in 1971, a year after they stopped mandatory vaccinations. My wife is not from the US, and she has the smallpox "scar" from her vaccination. If the remaining samples were to get out of the lab, I have my doubts as to whether or not the world will respond the same way it did 60 years ago.
Your argument could perhaps hold water if it were centered on the Johnson & Johnson formulation.
There is no precedent for a relatively novel technology being injected into everybody in a blind panic before a great deal of testing has been performed.
It was a huge gamble. It could have gone much worse than it did.
Before a great deal of testing? It went through multiple clinical phases, including a phase iii trials with over 40,000 people from April 2020 to November 2020.
By the time most people started getting it, the phase iii trials had been going for 11 months.
If there any any significant acute effects, they would have been found.
One can speculate about long term effects but one can also speculate on long term effects of natural COVID infection.
When Polio hit the US, the Salk vaccine was enthusiastically shipped out despite no long term tests either.
It’s amazing to me that people who talk in terms of risk minimization seem to simultaneously latch onto “natural” and “alternative” cures.
Natural immunity is bandied about as if there’s no risks involved and with claims or durability which are unproven.
> It was a huge gamble. It could have gone much worse than it did
But so could have Covid, that's why I say this can only be said in hindsight.
Also, the smallpox vaccine was pretty novel at the time when it was mass distributed, that was the first vaccine ever to be mass distributed. You'd have only similar trials as for COVID at the time, small sample, limited time frame, etc. You couldn't have argued it any more/less safer than the mRNA ones back then.
I don't think medical interventions should be forced on people, even if they need it. I'm for personal autonomy and choice. That said, I also like truth and accuracy and well reasoned thoughts, and it's definitely true that Covid could have been much worse, that the vaccine might have no measurable side effects whatsoever long term, and that forcing it on people did save additional lives that wouldn't have otherwise. Today's posted research paper actually tells us very little more on those topics, except that we need more research on LNP's possible lingering immune effects in humans and see the extent of it and if it even replicates in humans.
Acknowledging this doesn't mean you have to support using force or coercion on people, it just means being intelligent and honest about reality, facts, what we do know, and what we don't know.
That's what I'm here to do. Some people want to claim we now know for a fact that mandated vaccines did nothing and harmed people, this simply isn't true, we don't know that for a fact one bit, we just don't really know, that's all it is. If you claim you know, you don't, you simply believe it strongly without real justification to match the strength of your belief, aka an irrational belief. If you had that justification, it would easily convince others and we would not still all be arguing about it, but the data isn't there, the understanding of the mechanisms involved isn't there. Not yet.
It should be possible to separate the two topics. Do we want as a society which strongly favors individual rights, that we can push mandates in the name of the collective even if it means coercing individuals to do things they don't want to do?
And similarly discuss, if we wanted to save lives, lower the medical cost, and limit the spread or negative impact of Covid overall on society, is it better for a maximum number of people to be vaccinated or is it not?
Unless you're saying that coercion is only justified on individuals if the benefit to society are well known, probable, and sizable enough to some "threshold".
And I'm also happy to discuss this, even to agree with it, in hindsight, the benefits of the vaccines weren't as big as we thought when they first came around, people hoped it would end COVID, eradicate it like vaccines did for smallpox, and that hasn't happened yet. So maybe it didn't meet the threshold, but at the time it wasn't clear that it didn't, because I still remember that we didn't know how bad Covid was going to get, or how well the vaccines would help to fight against it. Thus, I still stand that, assuming this premise, that the right thing is to coerce if there is due cause that doing so will really be to the benefit of all, then at the time it could very well have played out to be the case. Why didn't we eventually stop the mandates sooner afterwards I can't say, but I'm also not sure this is the premise people assumed, I think many people assumed simply saving the most lives mattered more than a few people's resistance to wanting to take a jab in the arm. Is that just? Well it's a debate we're all still having.
> Unless you're saying that coercion is only justified on individuals if the benefit to society are well known, probable, and sizable enough to some "threshold".
This point seems too obvious to me to even warrant defending. Obviously, there must be an especially high bar to be met before we chase people down, hold them down, and inject chemicals into them.
Well, you could argue there are no apt thresholds at which this is ever justified. That the individual always trump the collective, so individual autonomy and personal choice should never be compromised, even if it could benefit the collective to do so.
And similarly you could say the reverse, the collective should always take priority, and in all cases where even minor benefits are to be found, the collective matters most.
When I took the vaccine, it was the beginning of Delta variant, I don't remember it being known at that time that the original strain would stop circulating or what the effects of Delta would be, and especially not long COVID related symptoms. I also didn't know a less virulent strain, Omicron would come and spread and take over the others. There was also the issue of ICUs reaching their max capacity, you can't have everyone be treated for severe COVID at the same time, so you needed a lot of people vaccinated fast to relive the medical system from that load. And finally, it wasn't known that it would still allow spread, or that it wouldn't work as well from Delta and Omicron as the original variant.
When I took it as a 30 year old in very good health, I did so to protect my parents, my older coworkers, my friends that are immunocompromised, and to hope to avoid a bad time and possible long Covid symptoms. I'd already known two people who had died from COVID, one my age by obese, and one elderly. I wasn't worried of dying from COVID myself, but I still didn't want to get it, and I was worried of long term effects, still am on that.
Even now, I don't think anyone can claim a unanimous decision was better or worse, even in hindsight. The positive second order effects of vaccination are not clearly quantified, the negative effects of Covid long term are not clearly quantified, and the negative effects of the various vaccines are not clearly quantified.
The reason we're even all arguing about it is because it's very ambiguous knowing which is best, vaccination or not. If it was obvious one was a better decision we wouldn't be having all these debates of opinion.
Even though it is my opinion, I don't agree that it's morally bankrupt to think otherwise. Agreeing on values is one of the hardest things to achieve.
Some people have a collectivist leaning, others an individualist leaning (and this can depend on a per-issue basis even within the same individual).
Some people think the morally correct goal is to save as many lives as possible in the short term, while others think individual autonomy and personal choice is more important. Some are in the middle, putting the threshold slightly lower or higher in either direction.
You and me simply lean more towards favoring personal autonomy and choice, at least on this issue apparently.
Luckily, our societies have evolved diplomatic methods to solve these conflicts of values, through the democratic process and pre-agreed on laws. Instead of going to useless war or leaning on force, we put the elected officials in charge of the decision on the effective policies, and each one looked at the tradeoffs, looked at their constituency, looked at the limited data available, and made a decision.
The HN title seems to be somewhat misleadingly chopped. The study here showed that injection of a fake vaccine (coding for GFP) in mice appeared to reduce the effectiveness of future vaccines (coding for influenza) that used the exact same delivery mechanism.
Note that this a preprint, but appears to be accepted for publication, though may still undergo revisions to this draft.
So... exactly the same problem with adenovirus-vector vaccines, in that each vector virus is "burned" by the introduction of a vaccine using it? That's somewhat disappointing.
I think it was quite different from that in this study. This result appears to suggest that the mRNA remained an effective vaccine vector against new viruses, but suggested that it also slowed the body's immune response to an unrelated yeast infections in the week immediately after vaccination.
If I understand correctly, they then also showed that vaccination pre-pregnancy has inheritable benefit to their offspring in reducing the severity of illness in their children.
> If I understand correctly, they then also showed that vaccination pre-pregnancy has inheritable benefit to their offspring in reducing the severity of illness in their children.
Mothers pass on all the antibodies they have in their blood and breast milk to the baby. This effect diminishes greatly after colostrum is gone and stops as soon as the baby is weaned.
This can be considered an external immune system. Once the baby is weaned, it is fully vulnerable to all the diseases it might have been protected from by its mothers antibodies.
When vaccination was required to keep participating in social life this was my motivation to get a second JJ vaccine despite the pressure to get an mRNA vaccine. I assumed my immune system would have an easier time to remove it from my body.
There was another study showing DNA transcription, and you dismissed that too - not on any scientific basis, but because "anti-vaxers" discussed it, and you apparently had some issue with the journal.
You're all over this thread getting aggressive with people; accusing them of being Q fanatics and the like, without cause.
Kindly, consider that your anger might be covering for fear, shame, or something else. And even if it's not - could you rein in the general toxicity?
Well I find your comment very rude. Please concern troll and police and control someone else. I don't have to pretend like I lost my brain and forgot the last 3 years like everyone else here.
Where exactly should this be discussed? We've seen that any COVID discussion that goes against the main narrative gets blackholed, people get cancelled for wanting to push the breaks, everyone gets pushed into a one-size fits all "solution" and we're finding out that we still need more data.
Yes, a lot of places have quality control that removes the tiring "just asking questions" concern trolling and bad faith arguments from people who don't understand the basics of epidemiology. This comment section would be better with the same moderation. Confusing dissent with informed dissent is a big problem on "free speech" platforms.
I feel like the opposite. I really am not here to read about machine learning or JavaScript. News and comments on non-IT subjects are the real gold of the HN.
There are far worse places. I think the HN crowd is pretty good at looking and analyzing data (regardless of the source). There are many other places (respected and non-respected) where the audience takes as gospel whatever the newsreader says (irrespective of whether supporting or muddling data is presented).
> I think the HN crowd is pretty good at looking and analyzing data
Seriously, look through the comments on this article then compare the general antivax tenor to literally anywhere with experts. It frankly reminds me of the 9/11 truther "jet fuel can't melt steel beams" tropes that were repeatedly and patiently proven wrong by engineers, only to have the number of conspiracy theorists grow in number and confidence.
Y'all are gonna be much scarier, convincing, whatever, whenever you realize that the little extra certain imagery that you just had to throw in there exposes you. People would accidentally take you more seriously if you could manage to get (whatever that energy is that requires you to induce phallic imagery) out in some other way than in random comments about vaccines.
This is in fact an argument against censorship and for dispassionate and objective reporting where you don't take the word of government representatives or pharma executives at face value. If the (mainstream) media cedes this ground to more conspiratorial voices, whose fault is that?
Because only Rogan has both the platform and enough f-you money to not care if he's deplatformed from the internet in total? And let's be honest: controversy drives interest, just like the MMA fight coverage he's a part of.
I suspect he's genuinely interested in the topics at least for a while. I can relate to a certain degree: when I am learning something new I deep-dive on a topic and talk to people who know things about it, I just don't have access to people to interview like Rogan does. In my case, once I exhaust my learning on a topic I usually never care about it again (eg: is a 56V cordless drill inherently superior to one that operates at 18V) and just move on to other interests though while I'm learning it's like a fever that I cannot shake until I get to the bottom of the inquest.
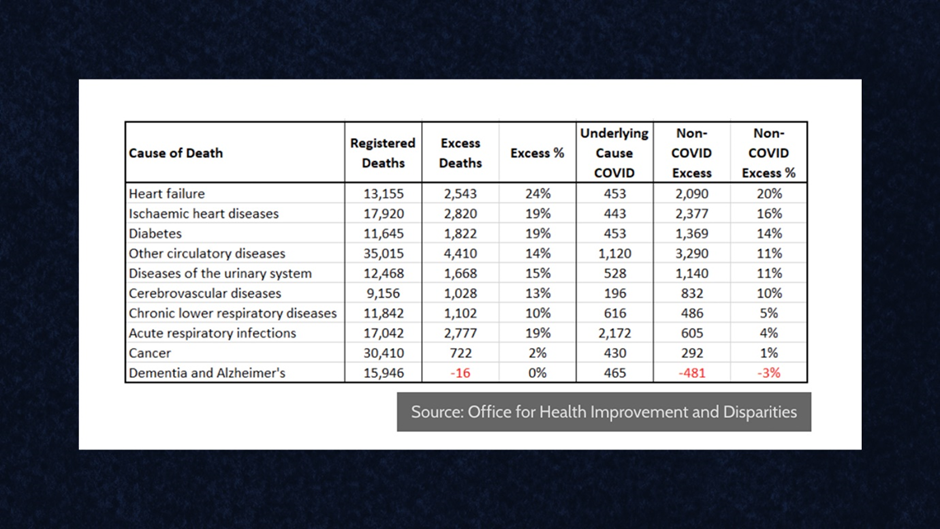{kind=link}
{kind=link}