Of course while YMMV, I've found the same thing - I've been prescribed opioids for pain, and I found that Advil worked just as well, without the side effects. I do understand that opioids have their place - for example I was told that Advil was not safe to take before surgery so I was stuck with the prescription meds.
On example that made an impression on me: a couple of years ago, I had arthroscopic surgery on a knee. When the surgery was done and I was being discharged, a nurse came to me with a percocet script and told me to take one every xx hours. Having taken percocet in the past and being familiar with the aforementioned side-effects, I asked her if she wanted me to take it for pain management, or if there was another reason to take it (blocking the formation of blood clots for example). I'm fairly pain-tolerant, so if it was a pain management thing, I wasn't going to take it. Her response was "just take the pills." That was not helpful. If doctors and nurses are just shoving these things down patients' throats it's not surprising there is a problem out there.
Digestive problems are so common with long-term use that some doctors think that they should co-prescribed with omeprazole and other agents to head them off. (Long-term omepraloze will give you B-12 deficiency if you don't supplement; it is an unusual side effect, but I can't sleep if I take omeprazole.
Cardiovascular risk from Vioxx was enough to pull the drug from the market; risk is also seen with Celebrex and other COX-2 selective NSAIDS. The risk with non-selective NSAIDS is less understood but still present.
My doc does not want me taking acetaminophen because she thinks it causes me to get elevated liver enzymes.
Like opioids there are problems when people don't "use as directed". My grandmother used to take Bufferin by the handful and one day at the dinner table we saw her throwing up blood like something out of a horror movie and she was subsequently hospitalized..
Acetaminophen overdoses can easily destroy your liver and are one of the most common forms of fatal poisonings.
The verdict is that we don't have truly 'safe and effective' medicines for pain in 2017.
This study only looked at acute pain. Generally those medications are safe for acute pain.
(Unless by 'safe and effective' you mean NEVER have side effects, in which case we probably don't have any 'safe and effective' medications.)
Chronic pain is difficult to deal with and wasn't addressed in this study. Generally opiates are not recommended, but its tough to find other alternatives that are consistently safe. Opiates often end up being used and... epidemic. (... == long complicated story)
That's a bit like saying we don't have food that doesn't cause obesity. What is your definition of safe? what is your definition of effecitve? If a person turns up to the emergency department in severe pain from trauma, I can safely relieve their pain without endangering their life, that is both safe and effective. If an elderly person with arthritis of the knees is on 3x daily 1330mg Paracetamol SR for months and months, that is both safe and effective.
Paracetamol/Acetaminophen has an incredible safety profile - in people who use it responsibly and don't have liver disease.
It is, after all and as you are obviously well aware, responsible for the highest number of ED presentations for overdose, and it does kill a number of people each year. But that's a mental health issue, and you can overdose on Water (or food, as I indicate in opening paragraph), and die. For people who take it responsibly and without intent for suicide, it is incredibly safe and effective.
Same with ibuprofen - although with the proviso of Do not take for more than several days. But, the same could also be said of opiates - safe for short periods. it's chronic use that will cause problems in lots of cases (ie. add in benzos as well)
The topic at hand is acute pain management in the ER, you seem to be talking about chronic pain management, which is another (more complicated) topic altogether.
Cannabis has pretty awful side-effects for me. It gives me absolutely incredible nausea, to the point where I've tried it ~10 times in varying doses, thinking my dosage was an issue, and out of those I was violently ill 4 of the times. The other 6 times were simply unenjoyable.
It doesn't just go away like alcohol either. If I drink too much and throw up, I feel better within a few minutes. For cannabis I remain high afterwards, so I've become pretty hesitant about it.
That being said, it is very likely less addictive and has far fewer side-effects for those who it helps. For that reason I am extremely positive about legalizing it and studying it further. :)
A lot of people who take cannabis for pain or anxiety take CBD [1] rather than the raw THC-containing plant. There's almost no associated high, so it sounds like you haven't tried it. The abuse of medical marijuana laws to circumvent prohibitions on recreational use has confused the issue, but people shouldn't equate the substances that get consumed recreationally with the much more processed and specific substances that get used medicinally.
Sorry to pick on you, but people should realize that if all they want to do is try cannabis for pain management, they shouldn't let a dislike for the recreational effects deter them because the two can absolutely be separated.
FWIW, I manage my pain with meditation techniques and it's the only form of pain management that I recommend whole-heartedly, so I'm not recommending anyone try CBD. But I know people who take CBD for pain and I think people should, at least, understand how cannabis is used medicinally before saying negative things about it.
I never touched the stuff, but I would end up having to take my friend to the ER. For some reason at different times it would cause an allergic reaction and he would act like he was in septic shock and have dementia.
Doctors and I were convinced he was not telling the truth or his stuff was laced. Ended up that he was telling the truth and was clean other than pot. Sad thing was he would keep using pot which ended up messing with his health.
I never see why people care to be sedated emotional. Worst thing about pot to me. They miss out on so much emotionally.
If you don't understand why people would avoid the full force of their emotional response to life then you apparently have had great fortune in your emotional experiences. I note you don't have to want it for yourself to understand why others would want it.
Cannabis enhances my emotions. I'm normally pretty flat emotionally and cannabis is one of the only things that changes that. I'm not sure what you mean by sedation here.
Who the hell would 'lace' weed? With what, water? Nearly every other dug costs more to lace it than just sell it de novo. THC as a drug is SUPER cheap with the various 'legal' states. Even at high-end stores, concentrates are $25/gram [0]. This reads like some ham-baked DEA post.
Yep! I tried edibles, joints, and vape pens from 3 different dispensaries in the bay area. The edibles and "free" joint I got from Airfield Supply Co. were the ones that effected me the least negatively.
“Respond” is an understatement. 10mg THC, with no CBD, represents a typical edible from a dispensary, but as a small person with low tolerance and a fast metabolism, I’ve found that amount of THC by itself ends with me fearfully holding onto the Earth for dear life for a couple hours.
On the bright side, at dispensaries you can know precisely what you’re getting, so at least I can say “this weed will pleasantly reduce my anxiety and pain, that weed will blast me unwillingly into space” which is an option I never had before.
Anecdotal, but I can't imagine living a normal life while regularly using though--even if regular is just a couple days a week.
It's legal where I live and the handful of times I have used during the week, I can't remember what I did the day before as well, or what my tasks for the day are. My performance at work noticeably degrades. I'm also more tired the day after, despite generally getting more sleep.
It's great for the weekend when I can just sleep it off or my only tasks are to go for a hike and get groceries though. Better than alcohol at least.
I'm curious what makes it great for the weekend for you. Not being able to remember what your goals for the day are or remember what you did the day before doesn't sound great, even if it is the weekend.
I suppose I was thinking in terms of the alternative being alcohol. If I were going to choose between a night out drinking, or a night out having smoked a bit, I'd go for the latter. I'd rather feel a bit hazy the next day than be sick to my stomach or have a headache--which I get even just from ~3 beers over a few hours. I could of course opt for neither, but social norms being what they are.. there's some pressure there but that's a separate issue.
That being said, I may have exaggerated the memory issues. It isn't like full blown amnesia. More so it just takes longer than usual to remember things. I'd compare it to a cache miss. Smoking clears my brain's cache the next day and I end up feeling like I am pulling short-term thoughts and memories from colder storage.
I'm not the person you are responding to, but I limit my cannabis use during the workweek for similar reasons. Most often my goals for the weekend are to relax and enjoy myself. Of course I'm not going to get high if I'm about to fill out paperwork to refinance my mortgage.
It may help to note that THC and CBD are two active components which can treat different symptoms. I find CBD extraordinarily effective at treating my essential tremor. CBD and THC combined provide mild help for my pain, but THC makes me anxious and spacey. The side effects don’t quite outweigh the benefits for me, personally. But I cannot recommend CBD enough, and agree both are worth trying.
So many innovations in medicine, food, exercise, pesticides, whatever, only look better than the old stuff because they haven't been around long enough for all their flaws to be discovered.
True for high-THC strains, but not high-CBD / low-THC ones. And of course opioids also famously affect perception: "do not operate heavy machinery" etc.
I have heard that CBD is extremely great as a natural anti inflammatory however the strains that get recommended are so absurdly expensive. On the order of 30ml for 150$ for charlottes web for example. Is it actually worth it? How long does that 30ml bottle last for 150$?
The bottle lasts approx 2 weeks with 'correct dosage'. And that price is the higher end product. I am familiar with the mid-range product which I used for 1.5 months (due to pain) and discontinued it because I honestly couldn't really tell the difference.
Yeah this is quite disheartening to hear. 300$ a month for something that some people can't even tell the difference with. I don't want to spend 150$ for 30ml of snake oil haha.
My wife has a number of health issues (chronic knee pain, low-level anxiety, CFS). She tried the same CBD oil for about a month and found it had no effect one way or the other.
you're referring to the LP prices, i.e the "legal" stuff. you can buy far higher quality CBD strains at dispensaries, or even black market dealers, for cheaper.
> My doc does not want me taking acetaminophen because she thinks it causes me to get elevated liver enzymes
An uncle and some other older physicians who are on long-term measured acetaminophen usage reported supplementing their regimen with n-acetyl cysteine (NAC) with no apparent diminution in analgesic effect. WebMD has a description of the chemical mechanism:
I had some bad reactions to NSAIDs (asthma attacks & bad headaches). I was never sure if I was having an attack come on and thus took aspirin, or if the aspirin was causing it. Eventually I went to a doctor and it turns out there's a allergy-like sensitivity to these things that some people have.
I agree the nurse absolutely should have answered your questions about the medication or gotten a doctor to answer them. It's just inexcusable behavior on her part.
Did the script say "P.R.N?" PRN means "as needed" in medical terms. It's an abbreviation for "pro re nata." Just for future reference.
I've also found that, for me, naproxen (Aleve) works much better than opioids. Opioids just make me feel very, very sick (from nausea). If they do help with the pain relief I can't tell over the nausea and vomiting.
There's a fairly big camp of people both online and in real life that is strongly against questioning medical authority. I've encountered it before.
For example (and I know this is purely anecdotal), after doing a few hours of extensive research and photography comparisons online I came to the conclusion that my sister had shingles. I mentioned this to the doctor when I took her and he dismissed it and said that it is unlikely since she is so old. I mentioned this on a subreddit that I frequent and a bunch of people jumped on me and told me to stop doing my own research and to let medical authorities do their job without me pestering them. However, after taking her to a different doctor, he immediately recognized it as shingles and prescribed her the appropriate medicine.
On the one hand, I get why doctors don't want the "ignorant masses" doing their own research and coming op with cockamamie theories, but on the other hand, doctors can only hold so much information in their heads whereas the internet has vastly more information available and I can become an expert in one tiny little niche fairly quickly.
After a number of years with a different diagnosis, I convinced an ultrasound technician to go beyond their exam script -- enough to discover that, in fact, I did indeed have a minor hernia.
If the doctor hadn't been so sure of his diagnosis, this would have been caught years earlier. I'd specifically asked, more than once, about the possibility.
A lot of scrambling on their part, that day, to get me a same-day appointment for consult with a well-regarded surgeon.
A useful approach is to ask "could this be shingles?", and then "why not?", and then "if i isn't shingles what else could it be, and why is it that and not shingles?"
the UK has had a campaign recently around sepsis where people are being trained to ask these questions.
It's a fine line. Most of the time, the patient is actually wrong, and that can make it pretty annoying, especially if the medical professional in question is having a stressful day (and aren't they all...).
I have a lot of medical knowledge and I try not to be a wise ass with my doctors. Sometimes though, it pays to pay attention.
I always like to come to a Dr's appointment with a "sealed envelope" ... what I think the problem is, but not to mention it until they get through with their diagnosis.
Yes doctor, no doctor, I don't think so doctor, yes doctor also my left foot. => He thinks I have a sprained ankle, I think I'm not sleeping well (or whatever) and I'll mention what my guess is at the end (not before) and ask him why my guess is (presumably) wrong.
Of course if you think there's something unusual or your symptoms are severe then of course go to the doctor without delay, but it's also helpful to get a bit of a personal education when you've got time with a specialist.
I had a slightly different experience, luckily, I guess. When I was in recovery after having a brain tumor removed, I was first being given fentanyl once every hour or two. I found that for the few minutes I was lucid (before the next dose), I really didn't have much pain and asked for something less strong. They moved me to norco, which still seemed too strong. After another request for something less, they moved me to plain tylenol.
I did get a big script for norco when I was discharged, but their instructions were to take it if the pain became distracting.
The nursing and medical staff at the hospital (CPMC Davies) overall seemed great, so it may just be the difference between staff that listens/tries and staff that doesn't.
Same here. After a LONGGG phone call cradling the receiver while trying to type, etc., I had my neck spasm severely -- so much so that the following day someone else had to drive me to urgent care (1). They prescribed a strong muscle relaxant in combination with either Percocet or Vicadin -- I forget which.
I switched over to the default over the counter dose of ibuprofen, and it worked better than the combination of those two "heavy duty" prescription drugs.
I will say, though, that doctors in the U.S. have been damned cavalier about ibuprofen. One doctor with a popular radio show would cite the nickname, "Vitamin I", and routinely tell people to use it non-stop for a month or two.
I've found that now, a few days on it will make me rather lethargic. My cardio strength and sometimes rhythm feels impaired. And lo, there are studies now coming out that indicate it may carry as much risk as Vioxx and the like.
(Incidentally, a doctor prescribed me Vioxx a month or two before it was yanked from the market. I questioned this, remarking on recent news I'd read indicating it had problems. He had no clue and told me it was perfectly safe. Sure, it was still on the market, then, but he appeared to have no clue about the looming controversy.)
With any medicine, it really seems TANSTAAFL. You have to carefully weigh the benefit against known as well as suspected risks. And the U.S. medical system completely falls down in not fully informing not just patients but also doctors to the existence and nature of these.
1) Well, that urgent care experience -- a new facility opened by the premier area hospital -- was itself a horrible experience. Deserted facility, by all appearances, yet it took about 2.5 hours to see a doctor. Who gave me no neck brace; family took me to their chiropractor, the next day, who DID give me a neck brace -- which provided the first real relief and stopped me from constantly retriggering the injury with every movement.
To be clear, I refuse to have my neck cracked. And the chiropractor wouldn't have, at that point, anyway, given my severe spasming. But at least he had the sense to immobilize my neck. (Then he provided some ongoing care to encourage the release and healing of the spasming. To whatever extent this may have helped, that initial immobilization was key. WTF was wrong with that fully credentialed MD serving the urgent care's rather extensive ER facility?)
I've found through my experience that the choice of urgent care vs a non-urgent care doctor is more important than I have always thought: An urgent care center wants to focus on the shortest path to getting you relief (your story aside). They'll err towards slightly over-prescribing. The non-urgent care doc will take a more comprehensive treatment path.
A slight distinction that might not matter sometimes, but i often wonder how many antibiotics/pain killers I've taken prescribed from urgent cares that were possibly overkill.
Yeah. Rather than your typical urgent care facility, this was the hospital's initial effort to significantly expand its effective service area. It was a quite substantial building -- since expanded to the size of some hospitals -- and they had labeled what I used an "emergency room". My family suggested going there as it was a lot closer.
That ER doctor just gave me the prescriptions and sent me off. No follow-up care. I guess you'd have had to see my level of discomfort. My family was equally surprised and disappointed.
I take your point. And much of the U.S. health care system keeps pushing patients towards urgent care and "the doctor at hand". Not that there aren't good urgent care staff; nonetheless, it doesn't exactly promote medical management.
Also, I've delayed some care because I've been uncertain of the approach and awaited more information and perhaps improved procedures and techniques. This might well be called a conservative approach -- and these days, so much of the U.S. rhetoric is about the need to be "conservative". Well, much of that is actually "Conservative", which is actually a rather different ideology.
Yet, insurance keeps worsening by the year. Patients who might otherwise be inclined to be conservative and await better knowledge as well as what would normally be lower costs (in most other industries, "product" costs decline with age and with technical improvements and growing marketshare). Well, in U.S. health care, patients can feel compelled to "act now", because while technology and standards of care may improve, next year's insurance may well not cover it or cover it enough for it to be affordable ($5000 deductible? $7500?), if one even has insurance next year.
For the ER in our town to take you seriously you would have to have visible bullet holes or severed limbs. Otherwise they dismiss you with a condescending sneer.
pasbesoin says> " They prescribed a strong muscle relaxant in combination with either Percocet or Vicadin -- I forget which.
I switched over to the default over the counter dose of ibuprofen, and it worked better than the combination of those two "heavy duty" prescription drugs."
Had you continued the muscle relaxant (the problem was an involuntary muscle spasm), you possibly could have avoided further treatment (the neck brace).
If I suffer a muscle spasm that can't be massaged out, then a muscle relaxant + ibuprofen serves well for 1-2 days and, after that, only ibuprofen.
IMO muscle relaxants + narcotics is not a useful combination, their purposes(muscle relaxation vs pain-reduction) being orthogonal, except in cases of severe injury where near-immobilization is required.
I was on the muscle relaxant for a full day, and I was no better. Any time I moved, I was retriggering the spasm.
The neck brace stopped that. I still had to be careful, but at least I could walk around and sit and such without constantly re-spasming (which I suspect was actually exacerbating the injury).
I do agree in concept with the concern about combining such an injury / muscle relaxant with strong pain killers. The pain is warning you as to damage; numbing it seems like it might well promote furthering that damage and/or hindering healing.
In my case, once I was braced and stopped retrigging -- and possibly worsening -- the spasming, the remaining pain was entirely tolerable. Of course, the limited effective activity was another aspect requiring coping. That included sleeping: Getting into bed, and keeping things immobilized in bed, was a bit of effort. I learned how to sleep with a neck brace on, and I "trained" myself quickly not to roll from side to side -- despite my allergies that promote frequent shifting.
I was going to post a similar opinion specifically of percocet: it was prescribed for me after a surgery, it gave me a weird sense of detachment, but didn't seem to do anything particularly significant for pain.
I stopped after the first one.
I have enough addictive behaviors, I don't need to add a chemical one.
God do I hate medical
professionals like that. It's as if they don't want you to steal any of their elite knowledge or that you as a patient are beneath them. How dare one of us ask a semi-intelligent question!
Agreed, I've been lucky and only required a few surgeries in my life. Every time I get handed a jug full of opiates, and end up taking ibuprofen instead. Personally the pain management I get from ibuprofen is similar (definitely less, but sufficient) to the opiates but without the side effects.
This is not the case when you suffer major 3rd degree burns. When you need morphine in the case of say regrowing nerve endings in a damanged limb advil will not cut it, not even medical cannabis will cut it, there are still cases where giving a patient morphine is appropriate.
The discussion around opiate abuse isn't about the extreme cases. Yes, if I get 3rd degree burns then I want to be as out of it as possible until the pain goes away.
The problem isn't the extreme cases, it's the every day ones. Opiates are being massively over-prescribed in cases where OTC medicine or a shot of whiskey would suffice, and this over-prescription is a driving force behind the addiction epidemic.
Not sure if you said it in jest or not but alcohol is also highly addictive, prone to abuse, and harmful to your health and IMO would really not be a step in the right direction.
edit: I almost added to my comment "It's almost taboo in our society to mention this fact" but didn't. I was almost immediately down voted so I guess maybe I'm not wrong...
I'd say it's extremely taboo to mention anything negative or even the possibility that alcohol is one of the most abused and disruptive drugs in our society.
People don't even like to call it a drug, which severely bothers me to be honest. I've tried some things and alcohol, from my perspective, is one of the more dangerous drugs around
As on expat UK-> USA said if you have a pint for lunch people start leaving AA leaflets on your desk.
A while back I was talking to a course tutor who in the UK gave the "dealing with staff with serious addiction problems" course - he commented its when you find 3 or 4 stashes of vodka hidden in the office that you know you have a problem
Took morphine for a back injury, I just got sleepy but still had the pain.
Took Percocet after a shoulder surgery, I just slept through the pain. I also understand now why people get addicted.
I get raging migraines, Excedrine is the only thing that works for that.
True story, when my daughter was in the hospital (cancer) we overheard a nurse and doctor discussing what to give a child (also with cancer) for tooth pain... "morphine". The nurse was like "for a tooth? can't we tell the mother to give him Tylenol?"
Also, true story Tylenol is not "formulaic" (I may be saying that wrong) at many hospitals. Meaning THEY DON'T KEEP IT IN THE PHARMACY (the one that fills orders for internal use). I was very surprised to learn this.
I find it very odd that a nurse would be so cavalier about that. There are a lot of people who can't/won't take prescription pain meds for a myriad of reasons. Some are concerned about addiction, but other reasons are religious/philosophical. I've always been asked if I want those kinds of pain meds, even when they are highly recommended, it was always a question.
All the commenters thus far seem to think they know more than a randomized clinical trial that was double blinded looking at oral (not IV morphine) combination doses of opioids like codeine, hydrocodone, and oxycodone with tylenol vs ibuprofen+acetaminophen (tylenol). Here's the actual study if you would like to read more...
I'd like to note that their p-value was awfully close to the statistically significant differences in pain reduction, so a larger study is definitely warranted.
We've known for a while that IV acetaminophen is just as effective at pain reduction in acute pain compared with IV morphine, as well. See this study, there are more similar to this:
For those of you that think that a few doses of opioids can't cause addiction, think again. This study found that even after 10 days supply of opioids, 20% of patients had a dependence lasting up to a year.
I've seen patients get 30 day supply for appendectomy regularly, and my dentist friends have prescribed up to 50 at a time in the past.
We need to do these studies, and discuss them, and make them better, so that patients get the best care that they can. What we absolutely cannot do is rely on anectodal evidence to make clinical decisions.
> For those of you that think that a few doses of opioids can't cause addiction, think again. This study found that even after 10 days supply of opioids, 20% of patients had a dependence lasting up to a year.
The study did not find that. The study looked for long-term opioid use, not addiction, and not dependence. Long term use, addiction, and dependence (and tolerance) are all separate things.
Long-term use: simply using a thing consistently for a long time
Addiction: compulsive seeking, not noted in any of your links
Dependence: something bad happens when use is discontinued
Tolerance: more use is required to get the same effects
You're right, thank you for the clarification and I apologize for misleading. This study did not look at addiction.
However, the study noted a few things that lead me to believe that this long-term opioid use is not intentional by prescribers. The study excluded patients with cancer, which is a common reason to be prescribed long term opioids. Additionally, they note that most of the patients were not provided long-acting opioids at the start, suggesting that the prescribers did not intend to start these patients on long-term opioid therapy.
At the very least, the data is suggestive of an increase in dependence in patients prescribed a 10-day or greater supply of opioids, as we know that when patients are on opioids for too long, you must slowly discontinue lest you initiate withdrawal.
Yup -- requesting an edit of the link title to clarify that it's about oral analgesics only, not IV analgesics, since this has indeed been a major point of confusion for several commenters.
To clarify even more, it also doesn't address cutaneous delivery of opioids or other analgesics for people who are unable to take either IV or oral applications.
You are absolutely correct. I was just noting that even if individuals think morphine is the best at reducing pain, there are other options related to this article.
Ok. I just think it’s important to remember that different people handle pain differently, and we shouldn’t end up refusing people something that helps them because an average in a study said it wouldn’t help. That does need to be weighed against the danger of addiction/dependence, though.
The title of this link is frustrating and misleading. The article clarifies a bit, but I take issue with Ars linking to the specific study with text stating the methodology is the gold standard. That doesn’t mean the conclusion will hold up to scrutiny, or that “extremity pain” is a meaningful dimension. The type of injury (eg. compound fractures, sprains, etc.) could be more meaningful than where the injury is. There’s no control for injury location.
Also, the CDC guidelines state that opioids are recommended when other treatments fail (regardless of the underlying condition). That key facet was excluded from this article. Ugh.
Apologies, this is a bit of a rant. I have a very painful chronic neurological condition that often requires powerful opioid pain medication to get out of bed (and not commit suicide). Please keep in mind that there are legitimate use cases for opioids. I don’t like them, but combined with biofeedback, PT, mindfulness and relaxation techniques, I’m able to survive until my condition gets better (if it does).
We all understand that opioids should be avoided when possible. Addiction is horrific. I don’t think anybody is arguing that. But please help stop making life exponentially harder for people with legitimate problems that effectively require opioid medications as part of a treatment plan. We have it tough enough already.
The only way out of the current situation is to develop drugs that are at least as effective as opioids, but not addictive (and ideally not psychoactive). I’ve tried everything (yes, an NSAID + acetaminophen, and even intrathecal Ziconotide), but we just aren’t there yet. I hope we get there soon, because I’m sick of the mental cloudiness and health risks of opioids. I want my life back, and I’m sick of fighting just to maintain an acceptable level of pain management.
I was about ready to chime in the same thing. I've been on opiods for six years (not by simple choice). I'm also on a literal 15 other medicines. I take around 30+ pills a day I've had multiple back surguries. I've got on average 3 doctor visits a month (those co-pays add up fast!)... for six years. And this all started in my prime... at 25 years old where I went from starting a Ph.D program... to fighting with every ounce of my strength and mental fortitude to keep from being homeless.
I'm not sitting around, popping pills to get high. And, you can't magically get addicted to opoids if you never take increasing doses (read: follow the prescription). The longer you take them, the high rapidly goes away (drug addicts "chase" it by increasing doses) while the pain relief stays usable for a _much much_ longer period.
After six years, I've gone down on dosages slowly. The relief works fine. And I get zero high. It's like taking a Tylenol for me except it actually helps my pain.
Meanwhile, for 6 to 9 months when I lost my insurance I was stuck with over the counter medicine. I destroyed my gastrointestinal tract and almost my kidneys, just trying to take enough medicine to not commit suicide from the pain.
Are opoids being over perscribed? Yes. duh.
Does treating anyone who takes opoids into an addict, help anyone? NO.
People need to get off their high horses (ha, pun.) and realize pills are pills. You can argue for reduced perscriptions but the second you start villifing actual patients by telling them "you're pain isn't real. just take some Tylenol" you're now apart of the problem. You're not stopping a single person from getting high. You're just helping oppress people who are already so !@$!@ed up that they barely have the energy to keep going, let alone defend themselves from the public's armchair warrior researched lynching.
I've moved plenty of times. I've seen literally dozens of doctors. And almost every single one of them agreed with my diagnosis that I should be on this medicine. What makes you think reading a bloody internet magazine article about a single study makes you think you know better than the doctors who are trying to save my life?
So while yes, I think most people here are more reluctant to be as judgey--and I thank you for it--there are still plenty of people abusing sources to make their soap box point. They think opiods are automatically evil. They're not. They're the "right tool for the right job." end of story. And just because one research study says they're not useful for specific scenario, doesn't mean all scenarios are some secret conspiracy to get healthy people high.
I don't "want" to be an ANY of these medicines. Every single one is a potential liability. I have to keep them with me when I go places. I have to keep them safe from thieves (!!!) at home. I have to monitor how many each I take a day. At 25 years old, I had two 7 day pill counters just a 85 year old man. We don't _want_ to be on these medicines and deal with their side-effects upon side-effects. We're taking them because we have to and the other option is to simply roll over and die.
So forgive me if I sound emotional, when literally one of the tools that keep me alive, is being threatened by both conservative and democrats looking to grandstand to their constituents while nobody actually does anything to stop the abuser.
You can't imagine what it's like when you see someones face (nurse, doctor, police officer) completely change and withdraw the second they find out you're on an opoid. It's unreal. The entire room "goes cold." I dare you to try telling someone that. They stop talking to you and talk _at_ you. I've literally had a cop lie on a police report when he found out I take a medicine that I'm 100% legally prescribed. I've had receptionists not forward my calls to the doctor. I've had people scout out and follow me home.
All because I chose to put a pill in my mouth that a doctor told me to.
I could write an entire book on this stuff by now. I've considered building a YouTube channel about it. As a scientist, I can tell you, it's like walking into another world.
I have a very good friend with a similar story about long term back problems. He was on oxycontin for literally 10 years along with other medications. Multiple back surgeries.
Then when his prescribing doctor got arrested, he ended up detoxing involuntarily at first, and then voluntarily, and he found that he didn't have any pain after he managed to make it through withdrawal.
I honestly think a lot of people with chronic pain that they're treating with opiates are actually treating withdrawal with opiates.
There are medications being developed for conditions like yours. Nav blockers that work only on specifically nociceptor circuits. I have high hope for targeted compounds like this, it would improve the lives of millions.
Agreed that opiods are overprescribed, but for acute pain there's no comparison. At least in my experience.
I was rushed to the ER with an excruciating condition, and i popped quite a bit of ibuprofen at home before going to the hospital (i think 4-6?). Nothing.
In the triage room or whatever, that morphine drip (plus saline IV to replace all fluid i vomited up due to pain) made the 8/10 pain reduce to a 2-3/10, allowing me to bear with it until i was put under general anesthesia for surgery.
>In a randomized, double-blind clinical trial—the gold standard of trials—a combination of ibuprofen (Advil) and acetaminophen (Tylenol) was just as effective at treating patients with acute pain in an extremity as three other pain-killer combinations containing opioids.
They tested medicine combinations (400mg of ibuprofen and 1,000mg of acetaminophen), not ibuprofen alone.
Extremity pain (arms and legs) was tested only, not pain in general.
They only tested medications delivered orally, not intravenously. That distinction is very, very important as intravenously administered medications have a much higher placebo effect than orally administered medications. In fact, I'd love to see a comparison of orally administered opioids vs intravenously administered NSAIDs.
They didn’t say opioids are no better than either acetaminophen or ibuprofen; they said that opioids are no better than the combination of ibuprofen with acetaminophen — something very rarely prescribed (and usually advised against on the labels of both drugs.)
counter-anecdote: my doctor told me to use precisely that combination for severe pain. She said you cannot combine multiple NSAID's (ibuprofen, naproxen, ASA), but you can combine an NSAID with acetaminophen.
Agreed; I've been prescribed that combination more than once by different doctors. It's very common, and often the recommendation is to stagger them. NSAIDs are metabolized by the kidneys and acetaminophen is metabolized by the liver, so they can be safely combined.
EDIT: also, this is pretty much what Excedrin is (aspirin instead of ibuprofen, but NSAID + acetaminophen, plus also caffeine)
As a migrainer, excedrin really only works part of the time. Though, opioids really only succeed in making me not care about the pain. I’m still in pain with them.
The best treatments, for me, directly address whatever underlying issue.
Drifting off-topic, but have you tried sumatriptan ("Imitrex")? It seems to have a near-total effectiveness on my ~monthly migraines. Neither acetaminophen nor NSAIDs ever did anything for my migraines.
I agree that directly addressing underlying causes like stress, noise, sleep, and diet are better than a pill.
I was about to say the same thing - sumatriptan works amazingly well for my migraines. I'm in the UK though, and I seem to recall someone on HN saying it was very expensive in the US.
It might have once been expensive ("Imitrex" (R)(TM)) but there is a generic now. I understand there are also non-pill delivery systems, like nasal or patches, and other permutations that may still be under patent. The pills seem to work for me.
It works by causing your muscles tissues to dialate or something like that. My doctor explained taking too many in too short a time could cause a stroke or heart attack, forget which exactly. One side effect i get is my skin becoming highly sensitive to heat. We’re talking luke warm shower water feeling something like scalding hot. It’s not that exactly either, very weird sensation. Other times my throats tensed up similar to when you eat something highly sour.
We do this pretty often for the patients that come into our student run clinic. We aren't allowed to prescribe opioids, so we tell them to alternate ibuprofen and acetaminophen every 4 hours. Works pretty well, and doesn't stress your liver or stomach as hard.
Same. In the hospital I was given small doses of morphine, and frankly I was shocked at how well it worked. I've had demerol for kidney stones, and it didn't do much for pain.
But the morphine at the hospital was like magic. And the dose low enough I didn't really feel any other effects.
That said, when it was time for discharge, the doc told me to alternate tylenol and advil every 2 hours (4 hour cycles each), as needed.
It wasn't news to me. I've followed the protocol before. I wasn't really in much pain by the time I was discharged, so I didn't bother with it this time and can't really compare.
They didn't say opioids are no better than acetaminophen+ibuprofen, but codeine, which is weak enough to be freely available OTC in many countries.
Anyone doubting the merits of opioids in pain control should take a look at https://en.wikipedia.org/wiki/Equianalgesic - many of the voices in this debate will sorely regret their remarks if they ever experience real pain, which most people will at some point.
Acetaminophen and ibuprofen are safe and effective together.
The label you refer to advises against using other medicines that contain acetaminophen, as many cold and allergy medicines do (Excedrin, NyQuil, Robitussin).
The thing you want to look out for are not doubling up acetaminophen, and not taking any combination of aspirin + naproxen + ibuprofen.
Ibuprofen can cause liver damage in higher doses. It appears to happen almost randomly though, which suggests something unusual to the patient prompts the reaction.
No, you wouldn't be crazy. You'd simply be following medical advice/what's best for your situation. For some chronic pain sufferers opioids are one of the only options (or is something that is used in addition to other methods/things to alleviate pain). For instance, many people with connective tissue disorders use opioids in addition to other physical methods (surgical, splints, etc)[1], and removing something like an opioid can make life untenable, and amounts to torture [2]
Those opioid doses are all super low, roughly equivalent to a single Tylenol 3. The alternative is a super high dose of acetaminophen. 1/4 your daily recommended maximum. At roughly 3x the acetaminophen + the fairly high dose ibuprofen I don't think there is anything really surprising about this.
You couldn't take that acetaminophen dosage for more than 8 hours with 2 hour dosing without hitting your daily maximum. I'm skeptical that opioid alternative with such a low dosage over such a short period of time has any real chance of being addition forming.
These are standard doses of all these medications. Its the dose of tylenol often used in the hospital and wasn't dosed every 2 hours it was dosed once. For the opiates we either give 1 or 2 pills, here they gave 1. Perfectly reasonable.
OTC standard dose for regular strength Tylenol is 1-2 capsules x 325mg. They are giving the patients 1000mg or the equivalent of two extra strength pills (500mg). While both are 'standard' doses, I think the poster's point is that they're comparing 'regular strength' opiates (5mg of oxy/hydrocodone) with extra strength acetaminophen (1000mg acetaminophen). If they wanted a proper comparison, they should compare 7.5 or 10mg of oxy/hydrocodone with 1000mg of acetaminophen. Also, because the oxy/hydrocodone pills they test also contain acetaminophen you'd think they'd test the efficacy of oxy/hydrocodone by themselves as well, but apparently that didn't cross their minds. It definitely looks to me like the combinations tested were chosen so as to get a predetermined result.
I'm not saying they are unreasonable doses but they are definitely low as far as opioid doses go. Apart from T1/T2s you can't get lower afaik.
My point is I don't see that replacing opioids in this case is really useful. I'm happy to admit I don't know the answer here but I'm skeptical that people going to the hospital and getting a single 5mg percocet/vicodin or even a 3-4 over ~8-12 hours are really at risk of addiction.
For 24/7 dosing that acetaminophen/ibuprofen combo is only safe once every 6 hours which from my experience is way too long for acetaminophen. Even on every 4 hours I find the last 1 hour is definitely very noticeable.
The median pain level after treatment was above "Distressing" (Pain level 4). That's not reasonable. It is unethical. And probably why the study was run in the Bronx rather than someplace like Manhattan where people are far more likely to have the means to get what they want and to do something about shoddy treatment.
Well lets take some of these folks and give them a herniated disk like I had. Advil? Tylenol? Sure - like Skittles. Even high doses of Hydrocodone only kept the debilitating pain away for a couple of hours.
I only slept 3 hours a night for 2 month. My neurosurgeon said - "When you've reached your pain limit call me and we'll schedule surgery". That was 2 months.
I'm very grateful for both the narcotics and the neurosurgeon. Surgery was the last resort and thankfully it reduced my pain 95% (micro discectomy).
Some years later I was umpiring and tripped and fell right on my ribs (I'm 230 lbs) - crackity crack. Breathing would not have been possible without a good dose of Percocet - a limited, appropriate amount.
So not sure exactly what's going on with this study (and I think the hysterical press has some factor) but I'd debate the results.
There’s no worse pain than passing a kidney stone. Ibuprofen + acetaminophen works better than anything I’ve ever been prescribed. If it hasn’t worked for you, you might not have taken enough. Ask your doctor about the dosage. It’s safe to take more than what is recommended on the bottle.
"Pain" is a very difficult thing to nail down. It is a physical thing but also a psychological issue. The same physical pain, an identical injury, can manifest completely differently according to the patient's mental state. That's why VR games reduce pain in children undergoing painful treatments. That's why someone with severe chest pain can see it suddenly diminish once the doc rules it's not heart attack.
An opiod hits the mental half in a way the others do not. If you are in hospital with a compound fracture (bone sticking out of you) then you aren't just in severe pain but are also absolutely terrified. Opiods work in such cases. Within a minute you will be very happy. Advil might help with the physical pain but it won't put your mind in the same place.
I don't get the US stance on opioids. In Germany they are heavily regulated and can't be obtained without special prescription giving them an rather exclusive aura. No German doctor would prescribe them for headaches and people only really get them after serious surgery for a really short term. Advil (Ibuprofen) and Aspirin (ASS) are far more common here and used for pain management at a far broader extent than in the US. And frankly so, Germany doesn't have an opioid problem.
That said, I think Bayer (manufacturer of Aspirin) being a German company could have something to do with that, on the other hand seeing the immense money spent on lobbying by Opioid companies in the US really says a lot. IIRC Purdue even paid university professors to downplay risks of Oxy in front of their students so they would get a biased view on them already.
Your view looking into the US may be a little flawed, to be honest. Opioids are also regulated in the US. No one gets them for headaches. Doctors recommend Tylenol and Advil for most aches and pain.
The times when my wife and I have received Opioids: broken ankles, back injuries from weight lifting, and after c-sections. I didn't receive them when I broke my collarbones (I've broken both, on separate occasions).
> I think Bayer (manufacturer of Aspirin) being a German company...
Tylenol is produced by a huge American company: Johnson and Johnson. Advil is produced by another huge American company: Pfizer.
I get fiorecet for migraines after the doctor tried me out on a few other preventative medications which either didn't work or had side effects like making me as sleepy as taking two Benadryl.
There as needed and I can go months between refilling the script sometimes but it's still for headaches
I mean, I get migraines too, and they're completely debilitating, but I would personally just classifiy them as something very different than a headache. Undersells just how horrible they can be.
Yea, wasnt sure if the OP was including them or not. Some people do when they say "headaches". If I dont take any medication before getting a migraine and it goes all the way I am incapable of even moving
Bayer is the original manufacturer and trademark holder for Heroin, so I imagine they could have entered the opioid game if they wanted to. However, they might still remember the 100 years old lesson of what comes from marketing opioids to the general population.
"And frankly so, Germany doesn't have an opioid problem."
You are very uninformed obviously. As far as i know for my town, Paderborn (NRW), we have about 1.000 people receiving opioid replacement drugs under government supervision (~90.000 city population).
> As far as i know for my town, Paderborn (NRW), we have about 1.000 people receiving opioid replacement drugs under government supervision (~90.000 city population).
While opioid abuse is rising, yes even in Germany, situations are not really comparable. In the US 20.5 Million people have a substance abuse disorder. Of which 2M have a problem involving prescription pain relievers, and roughly 600k people are addicted to Heroin. [0] For Germany data on this matter is generally less available, but reports range from 1.5M to 1.9M users of prescription drugs for Germany, that number includes sleep-aids and Benzos as well though. Zolpidem based drugs actually make up for 3/4 of German prescription drug abuse. [1] The official drug report mentions 160k high-risk opioid users and 77k in substitution programmes. [2] (That's actually far far less than the 1/90 rate you report for your city. Talking about uninformed...)
Also for comparison of the problem, let's look at the death rates in the US [3] and Germany [2]: 33k vs 1.2k now in relation to the population (age 15-64):
US: 0.000160 %
Germany: 0.0000226415 %
US death rate is 7 times higher than the German, while population is only 4 times bigger.
That said, a look at the opioid users in Germany (160k) and US (2M+600k) is way clearer. We are talking about 16 times the abuse rate in the US compared to Germany. So yeah, Germany doesn't have an opioid problem, compared to the US.
So while Germany has heroin addicts, the US actually has a drug addict training program running. In the US there are 290M opioid prescriptions per year. [4]
And while Germany doesn't have those outstanding numbers, Big Pharma is pushing for change in Germany [5 (German)]
The title is misleading, because opioids clearly are better at treating severe pain. I'm not familiar with the particular combination researched here, but Ibuprofene alone certainly doesn't cut it in many instances. On the other hand, I can't understand why doctors in the US are so happy to prescribe opioids.
In veterinary medicine it's slightly different, because we can't use ibuprofene for dogs and cats, but something similar. Still, opioids are a good idea perioperatively, and addiction is at worst a transient problem. The dog can't go out and score some heroin, for instance.
I was hospitalized with a huge abscess that was damaging my leg and hitting my sciatic nerve. The pain was as acute as I would imagine is possible. The morphine drip that I had did nothing. It was very frustrating. Sometimes the pain would re-occur before I was allowed to get more morphine, and the duration/severity of the pain was comparable.
At the time, I thought that the morphine only managed to make me tired after the pain had subsided, but maybe taking a nap after that kind of pain was normal anyways?
As someone who actually ended up in ER with a badly broken ankle once, I beg to differ. After surgery, Percocet was the only reason I could sleep for the first few days. I got off it as soon as I could, though.
Edit: I just wanted to point out there are different degrees of “acute extremity pain”. There’s “I bumped my toe against a chair leg” kind, and then there’s “I can’t breathe because I’m in shock” kind. Opioids are appropriate for the latter.
The other fun thing is that opioids are often cut with ibuprofen or acetaminophen. So even if you are taking an opioid for chronic pain, you might still be getting a long-term dose of Tylenol, which can damage your liver.
Would like to have seen an opioid-ibuprofen combo in the mix. Or ibuprofen and acacetamenophine each alone. For the class of injury described, swelling and inflamation will be very common, and ibuprofen is better suited than acetamenophine for this.
Class of injury is very important too: limb injuries producing acute pain are more likely to be a type where time, even just 2 hours, will have a leveling effect on pain, while one class or combination of drugs might provide better instant relief.
Finally, we have these short term acute pain examples and long term chronic pain, but medium term acute pain in the range of days to weeks might be a primary area of risk for new addictions where a patient requires more than a few doses but doesn't ask the patient to shift their outlook on how they deal with pain and adjust to it that chronic pain patient may have to do, with or without opiods. If the pain is short term in this way, the potent opioid pills can be seen as a quick fix that doesn't take as much effort as rethinking "acceptable" levels of pain.
I guarantee many of you who advocate for basically getting rid of opiates completely as an option for pain management, will be singing an entirely different tune if you ever end up in real pain and realize that "tylenol and advil" isn't going to cut it.
Researchers then randomly assigned the patients to get one of four pain-pill combinations: 400mg of ibuprofen and 1,000mg of acetaminophen; 5mg of oxycodone and 325mg of acetaminophen; 5mg of hydrocodone and 300mg of acetaminophen; or 30mg of codeine and 300mg of acetaminophen. Each of the pill combinations looked identical to the patients—three opaque capsules.
The dosages contain very little of each opiod. Based on Googling "normal dose of oxycodone" 5mg is the smallest available dose of oxycodone and half the size of the smallest dose of it under the brand name Oxycotoin. In addition each opiod cocktail contains less acetaminophen than in the non-opiod control.
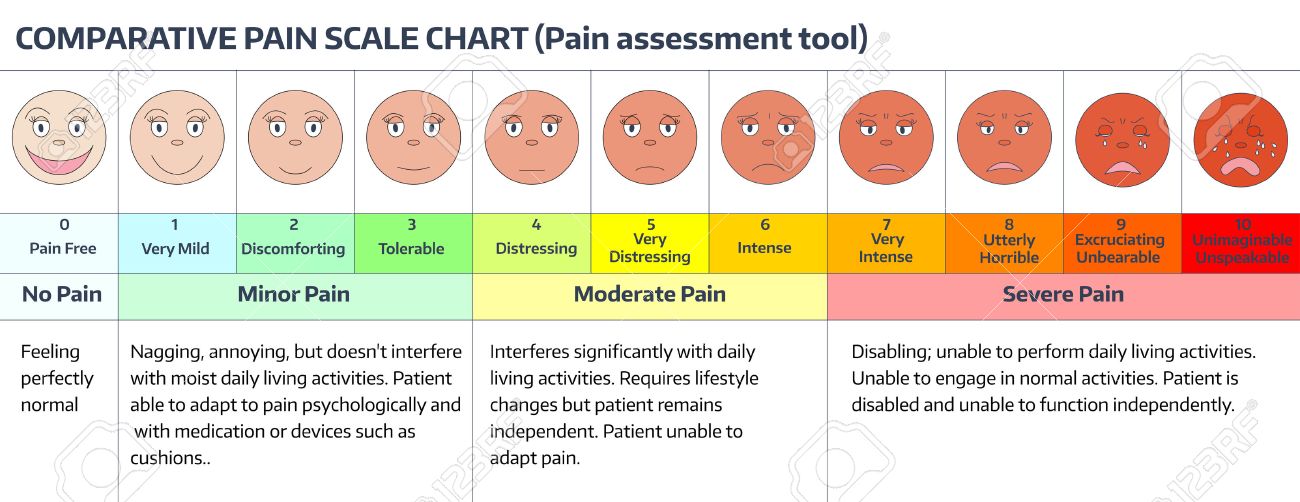
It's worth noting that the standard pain scale goes from zero to ten and that a mean of 8.7 across 411 patients is very high: closer to "Excruciating Unbearable" than "Utterly Horrible" [1]. Reducing it to 4.3 is to take it down between "Distressing" and "Very Distressing".
None of the treatments reduced the pain to "Tolerable" (level 3). One might say that the study shows that an inadequate cocktail of opoids is no better than an inadequate cocktail without them.
The headline here says the study "finds opioids no better", but what actually happened is that the study was too small to reach statistical significance on any of its endpoints.
More importantly, the study chose the top of the recommended dose range for the ibuprofen+acetaminophen group but the bottom of the recommended dose ranges for the oxycodone+acetaminophen, hydrocodone+acetaminophen, and codeine+acetaminophen groups. This strongly suggests that the study designers knew what outcome they wanted, and arranged subtle details of the study (which are hidden behind a paywall!) to make sure they got it.
This is a highly misleading presentation of the study.
The study compared the following doses:
— 400 mg ibuprofen and 1,000 mg acetaminophen
— 5 mg oxycodone and 325 mg acetaminophen
— 5 mg hydrocodone and 300 mg acetaminophen; or
— 30 mg codeine and 300 mg acetaminophen
So, the study is comparing high doses of ibuprofen/acetaminophen to low doses on opiates/acetaminophen.
It is an interesting outcome for mild pain and suggest that for mild pain it might be better to pass on low dose opiates but in no way does this show that opiates are not needed for severe pain.
400 mg ibuprofen and 1000 mg acetaminophen aren't high doses, at least when taken separately, they're pretty standard adult doses (I think those are also the most common pill dosages.)
Maximum single does of standard release acetaminophen is 1000 mg. Make no mistake, that is a high dose and it's terrible for your liver. That's why in recent years, there are more and more 325 mg preparations (where an adult takes 2 x 325) rather than the traditional 2 x 500 mg.
an initial prescription of just a few days' worth of pills can trap patients into using the highly addictive, often deadly drugs for a year or more
I call BS on this. Maybe if you have an unresolved underlying chronic pain, this could be true. But many people get a hydrocodone prescription after surgery or dental work and do not go on to become addicts.
And no, Tylenol is not great for acute pain. It does very little for me in fact. Ibuprofen or aspirin work better in my experience.
I've met a few people who got addicted to pain killers at 15/16 years old. It started with a small prescription after dental surgery or similar, their parents left them to their own devices to take meds as needed. When the prescription was up they then went out and bought it on the street because they wanted the feeling to keep going. Some people are simply vulnerable, and even a little temptation is too much.
Can you link to the studies that you've performed that demonstrate this? Because there havebeen multiple discussions on this site where studies have proven that people _do_ get addicted over short term, unnecessary high doses.
>According to the large, annually repeated and representative National Survey on Drug Use and Health, 75 percent of all opioid misuse starts with people using medication that wasn’t prescribed for them—obtained from a friend, family member or dealer. And 90 percent of all addictions—no matter what the drug—start in the adolescent and young adult years.
>A Cochrane review of opioid prescribing for chronic pain found that less than one percent of those who were well-screened for drug problems developed new addictions during pain care; a less rigorous, but more recent review put the rate of addiction among people taking opioids for chronic pain at 8-12 percent.
The study that most people reference in this setting[1] simply associates days of opioid usage to likelihood of using opioids in the long term. A simple (and very likely) explanation is that people who need opioids for ten days are likely suffering from chronic pain.
Toradol (NSAID) is the most effective pain killer I've experienced. I broke a rib and could barely move. ER injected me with Toradol, and for a brief few hours I could move normally. I call that the best high I've ever had -- not a buzz -- just absence of pain. Unfortunately it's so bad for your stomach they won't give you two shots and won't let you take it orally more than a few days.
Personally I'd rather take the opiates. I have GERD and other GI problems. Ibuprofen is likely to lead to extreme pain and discomfort. I've taken a variety of opiates in the past. They did work for reducing pain but I couldn't wait to stop. I hate the dopey feeling.
I'm sure this is true for the pain associated with the various ailments that bring most people to the ER, but opioids are massively more effective for serious trauma. Motrin does very little for people who've been shot. Fentanyl lollipop on the other hand....
I find that really hard to believe. Maybe for some kinds of pain OTC meds or marijuana will cut it, but when I have really bad back pain nothing works as well as opiates, not muscle relaxers, not tylenol, not even close. Opiates work like magic.
I broke my arm a decade or so ago. The doctor wasn't able to set my bone without relaxing my extremely tight muscles. Morphine worked great for that. I sincerely doubt that an NSAID could have done this, or even something like a Soma (Carisoprodol).
Same thing happened when I dislocated my shoulder last year. No NSAID could have done what that morphine did. They tried for about 10min to do it without the morphine but it was just simply not happening. After the morphine they actually had to put my shoulder back in twice since it popped right back out after the first attempt.
Isn't it well-known? It is written on ketorolak informational sheet.
edit: oh, I see, article is about ibuprofen and acetaminophen. The point stands, non-opioid paikillers have same effectiveness
Yeah they cause bleeding though so dont expect advil if you come in with a bullet wound. Hopefully we can stop giving opioids for non bleeding injuries with this study.
Yeah, look, I staggered into the ER with a shattered collar-bone and a shitload of missing skin, and 10 mg of oxy had me feeling pretty much FINE while a nurse took a coarse sponge to scrub the asphalt out of my wounds.
Overprescribed, yes. Comparable to OTC? Absolutely fucking not. Claiming that ibuprofen is as effective as diluadid or morphine is completely disingenuous.
Your anecdote is irrelevant - the study only tested extremity pain, a collar bone is not an extremity.
They only tested drug combinations as well, not a single medication.
I presume, from your comment, you also weren't given the 400mg of ibuprofen and 1,000mg of acetaminophen combination first and then an opioid only because that wasn't enough pain relief.
And while we are swapping anecdotes, I was given hydrocodone for an acute extremity injury (leg) and the only noticeable thing it did for me was make me feel really, really nauseous. If it did help with the pain it was hard to tell because of the nausea.
Acute pain from injury? Give me opioids. Post-surgical pain while in hospital? Opioids. Released from hospital? Opioids probably shouldn't be prescribed.
{kind=link}
On example that made an impression on me: a couple of years ago, I had arthroscopic surgery on a knee. When the surgery was done and I was being discharged, a nurse came to me with a percocet script and told me to take one every xx hours. Having taken percocet in the past and being familiar with the aforementioned side-effects, I asked her if she wanted me to take it for pain management, or if there was another reason to take it (blocking the formation of blood clots for example). I'm fairly pain-tolerant, so if it was a pain management thing, I wasn't going to take it. Her response was "just take the pills." That was not helpful. If doctors and nurses are just shoving these things down patients' throats it's not surprising there is a problem out there.